

Metronomic Chemo-Endocrine Therapy (FulVEC) as a Salvage Treatment for Patients with Advanced, Treatment-Refractory ER+/HER2-Breast Cancer—A Retrospective Analysis of Consecutive Patients Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
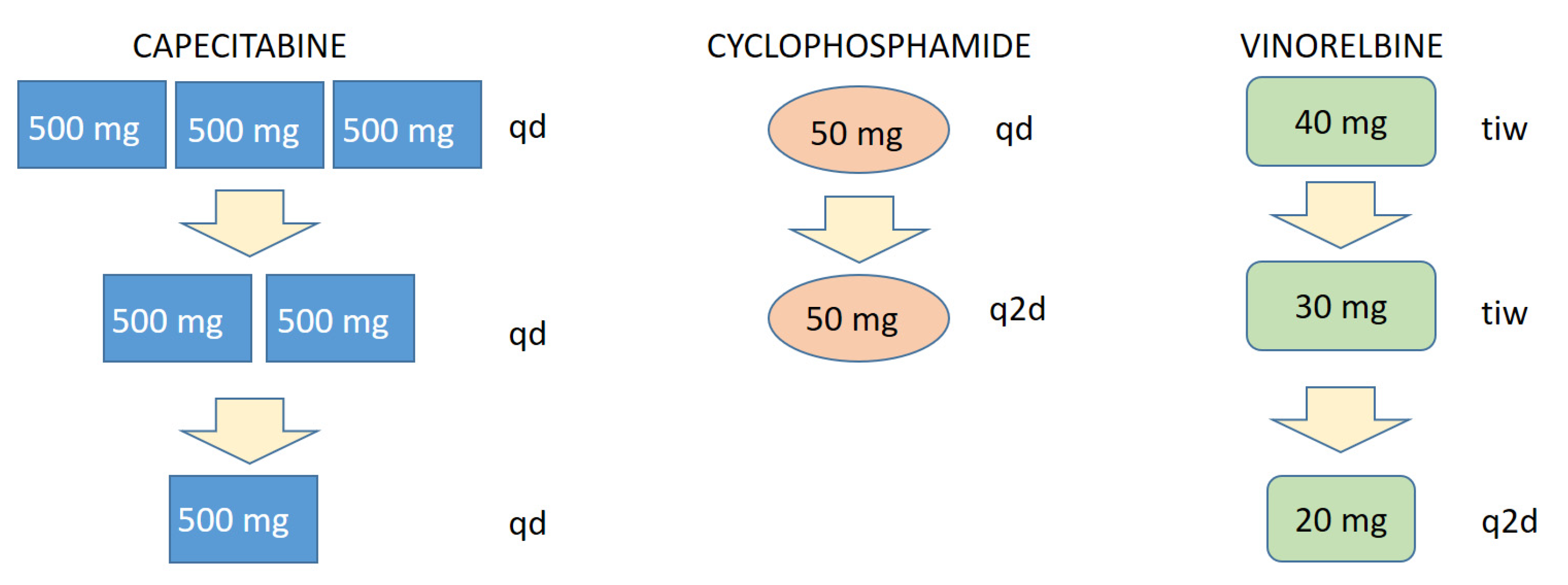
2.2. Treatment
2.3. Analysis of Treatment Efficacy
2.4. Safety Analysis
2.5. Statistical Considerations
3. Results
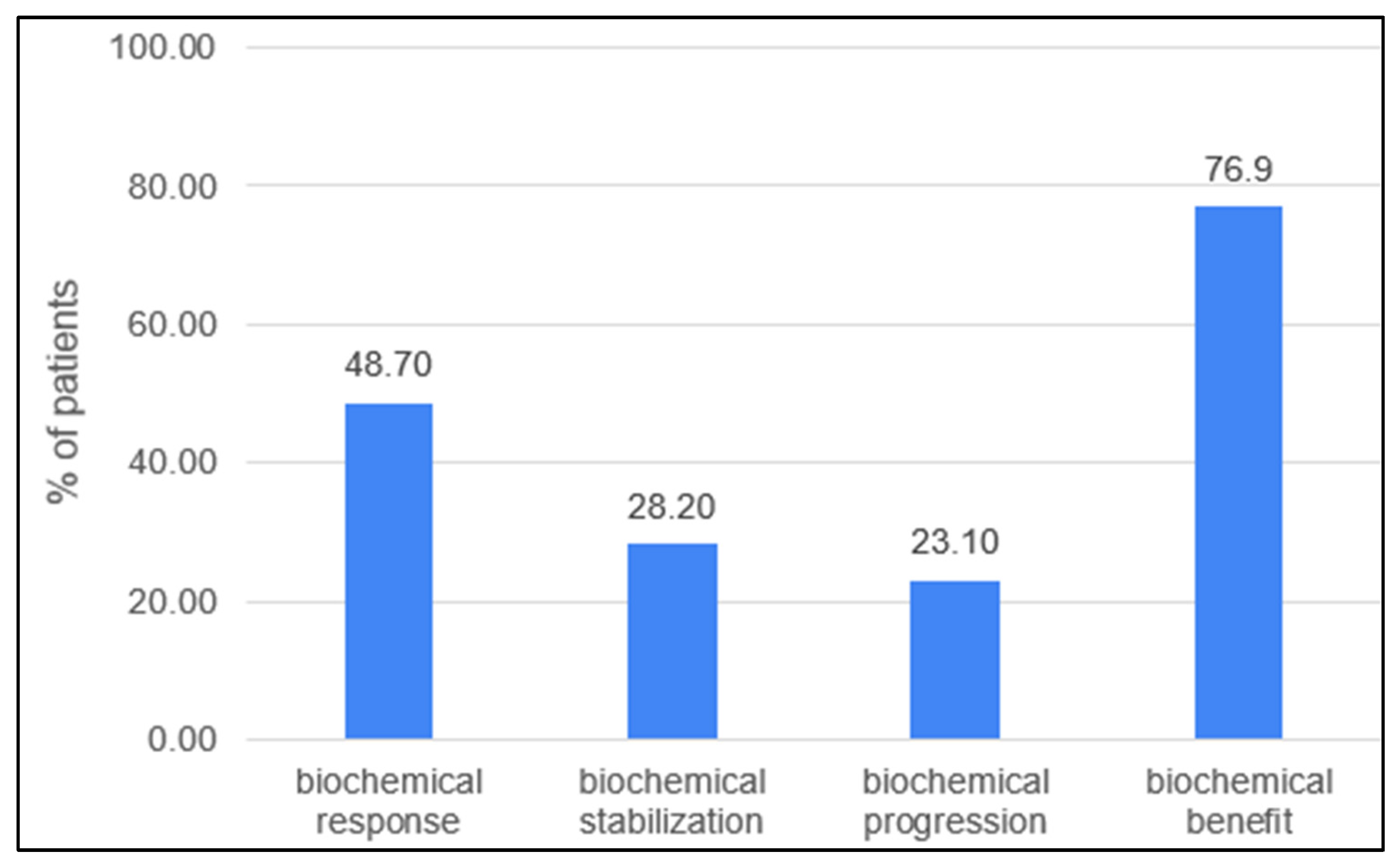
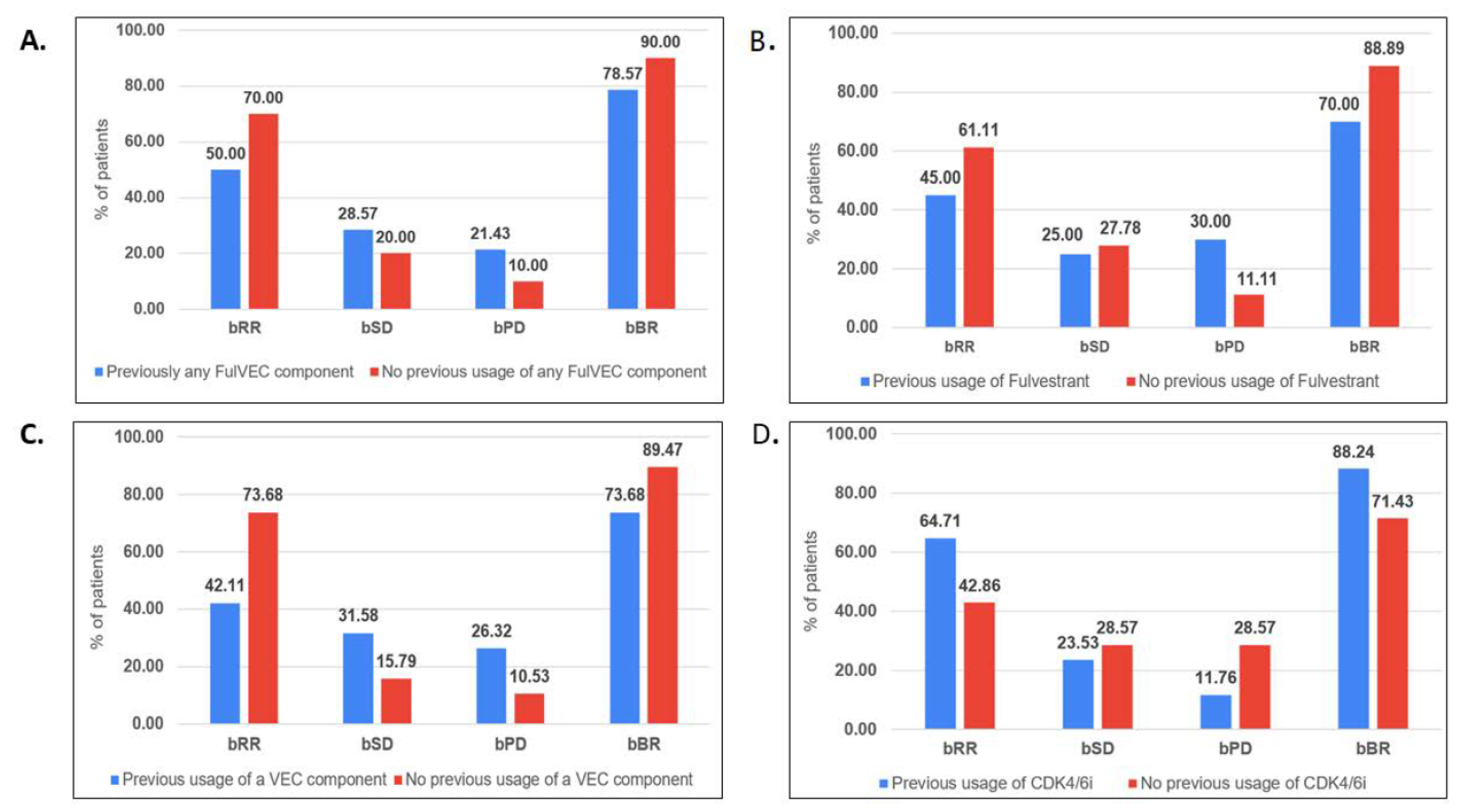
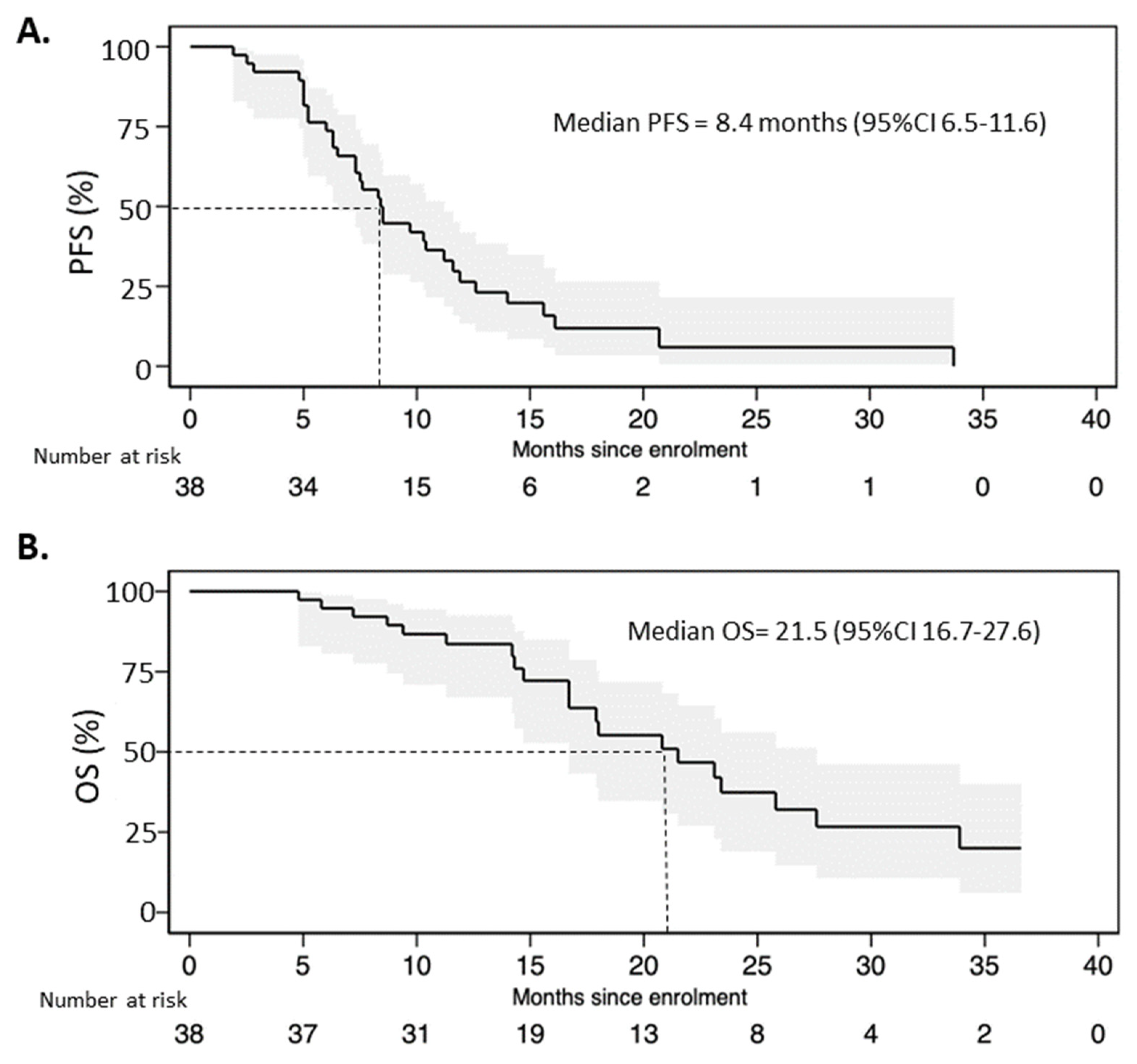
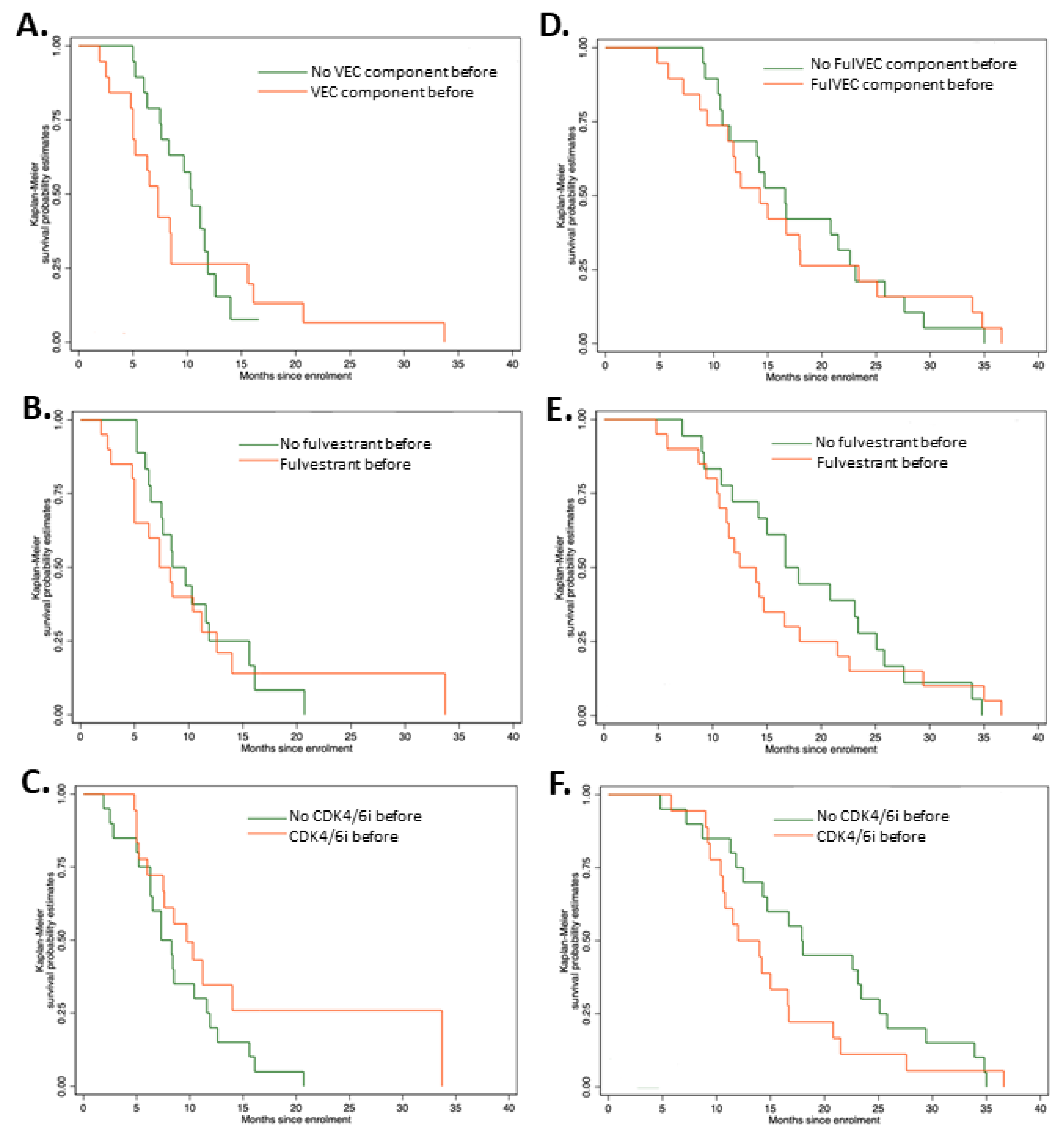
3.1. Efficacy
3.2. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Redig, A.J.; Mcallister, S.S. Breast Cancer as a Systemic Disease: A View of Metastasis. J. Intern. Med. 2013, 274, 113. [Google Scholar] [CrossRef] [PubMed]
- Rozeboom, B.; Dey, N.; De, P. ER+ Metastatic Breast Cancer: Past, Present, and a Prescription for an Apoptosis-Targeted Future. Am. J. Cancer Res. 2019, 9, 2821. [Google Scholar] [PubMed]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, C.; Barberis, M. Breast Cancer Heterogeneity. Diagnostics 2021, 11, 1555. [Google Scholar] [CrossRef]
- Cazzaniga, M.; Cordani, N.; Capici, S.; Cogliati, V.; Riva, F.; Cerrito, M. Metronomic Chemotherapy. Cancers 2021, 13, 2236. [Google Scholar] [CrossRef]
- Cazzaniga, M.E.; Munzone, E.; Bocci, G.; Afonso, N.; Gomez, P.; Langkjer, S.; Petru, E.; Pivot, X.; Sánchez Rovira, P.; Wysocki, P.; et al. Pan-European Expert Meeting on the Use of Metronomic Chemotherapy in Advanced Breast Cancer Patients: The PENELOPE Project. Adv. Ther. 2019, 36, 381–406. [Google Scholar] [CrossRef]
- Wysocki, P.J.; Lubas, M.T.; Wysocka, M.L. Metronomic Chemotherapy in Prostate Cancer. J. Clin. Med. 2022, 11, 2853. [Google Scholar] [CrossRef]
- André, N.; Banavali, S.; Snihur, Y.; Pasquier, E. Has the Time Come for Metronomics in Low-Income and Middle-Income Countries? Lancet Oncol. 2013, 14, e239–e248. [Google Scholar] [CrossRef]
- Cazzaniga, M.E.; Pinotti, G.; Montagna, E.; Amoroso, D.; Berardi, R.; Butera, A.; Cagossi, K.; Cavanna, L.; Ciccarese, M.; Cinieri, S.; et al. Metronomic Chemotherapy for Advanced Breast Cancer Patients in the Real World Practice: Final Results of the VICTOR-6 Study. Breast 2019, 48, 7–16. [Google Scholar] [CrossRef]
- Cazzaniga, M.E.; Cortesi, L.; Ferzi, A.; Scaltriti, L.; Cicchiello, F.; Ciccarese, M.; della Torre, S.; Villa, F.; Giordano, M.; Verusio, C.; et al. Metronomic Chemotherapy with Oral Vinorelbine (MVNR) and Capecitabine (MCAPE) in Advanced HER2-Negative Breast Cancer Patients: Is It a Way to Optimize Disease Control? Final Results of the VICTOR-2 Study. Breast Cancer Res. Treat. 2016, 160, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Montagna, E.; Bagnardi, V.; Cancello, G.; Sangalli, C.; Pagan, E.; Iorfida, M.; Mazza, M.; Mazzarol, G.; Dellapasqua, S.; Munzone, E.; et al. Metronomic Chemotherapy for First-Line Treatment of Metastatic Triple-Negative Breast Cancer: A Phase II Trial. Breast Care 2018, 13, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Fedele, P.; Marino, A.; Orlando, L.; Schiavone, P.; Nacci, A.; Sponziello, F.; Rizzo, P.; Calvani, N.; Mazzoni, E.; Cinefra, M.; et al. Efficacy and Safety of Low-Dose Metronomic Chemotherapy with Capecitabine in Heavily Pretreated Patients with Metastatic Breast Cancer. Eur. J. Cancer 2012, 48, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, M.E.; Torri, V.; Villa, F.; Giuntini, N.; Riva, F.; Zeppellini, A.; Cortinovis, D.; Bidoli, P. Efficacy and Safety of the All-Oral Schedule of Metronomic Vinorelbine and Capecitabine in Locally Advanced or Metastatic Breast Cancer Patients: The Phase I-II VICTOR-1 Study. Int. J. Breast Cancer 2014, 2014, 769790. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lu, J.; Leaw, S.; Hong, X.; Wang, J.; Shao, Z.; Hu, X. An All-Oral Combination of Metronomic Cyclophosphamide plus Capecitabine in Patients with Anthracycline- and Taxane-Pretreated Metastatic Breast Cancer: A Phase II Study. Cancer Chemother. Pharm. 2012, 69, 515–522. [Google Scholar] [CrossRef]
- Taguchi, T.; Nakayama, T.; Masuda, N.; Yoshidome, K.; Akagi, K.; Nishida, Y.; Yoshikawa, Y.; Ogino, N.; Abe, C.; Sakamoto, J.; et al. Study of Low-Dose Capecitabine Monotherapy for Metastatic Breast Cancer. Chemotherapy 2010, 56, 166–170. [Google Scholar] [CrossRef]
- Munzone, E.; Regan, M.M.; Cinieri, S.; Montagna, E.; Orlando, L.; Shi, R.; Campadelli, E.; Gianni, L.; De Giorgi, U.F.F.; Bengala, C.; et al. A Randomized Phase II Trial of Metronomic Oral Vinorelbine plus Cyclophosphamide and Capecitabine (VEX) vs Weekly Paclitaxel (P) as First- or Secon... | OncologyPRO. In Proceedings of the ESMO Annual Meeting; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Schwartzberg, L.S.; Wang, G.; Somer, B.G.; Blakely, L.J.; Wheeler, B.M.; Walker, M.S.; Stepanski, E.J.; Houts, A.C. Phase II Trial of Fulvestrant with Metronomic Capecitabine for Postmenopausal Women with Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer. Clin. Breast Cancer 2014, 14, 13–19. [Google Scholar] [CrossRef]
- Aurilio, G.; Munzone, E.; Botteri, E.; Sciandivasci, A.; Adamoli, L.; Minchella, I.; Esposito, A.; Cullurã, D.; Curigliano, G.; Colleoni, M.; et al. Oral Metronomic Cyclophosphamide and Methotrexate Plus Fulvestrant in Advanced Breast Cancer Patients: A Mono-Institutional Case-Cohort Report. Breast J. 2012, 18, 470–474. [Google Scholar] [CrossRef]
- Rashad, N.; Abdelhamid, T.; Shouman, S.A.; Nassar, H.; Omran, M.A.; El Desouky, E.D.; Khaled, H. Capecitabine-Based Chemoendocrine Combination as First-Line Treatment for Metastatic Hormone-Positive Metastatic Breast Cancer: Phase 2 Study. Clin. Breast Cancer 2020, 20, 228–237. [Google Scholar] [CrossRef]
- Mayer, E.L.; Ren, Y.; Wagle, N.; Ma, C.; DeMichele, A.; Cristofanilli, M.; Meisel, J. Palbociclib after CDK4/6i and Endocrine Therapy (PACE): A Randomized Phase II Study of Fulvestrant, Palbociclib, and Avelumab for Endocrine Pre-Treated ER+/HER2- Metastatic Breast Cancer. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 6–10 December 2022. [Google Scholar]
- Tao, J.J.; Blackford, A.L.; Nunes, R.; Truica, C.I.; Mahosky, J.; Jones, M.K.; Leasure, N.C.; Cescon, T. Phase II Trial of Palbociclib with Fulvestrant in Individuals with Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer with Disease Progression after Palbociclib with an Aromatase Inhibitor. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 6–10 December 2022. [Google Scholar]
- Sledge, G.W., Jr.; Toi, M.; Neven, P.; Sohn, J.H.; Inoue, K.; Pivot, X.; Okera, M.; Masuda, N.; Kaufman, P.A.; Koh, H.; et al. Final overall survival analysis of Monarch 2: A phase 3 trial of Abemaciclib plus Fulvestrant in patients with hormone receptor-positive, HER2-negative advanced breast cancer. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 6–10 December 2022. [Google Scholar]
- Lu, Y.S.; Im, S.A.; Colleoni, M.; Franke, F.; Bardia, A.; Cardoso, F.; Harbeck, N.; Hurvitz, S.; Chow, L.; Sohn, J.; et al. Updated Overall Survival of Ribociclib plus Endocrine Therapy versus Endocrine Therapy Alone in Pre- and Perimenopausal Patients with HR+/HER2- Advanced Breast Cancer in MONALEESA-7: A Phase III Randomized Clinical Trial. Clin. Cancer Res. 2022, 28, 851–859. [Google Scholar] [CrossRef]
- Neven, P.; Fasching, P.A.; Chia, S.; Jerusalem, G.; Laurentiis, M.; Im, S.; Petrakova, K.; Bianchi, G.V.; Martin, M.; Nusch, A.; et al. LBA4 Updated Overall Survival (OS) Results from the First-Line (1L) Population in the Phase III MONALEESA-3 Trial of Postmenopausal Patients (PTS) with HR+/HER2− Advanced Breast Cancer (ABC) Treated with Ribociclib (RIB) + Fulvestrant (FUL). Ann. Oncol. 2022, 33, S194. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | N (%) |
|---|---|
| Number of patients | 38 |
| Median age (range) | 46 years (30–80) |
| Menopausal status | |
| Premenopausal | 15 (39%) |
| Postmenopausal | 24 (61%) |
| Previous neo/adjuvant chemotherapy | 24 (63%) |
| Previous adjuvant endocrine therapy | 23 (61%) |
| Locoregional relapse | 11 (29%) |
| Disseminated disease | 39 (100%) |
| Bone metastasis | 31 (82%) |
| Bone-only disease | 3 (7.7%) |
| Lung metastasis | 13 (34%) |
| Liver metastasis | 25 (66%) |
| CNS metastasis | 3 (8%) |
| No. of previous systemic treatments | 2 (median) |
| ≤2 | 20 (53%) |
| 3–4 | 8 (21%) |
| ≥5 | 10 (26%) |
| Previously any FulVEC component | 30 (77%) |
| Fulvestrant | 20 (53%) |
| Vinorelbine | 11 (29%) |
| Cyclophosphamide | 12 (32%) |
| Capecitabine | 13 (34%) |
| Previous treatment with CDK4/6i | 18 (47%) |
| 1st line | 10 (59%) |
| ≥1st line | 7 (41%) |
| Adverse Events | Any Grade | G3 | G4 |
|---|---|---|---|
| Any adverse event | 51.3% | 38.5% | 10.3% |
| Neutropenia | 41.0% | 15.4% | 10.3% |
| Anemia | 12.8% | 5.1% | 0% |
| Thrombocytopenia | 2.5% | 0% | 0% |
| Fatigue | 7.7% | 2.6% | 0% |
| Hfs | 12.8% | 2.5% | 0% |
| Hepatotoxicity | 5.1% | 2.5% | 0% |
| Abdominal pain | 2.5% | 2.5% | 0% |
| Toxicity-Related Treatment Decisions | % (N) |
|---|---|
| Dose reduction | 46% (18) |
| Myelotoxicity | 80% |
| H&F syndrome | 15% |
| Other | 5% |
| Temporary treatment interruption | 23% (9) |
| Myelotoxicity | 70% |
| H&F syndrome | 25% |
| Other | 5% |
| Permanent treatment cessation due to AE | 0% (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buda-Nowak, A.; Kwinta, Ł.; Potocki, P.; Michałowska-Kaczmarczyk, A.; Słowik, A.; Konopka, K.; Streb, J.; Koniewski, M.; Wysocki, P.J. Metronomic Chemo-Endocrine Therapy (FulVEC) as a Salvage Treatment for Patients with Advanced, Treatment-Refractory ER+/HER2-Breast Cancer—A Retrospective Analysis of Consecutive Patients Data. J. Clin. Med. 2023, 12, 1350. https://doi.org/10.3390/jcm12041350
Buda-Nowak A, Kwinta Ł, Potocki P, Michałowska-Kaczmarczyk A, Słowik A, Konopka K, Streb J, Koniewski M, Wysocki PJ. Metronomic Chemo-Endocrine Therapy (FulVEC) as a Salvage Treatment for Patients with Advanced, Treatment-Refractory ER+/HER2-Breast Cancer—A Retrospective Analysis of Consecutive Patients Data. Journal of Clinical Medicine. 2023; 12(4):1350. https://doi.org/10.3390/jcm12041350
Chicago/Turabian StyleBuda-Nowak, Anna, Łukasz Kwinta, Paweł Potocki, Anna Michałowska-Kaczmarczyk, Agnieszka Słowik, Kamil Konopka, Joanna Streb, Maciej Koniewski, and Piotr J. Wysocki. 2023. "Metronomic Chemo-Endocrine Therapy (FulVEC) as a Salvage Treatment for Patients with Advanced, Treatment-Refractory ER+/HER2-Breast Cancer—A Retrospective Analysis of Consecutive Patients Data" Journal of Clinical Medicine 12, no. 4: 1350. https://doi.org/10.3390/jcm12041350