

Routine Use of a Pocket-Sized Handheld Echoscopic Device Plus a Biomarker by Emergency Medicine Residents with an Early Screening Algorithm for Suspected Type A Acute Aortic Syndrome
Abstract
:1. Introduction
2. Materials and Methods
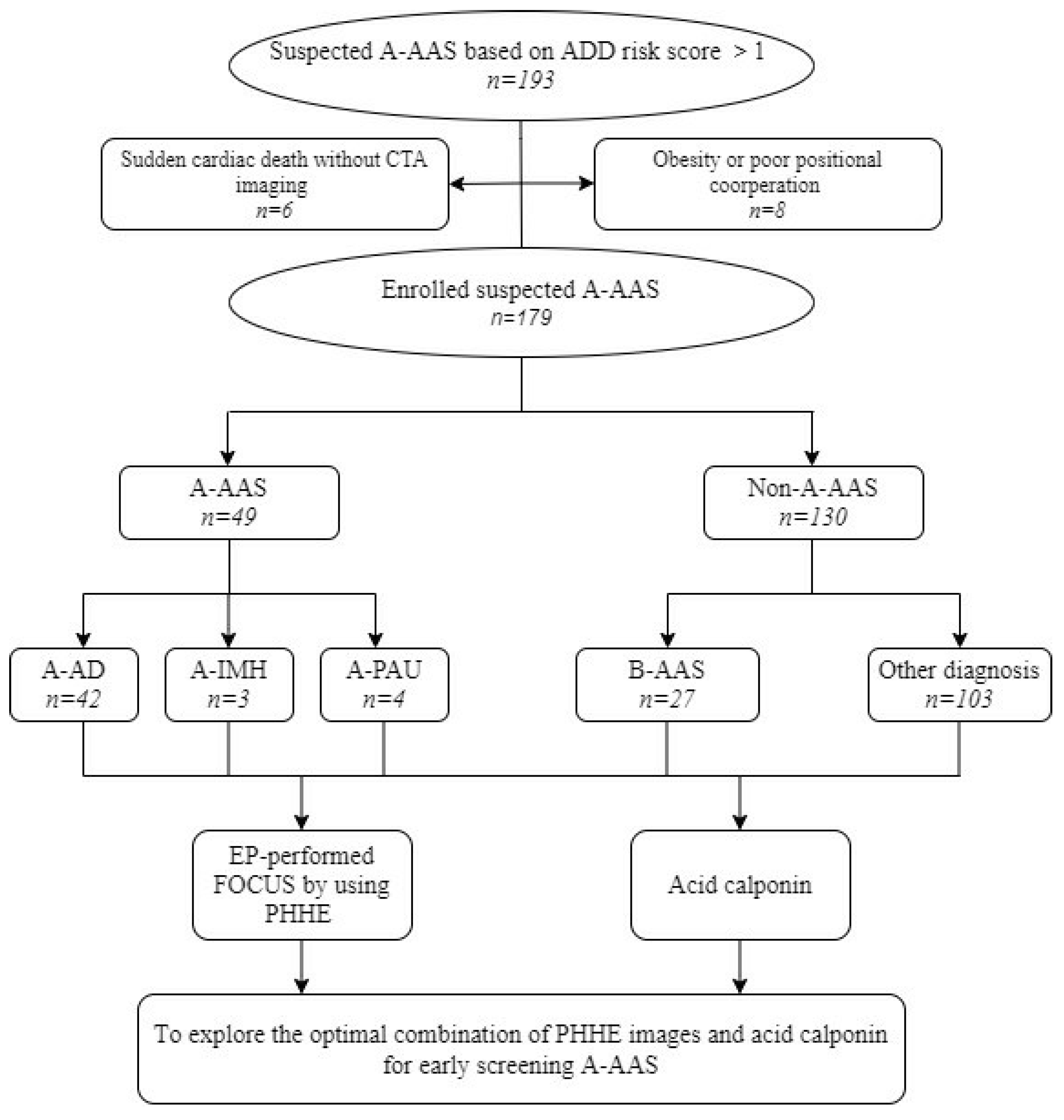
2.1. Study Design
2.2. Study Setting and Enrollment
2.3. ADD Risk Score Definition
2.4. Machine Used
2.5. EP-Performed FOCUS using PHHE
2.6. Acidic Calponin Analysis
2.7. Diagnostic Procedures
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
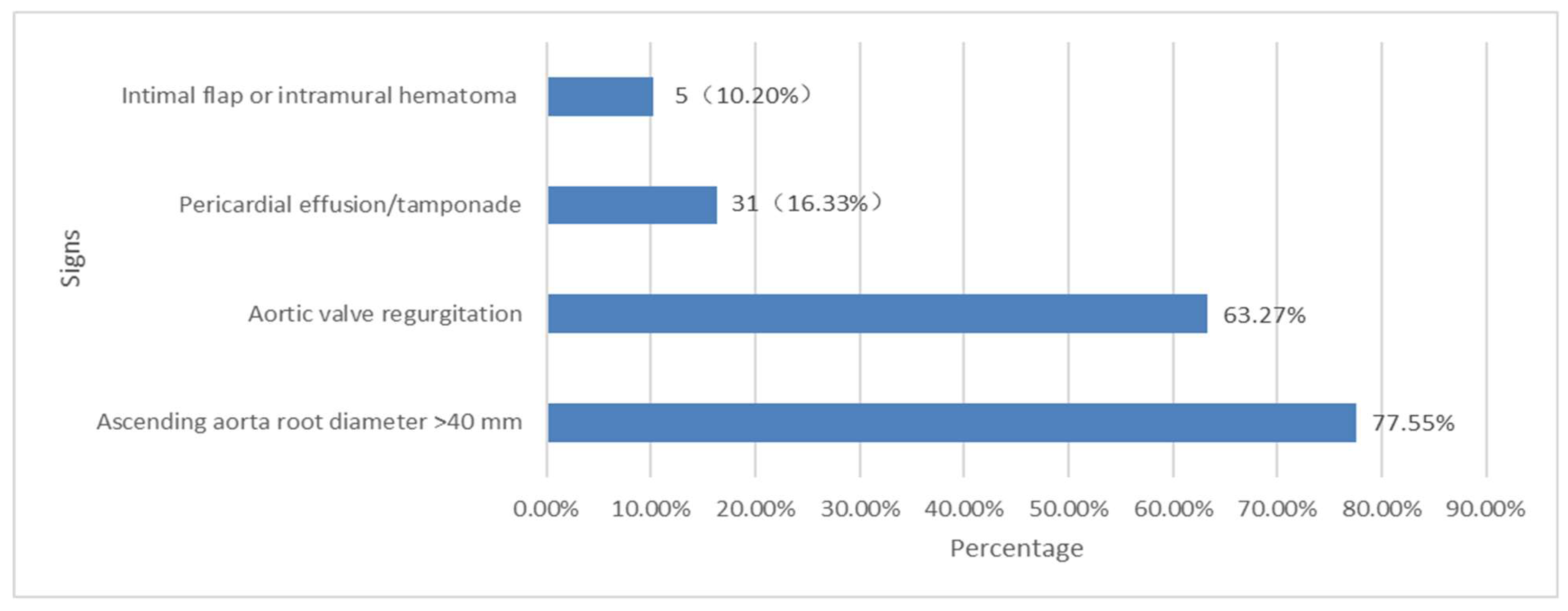
3.2. Direct and Indirect Signs of the PHHE for the Diagnosis of A-AAS
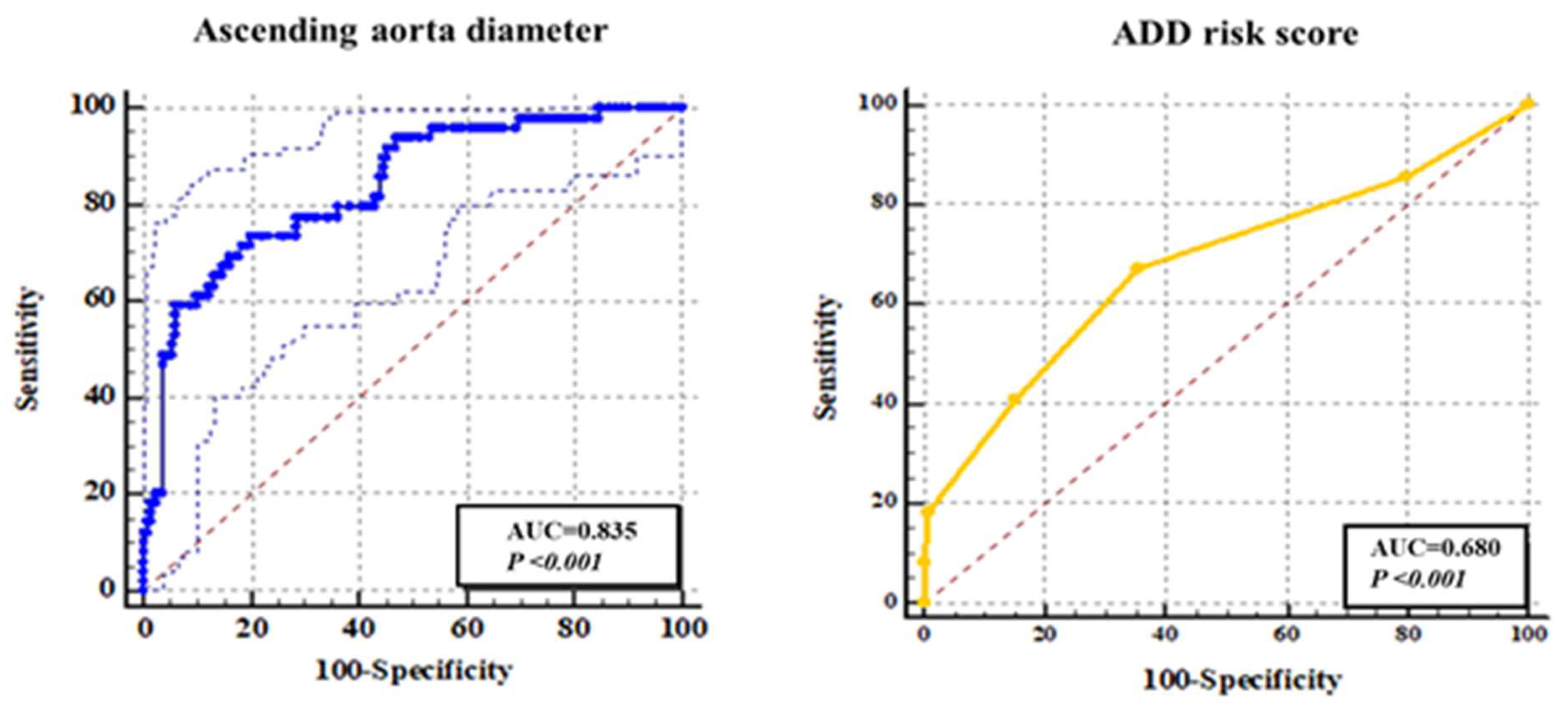
3.3. Independent Diagnostic Performance of Each Sign of PHHE-FOCUS
3.4. The Parallel and Sequence-Combined Diagnostic Value of PHHE-FOCUS Signs for A-AAS
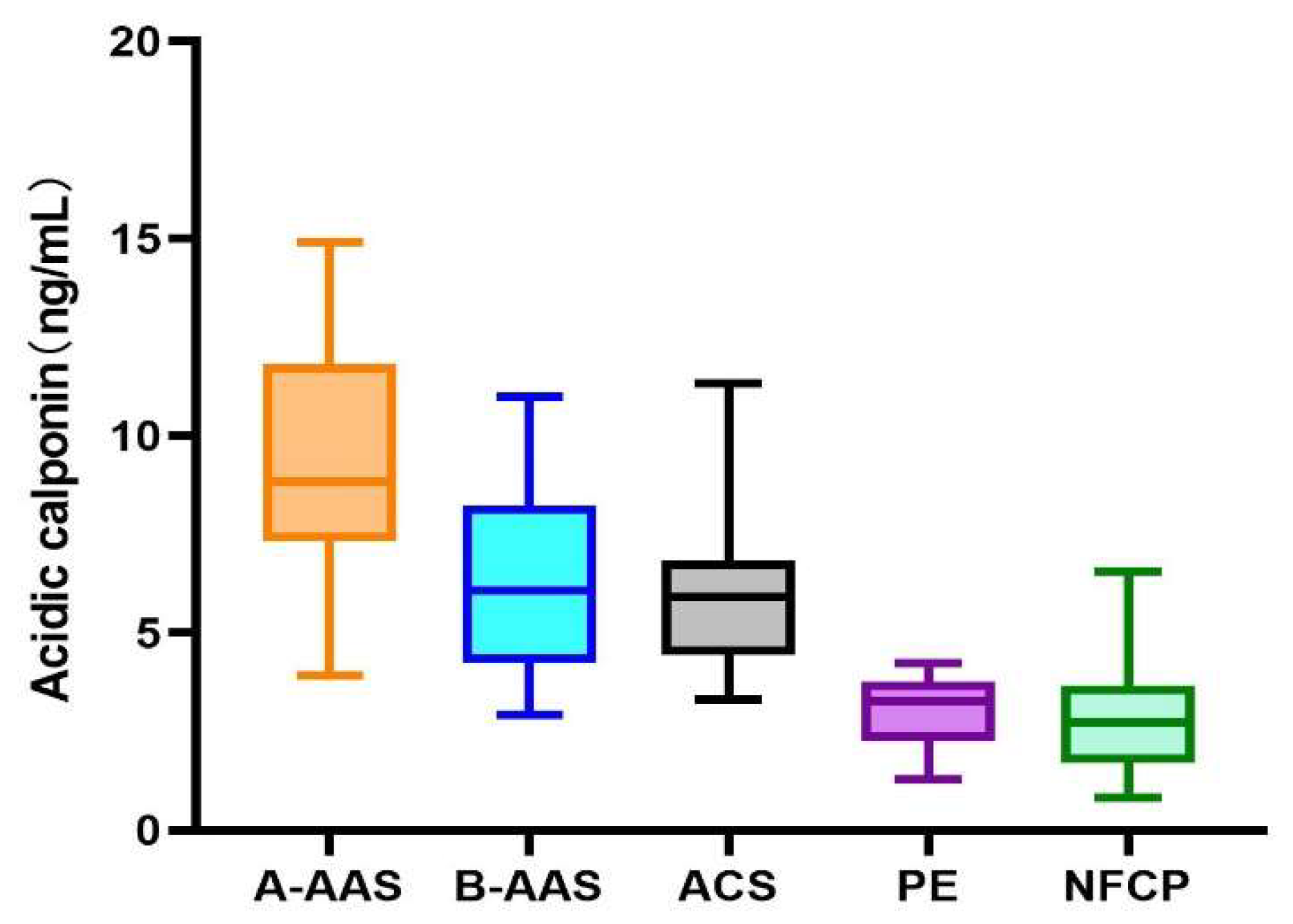
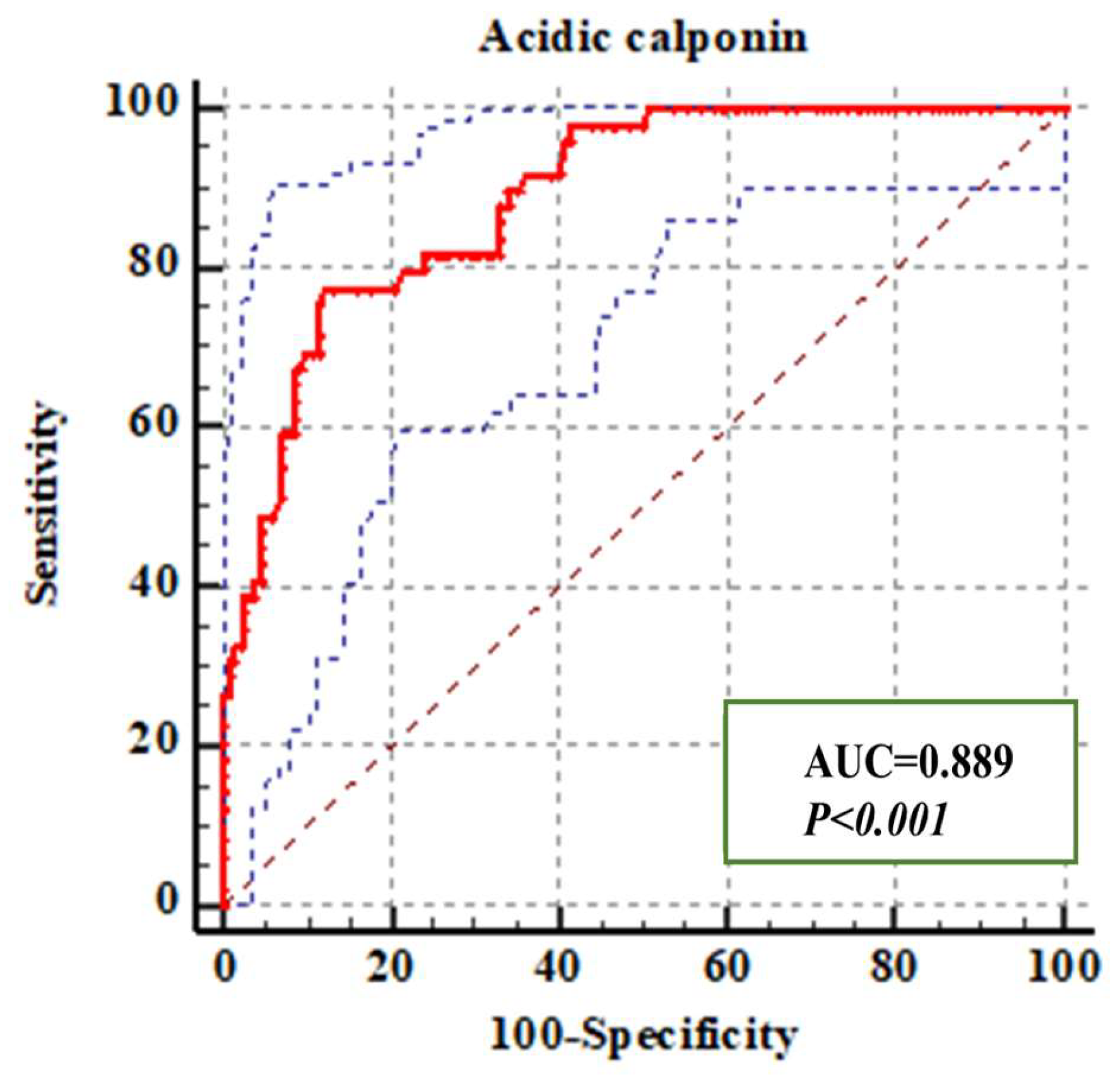
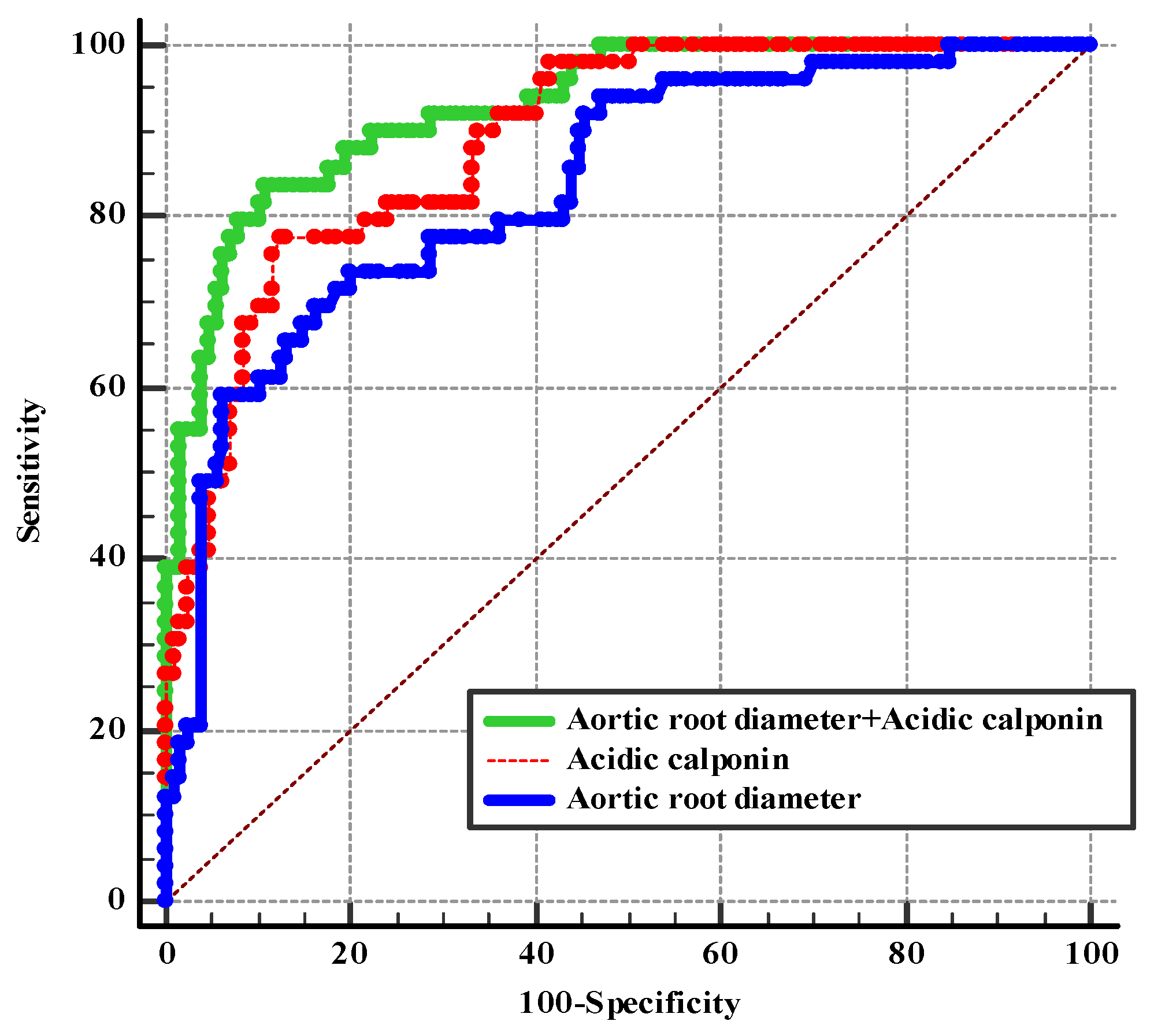
3.5. Diagnostic Efficiency of Acidic Calponin Alone or Combined with an Ascending Aorta Diameter >40 mm
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bossone, E.; LaBounty, T.M.; Eagle, K.A. Acute aortic syndromes: Diagnosis and management, an update. Eur. Heart J. 2018, 39, 739–749. [Google Scholar]
- Pape, L.A.; Awais, M.; Woznicki, E.M.; Suzuki, T.; Trimarchi, S.; Evangelista, A.; Myrmel, T.; Larsen, M.; Harris, K.; Greason, K.; et al. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection. J. Am. Coll. Cardiol. 2015, 66, 350–358. [Google Scholar]
- Chen, A.; Ren, X. Aortic Dissection Manifesting as ST Segment-Elevation Myocardial Infarction. Circulation 2015, 131, 503–504. [Google Scholar] [CrossRef]
- Tsai, T.T.; Nienaber, C.A.; Eagle, K.A. Acute aortic syndromes. Circulation 2005, 112, 3802–3813. [Google Scholar] [CrossRef]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar]
- Cochran, S.T. Anaphylactoid reactions to radiocontrast media. Curr. Allergy Asthma Rep. 2005, 5, 28–31. [Google Scholar] [CrossRef]
- Pourafkari, L.; Tajlil, A.; Ghaffari, S.; Parvizi, R.; Chavoshi, M.; Kolahdouzan, K.; Khaki, N.; Parizad, R.; Hobika, G.G.; Nader, N.D. The frequency of initial misdiagnosis of acute aortic dissection in the emergency department and its impact on outcome. Intern. Emerg. Med. 2016, 12, 1185–1195. [Google Scholar]
- Lovy, A.J.; Bellin, E.; Levsky, J.M.; Esses, D.; Haramati, L.B. Preliminary development of a clinical decision rule for acute aortic syndromes. Am. J. Emerg. Med. 2013, 31, 1546–1550. [Google Scholar]
- Ohle, R.; Anjum, O.; Bleeker, H.; Wells, G.; Perry, J.J. Variation in emergency department use of computed tomography for investigation of acute aortic dissection. Emerg. Radiol. 2018, 25, 293–298. [Google Scholar]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/ SCA/ SCAI/ SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar]
- Nazerian, P.; Giachino, F.; Vanni, S.; Veglio, M.G.; Castelli, M.; Lison, D.; Bitossi, L.; Moiraghi, C.; Grifoni, S.; Morello, F. Diagnostic performance of the aortic dissection detection risk score in patients with suspected acute aortic dissection. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 373–381. [Google Scholar] [CrossRef]
- Lewis, D.; Rang, L.; Kim, D.; Robichaud, L.; Kwan, C.; Pham, C.; Shefrin, A.; Ritcey, B.; Atkinson, P.; Woo, M.; et al. Recommendations for the use of point-of-care ultrasound (POCUS) by emergency physicians in Canada. Can. J. Emerg. Med. 2019, 21, 721–726. [Google Scholar] [CrossRef]
- Chiem, A.T.; Chan, C.H.; Ander, D.S.; Kobylivker, A.N.; Manson, W.C. Comparison of expert and novice sonographers’ performance in focused lung ultrasonography in dyspnea (FLUID) to diagnose patients with acute heart failure syndrome. Acad. Emerg. Med. 2015, 22, 564–573. [Google Scholar]
- Prinz, C.; Voigt, J.U. Diagnostic accuracy of a hand-held ultrasound scanner in routine patients referred for echocardiography. J. Am. Soc. Echocardiogr. 2011, 24, 111–116. [Google Scholar]
- Suzuki, T.; Katoh, H.; Watanabe, M.; Kurabayashi, M.; Hiramori, K.; Hori, S.; Nobuyoshi, M.; Tanaka, H.; Kodama, K.; Sato, H.; et al. Novel biochemical diagnostic method for aortic dissection. Results of a prospective study using an immunoassay of smooth muscle myosin heavy chain. Circulation 1996, 93, 1244–1249. [Google Scholar]
- Suzuki, T.; Katoh, H.; Kurabayashi, M.; Yazaki, Y.; Nagai, R. Biochemical diagnosis of aortic dissection by raised concentrations of creatine kinase BB-isozyme. Lancet 1997, 350, 784–785. [Google Scholar]
- Shinohara, T.; Suzuki, K.; Okada, M.; Shiigai, M.; Shimizu, M.; Maehara, T.; Ohsuzu, F. Soluble elastin fragments in serum are elevated in acute aortic dissection. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1839–1844. [Google Scholar]
- Eggebrecht, H.; Naber, C.K.; Bruch, C.; Kröger, K.; von Birgelen, C.; Schmermund, A.; Wichert, M.; Bartel, T.; Mann, K.; Erbel, R. Value of plasma fibrin D-dimers for detection of acute aortic dissection. J. Am. Coll. Cardiol. 2004, 44, 804–809. [Google Scholar]
- Gorla, R.; Erbel, R.; Kahlert, P.; Tsagakis, K.; Jakob, H.; Mahabadi, A.-A.; Schlosser, T.; Eggebrecht, H.; Bossone, E.; Jánosi, R.A. Accuracy of a diagnostic strategy combining aortic dissection detection risk score and D-dimer levels in patients with suspected acute aortic syndrome. Eur. Heart J. Acute Cardiovasc. Care 2017, 6, 371–378. [Google Scholar] [CrossRef]
- Nazerian, P.; Morello, F.; Vanni, S.; Bono, A.; Castelli, M.; Forno, D.; Gigli, C.; Soardo, F.; Carbone, F.; Lupia, E.; et al. Combined use of aortic dissection detection risk score and D-dimer in the diagnostic workup of suspected acute aortic dissection. Int. J. Cardiol. 2014, 175, 78–82. [Google Scholar] [CrossRef]
- Pare, J.R.; Liu, R.; Moore, C.L.; Sherban, T.; Kelleher, M.S.; Thomas, S.; Taylor, R.A. Emergency physician focused cardiac ultrasound improves diagnosis of ascending aortic dissection. Am. J. Emerg. Med. 2016, 34, 486–492. [Google Scholar]
- Sobczyk, D.; Nycz, K. Feasibility and accuracy of bedside transthoracic echocardiography in diagnosis of acute proximal aortic dissection. Cardiovasc. Ultrasound 2015, 13, 15. [Google Scholar] [CrossRef]
- Suzuki, T.; Distante, A.; Zizza, A.; Trimarchi, S.; Villani, M.; Uriarte, J.A.S.; de Luca Tupputi Schinosa, L.; Renzulli, A.; Sabino, F.; Nowak, R.; et al. Preliminary experience with the smooth muscle troponin-like protein, calponin, as a novel biomarker for diagnosing acute aortic dissection. J. Eur. Heart 2008, 29, 1439–1445. [Google Scholar]
- Ranasinghe, A.M.; Bonser, R.S. Biomarkers in acute aortic dissection and other aortic syndromes. J. Am. Coll. Cardiol. 2010, 56, 1535–1541. [Google Scholar]
- Suzuki, T. Cardiovascular diagnostic biomarkers: The past, present and future. Circ. J. 2009, 73, 806–809. [Google Scholar] [CrossRef]
- Chirillo, F.; Salvador, L.; Bacchion, F.; Grisolia, E.F.; Valfrè, C.; Olivari, Z. Clinical and anatomical characteristics of subtle-discrete dissection of the ascending aorta. Am. J. Cardiol. 2007, 100, 1314–1319. [Google Scholar]
- Evangelista, A.; Avegliano, G.; Aguilar, R.; Cuellar, H.; Igual, A.; González-Alujas, T.; Rodríguez-Palomares, J.; Mahia, P.; García-Dorado, D. Impact of contrast-enhanced echocardiography on the diagnostic algorithm of acute aortic dissection. Eur. Heart J. 2010, 31, 472–479. [Google Scholar]
- Cecconi, M.; Chirillo, F.; Costantini, C.; Iacobone, G.; Lopez, E.; Zanoli, R.; Gili, A.; Moretti, S.; Manfrin, M.; Münch, C.; et al. The role of transthoracic echocardiography in the diagnosis and management of acute type A aortic syndrome. Am. Heart J. 2012, 163, 112–118. [Google Scholar]
- Nazerian, P.; Vanni, S.; Castelli, M.; Morello, F.; Tozzetti, C.; Zagli, G.; Giannazzo, G.; Vergara, R.; Grifoni, S. Diagnostic performance of emergency transthoracic focus cardiac ultrasound in suspected acute type A aortic dissection. Intern. Emerg. Med. 2014, 9, 665–670. [Google Scholar]
- Panoulas, V.; Daigeler, A.; Malaweera, A.; Lota, A.S.; Baskaran, D.; Rahman, S.; Nihoyannopoulos, P. Pocket-size hand-held cardiac ultrasound as an adjunct to clinical examination in the hands of medical students and junior doctors. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Dijos, M.; Pucheux, Y.; Lafitte, M.; Réant, P.; Prevot, A.; Mignot, A.; Barandon, L.; Roques, X.; Roudaut, R.; Pilois, X.; et al. Fast track echo of abdominal aortic aneurysm using a real pocket-ultrasound device at bedside. Echocardiography 2012, 29, 285–290. [Google Scholar] [CrossRef]
- Wen, D.; Zhou, X.L.; Li, J.J.; Hui, R.-T. Biomarkers in aortic dissection. Clin. Chim. Acta 2011, 412, 688–695. [Google Scholar]
- Wang, D.; Wang, Z.-Y.; Wang, J.-F.; Zhang, L.-L.; Zhu, J.-M.; Yuan, Z.-X.; Wang, Y. Values of aortic dissection detection risk score combined with ascending aorta diameter >40 mm for the early identification of type A acute aortic dissection. J. Thorac. Dis. 2018, 10, 1815–1824. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A-AAS (n = 49) | Non-A-AAS (n = 130) | p | |
|---|---|---|---|
| Male, n (%) | 35 (71.4%) | 89 (68.5%) | 0.701 |
| Median age (years) | 55.6 ± 16.7 | 62.7 ± 13.1 | 0.029 |
| High-risk underlying disease or conditions | |||
| Marfan syndrome (other connective tissue disease) | 2 (4.1%) | 0 (0%) | 0.129 |
| Family history of aortic disease | 4 (8.2%) | 10 (7.7%) | 0.917 |
| Known aortic valve disease | 3 (6.1%) | 8 (6.2%) | 0.994 |
| Known thoracic aortic aneurysm | 6 (12.2%) | 5 (3.8%) | 0.082 |
| Recent aortic manipulation | 1 (2.0%) | 0 (0%) | 0.102 |
| High-risk pain features | |||
| Abrupt onset of pain | 42 (85.7%) | 118 (90.8%) | 0.328 |
| Severe pain intensity | 37 (75.5%) | 95 (73.1%) | 0.741 |
| Ripping/tearing pain | 20 (40.8%) | 46 (35.4%) | 0.502 |
| High-risk vitals | |||
| Pulse deficit/systolic bloodpressure differential > 20 mmHg | 18 (36.7%) | 10 (7.7%) | 0.011 |
| Focal neurological deficit (accompanied by pain) | 8 (16.3%) | 5 (3.8%) | 0.04 |
| Murmur of aortic insufficiency (new onset) | 8 (16.3%) | 16 (12.3%) | 0.482 |
| Hypotension or shock state | 9 (18.4%) | 10 (7.7%) | 0.039 |
| ADD markers | 3.2 ± 1.5 | 2.4 ± 1.6 | 0.001 |
| Sens, % | Spec, % | PPV, % | NPV, % | AC, % | |
|---|---|---|---|---|---|
| Direct sonographic signs | 10.2 (5/49) | 97.7 (127/130) | 62.5 (5/8) | 74.3 (127/171) | 73.7 (132/179) |
| Ascending aortic dilatation | 77.6 (38/49) | 68.5 (89/130) | 48.1 (38/79) | 89 (89/100) | 70.9 (127/179) |
| Pericardial effusion/tamponade | 16.3 (8/49) | 90.8 (118/130) | 40 (8/20) | 74. (118/159) | 70.4 (126/179) |
| Aortic valve insufficiency | 63.3 (31/49) | 67.7 (88/130) | 42.5 (31/73) | 83 (88/106) | 66.5 (119/179) |
| Sens, % | Spec, % | PPV, % | NPV, % | AC, % | |
|---|---|---|---|---|---|
| Formula 1 a | 79.6 (39/49) | 67.7 (88/130) | 48.1 (39/81) | 89.8 (88/98) | 70.9 (127/179) |
| Formula 2 b | 81.6 (40/49) | 63.1 (82/130) | 45.5 (40/88) | 90.1 (82/91) | 68.2 (122/179) |
| Formula 3 c | 85.7(42/49) | 61.5 (80/130) | 45.6 (42/92) | 92 (80/87) | 68.2 (122/179) |
| Sens, % | Spec, % | PPV, % | NPV, % | AC, % | |
|---|---|---|---|---|---|
| Formula 1 d | 4.1 (2/49) | 99.2 (129/130) | 66.7 (2/3) | 73.3 (129/176) | 73.2 (131/179) |
| Formula 2 e | 4.1 (2/49) | 100 (130/130) | 100 (2/2) | 73.4 (130/177) | 73.7 (132/179) |
| Formula 3 f | 4.1 (2/49) | 100 (130/130) | 100 (2/2) | 73.4 (130/177) | 73.7 (132/179) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lian, R.; Zhang, T.; Liu, J.; Zhang, G.; Hu, T.; Li, G.; Zhang, S.; Zhang, G. Routine Use of a Pocket-Sized Handheld Echoscopic Device Plus a Biomarker by Emergency Medicine Residents with an Early Screening Algorithm for Suspected Type A Acute Aortic Syndrome. J. Clin. Med. 2023, 12, 1346. https://doi.org/10.3390/jcm12041346
Lian R, Zhang T, Liu J, Zhang G, Hu T, Li G, Zhang S, Zhang G. Routine Use of a Pocket-Sized Handheld Echoscopic Device Plus a Biomarker by Emergency Medicine Residents with an Early Screening Algorithm for Suspected Type A Acute Aortic Syndrome. Journal of Clinical Medicine. 2023; 12(4):1346. https://doi.org/10.3390/jcm12041346
Chicago/Turabian StyleLian, Rui, Tongzhe Zhang, Juanjuan Liu, Guochao Zhang, Tianpeng Hu, Guonan Li, Suqiao Zhang, and Guoqiang Zhang. 2023. "Routine Use of a Pocket-Sized Handheld Echoscopic Device Plus a Biomarker by Emergency Medicine Residents with an Early Screening Algorithm for Suspected Type A Acute Aortic Syndrome" Journal of Clinical Medicine 12, no. 4: 1346. https://doi.org/10.3390/jcm12041346