

Construction and Validation of a Nomogram Clinical Prediction Model for Predicting Osteoporosis in an Asymptomatic Elderly Population in Beijing

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Information on Clinical Factors
2.3. DXA Examination and Diagnostic Criteria for Osteoporosis
2.4. Construction and Validation of the Nomogram Prediction Model
2.5. Statistical Analysis
3. Results
3.1. Participant and Clinical Characteristics
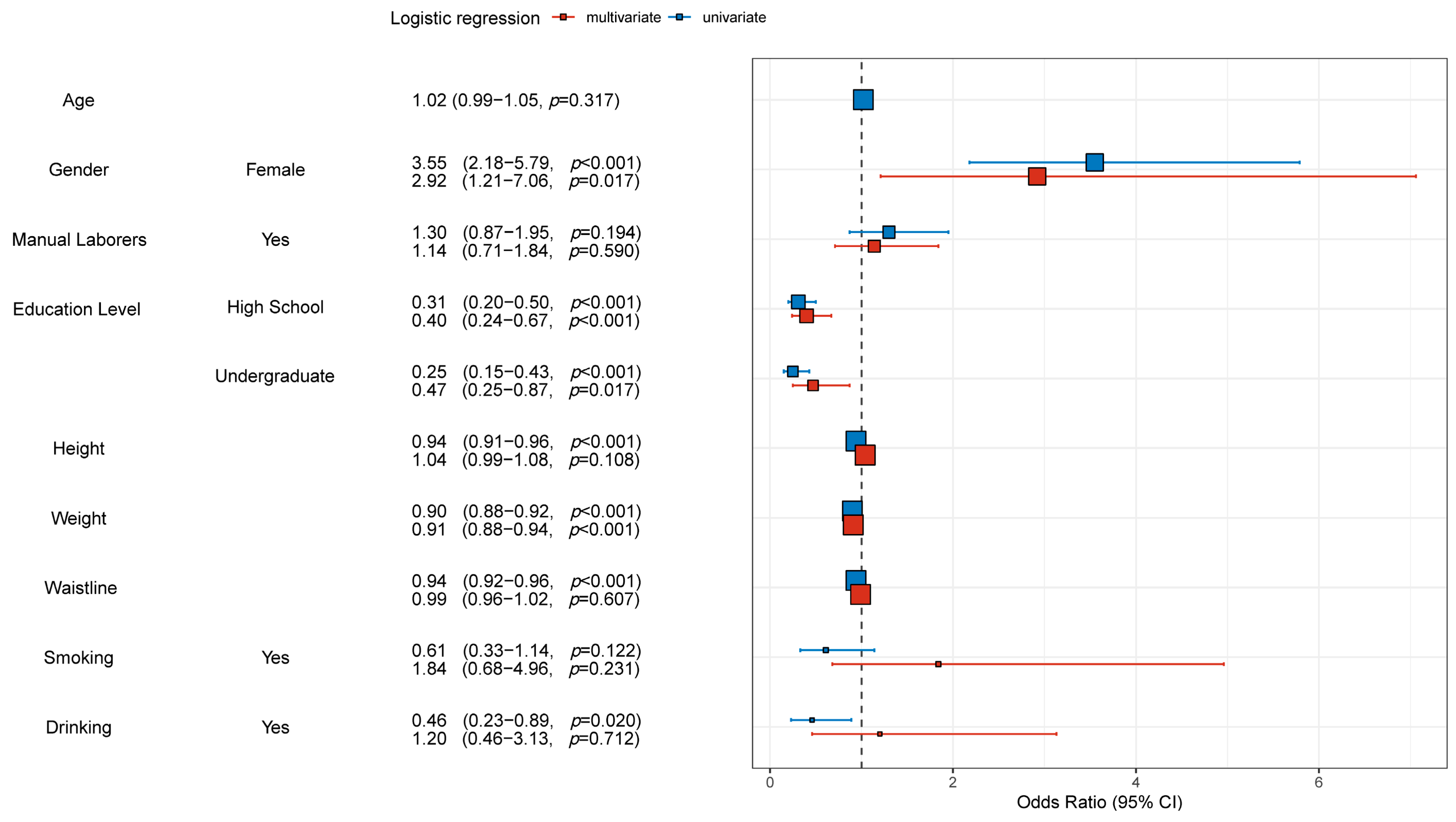
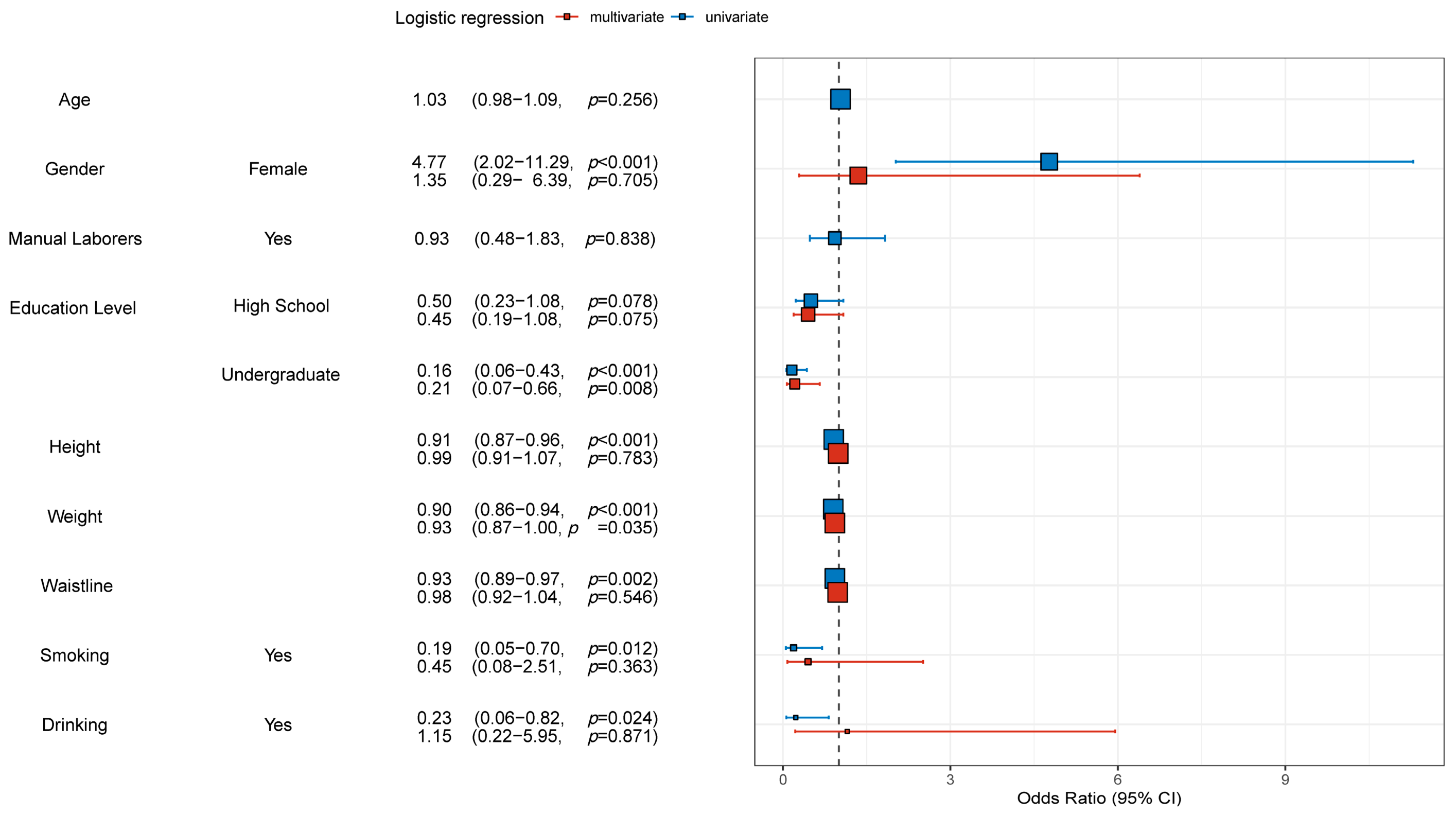
3.2. Univariate and Multivariate Logistic Regression Analyeis of Osteoporosis
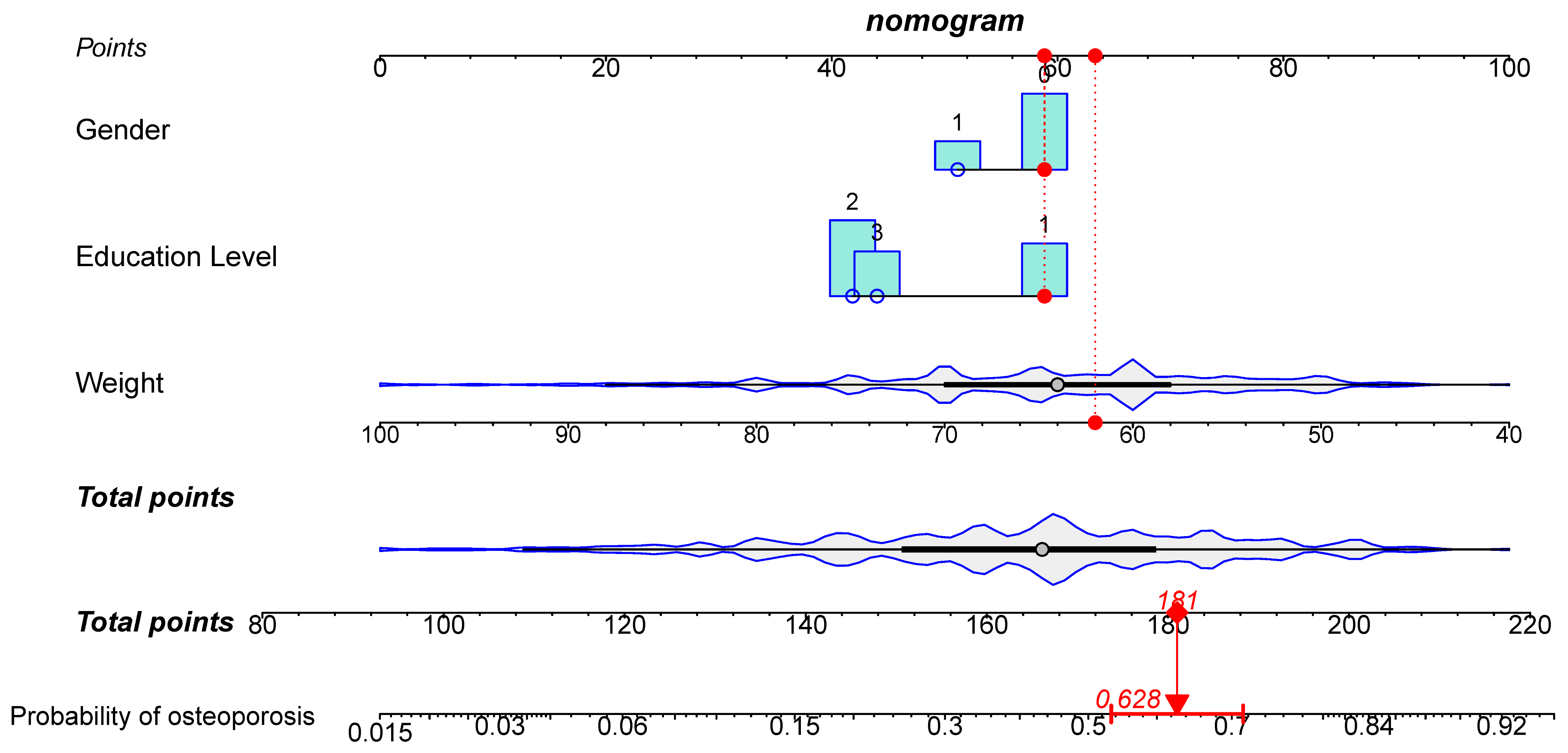
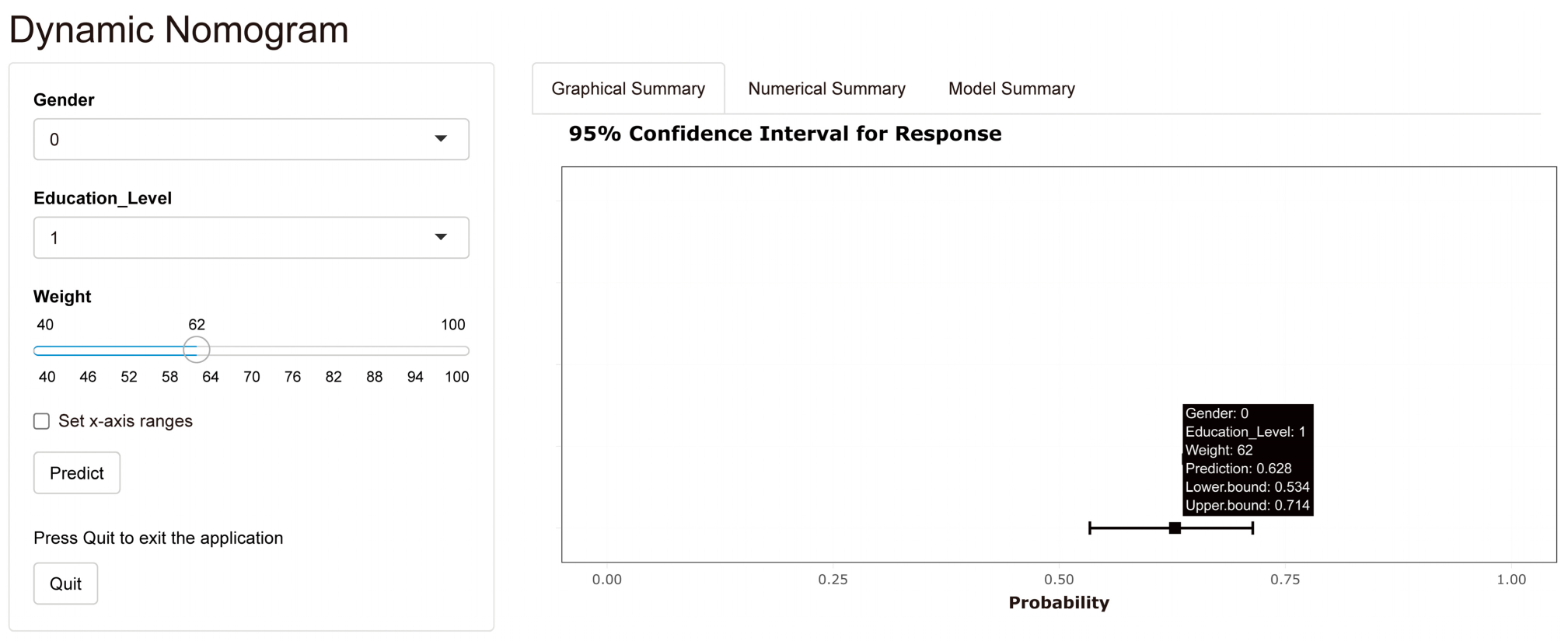
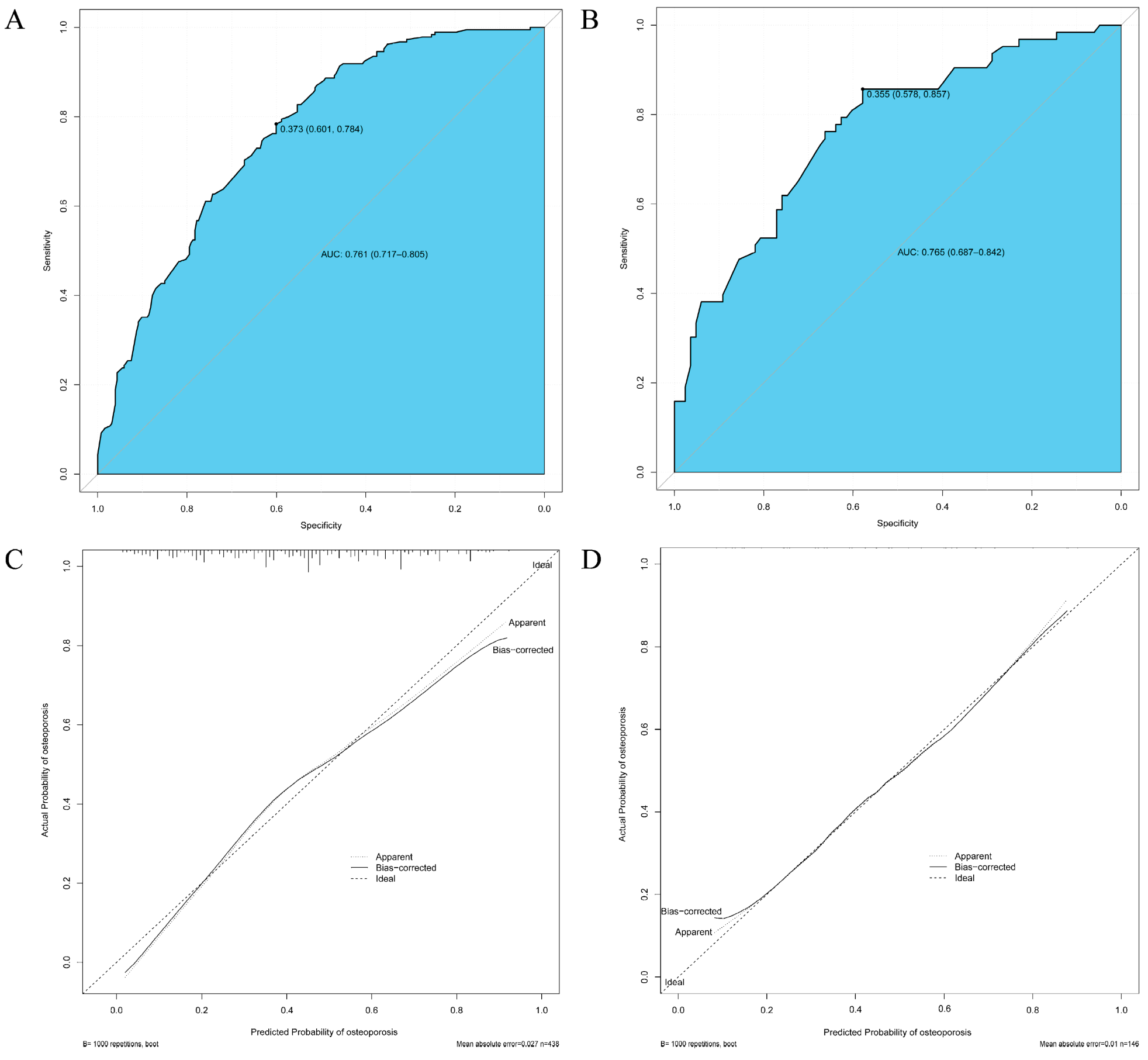
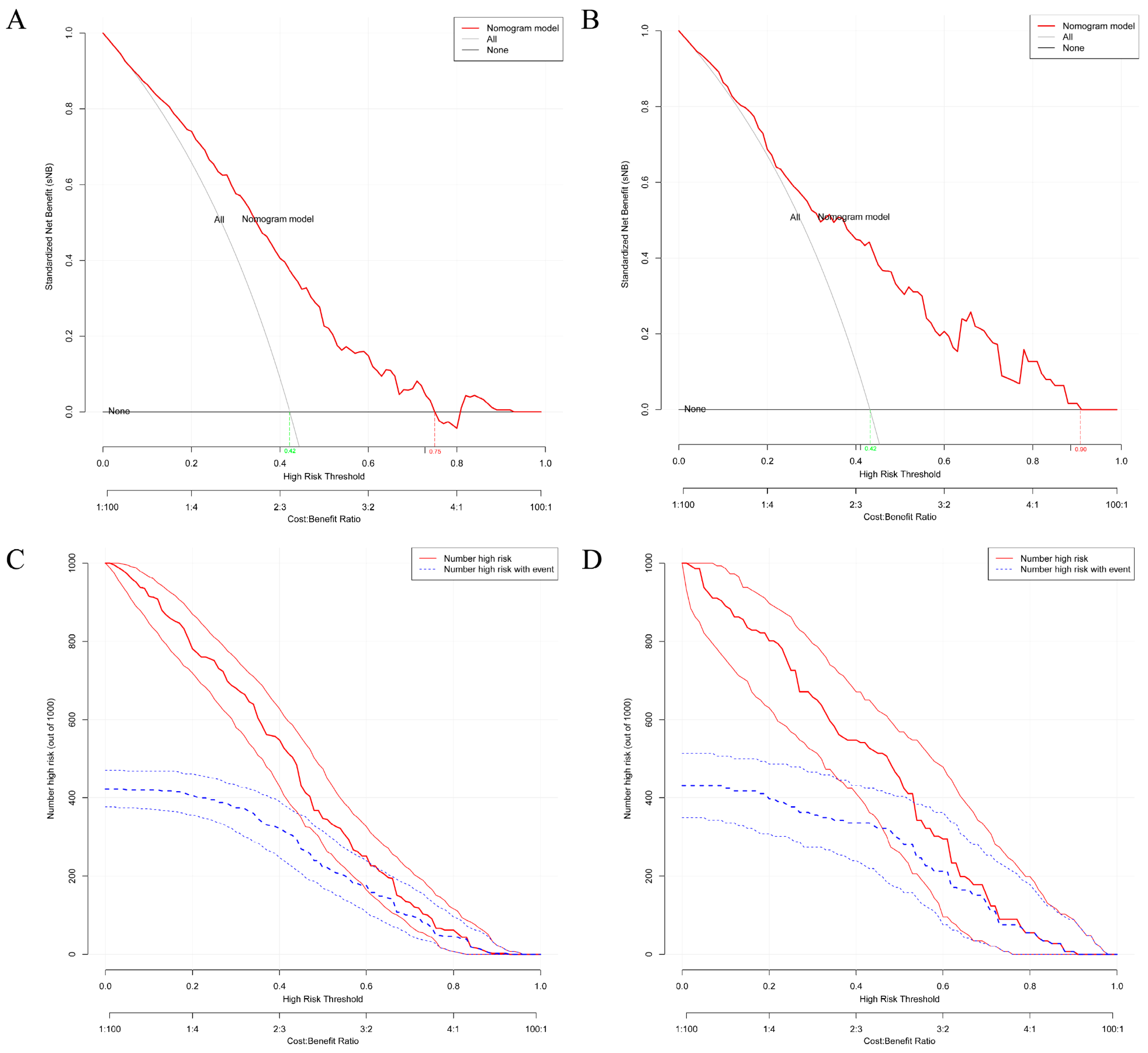
3.3. Construction and Validation of the Nomogram Clinical Prediction Model for Osteoporosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Sfeir, J.G.; Drake, M.T.; Khosla, S.; Farr, J.N. Skeletal Aging. Mayo. Clin. Proc. 2022, 97, 1194–1208. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yu, W.; Yin, X.; Cui, L.; Tang, S.; Jiang, N.; Cui, L.; Zhao, N.; Lin, Q.; Chen, L.; et al. Prevalence of Osteoporosis and Fracture in China: The China Osteoporosis Prevalence Study. JAMA Netw. Open 2021, 4, e2121106. [Google Scholar] [CrossRef] [PubMed]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Eastell, R.; O’Neill, T.W.; Hofbauer, L.C.; Langdahl, B.; Reid, I.R.; Gold, D.T.; Cummings, S.R. Postmenopausal osteoporosis. Nat. Rev. Dis. Prim. 2016, 2, 16070. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Crandall, C.J. Osteoporosis. Ann. Intern. Med. 2017, 167, ITC17–ITC32. [Google Scholar] [CrossRef]
- Schraders, K.; Zatta, G.; Kruger, M.; Coad, J.; Weber, J.; Brough, L.; Thomson, J. Quantitative Ultrasound and Dual X-Ray Absorptiometry as Indicators of Bone Mineral Density in Young Women and Nutritional Factors Affecting It. Nutrients 2019, 11, 2336. [Google Scholar] [CrossRef]
- Haseltine, K.N.; Chukir, T.; Smith, P.J.; Jacob, J.T.; Bilezikian, J.P.; Farooki, A. Bone Mineral Density: Clinical Relevance and Quantitative Assessment. J. Nucl. Med. 2021, 62, 446–454. [Google Scholar] [CrossRef]
- Oei, L.; Koromani, F.; Rivadeneira, F.; Zillikens, M.C.; Oei, E.H. Quantitative imaging methods in osteoporosis. Quant. Imaging Med. Surg. 2016, 6, 680–698. [Google Scholar] [CrossRef]
- Roux, C.; Briot, K. Current role for bone absorptiometry. Jt. Bone Spine 2017, 84, 35–37. [Google Scholar] [CrossRef]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Oden, A.; Melton, L.J., 3rd; Khaltaev, N. A reference standard for the description of osteoporosis. Bone 2008, 42, 467–475. [Google Scholar] [CrossRef]
- World Health Organization. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech. Rep. Ser. 1994, 843, 1–129. [Google Scholar]
- Krishnamoorthy, P.; Freeman, C.; Bernstein, M.L.; Lawrence, S.; Rodd, C. Osteopenia in Children Who Have Undergone Posterior Fossa or Craniospinal Irradiation for Brain Tumors. Arch. Pediatr. Adolesc. Med. 2004, 158, 491–496. [Google Scholar] [CrossRef]
- Marcovici, P.A.; Berdon, W.E.; Liebling, M.S. Osteochondromas and growth retardation secondary to externally or internally administered radiation in childhood. Pediatr. Radiol. 2007, 37, 301–304. [Google Scholar] [CrossRef]
- Xian, W.; Xu, X.; Li, J.; Sun, J.; Fu, H.; Wu, S.; Liu, H. Health care inequality under different medical insurance schemes in a socioeconomically underdeveloped region of China: A propensity score matching analysis. BMC Public Health 2019, 19, 1373. [Google Scholar] [CrossRef]
- Eloranta, S.; Boman, M. Predictive models for clinical decision making: Deep dives in practical machine learning. J. Intern. Med. 2022, 292, 278–295. [Google Scholar] [CrossRef]
- Faggion, C.M., Jr.; Chambrone, L.; Tu, Y.-K. Quality of logistic regression reporting in studies of tooth survival after periodontal treatment. J. Clin. Periodontol. 2014, 41, 1184–1192. [Google Scholar] [CrossRef]
- Scosyrev, E.; Glimm, E. Power analysis for multivariable Cox regression models. Stat. Med. 2019, 38, 88–99. [Google Scholar] [CrossRef]
- Jehi, L.; Yardi, R.; Chagin, K.; Tassi, L.; Russo, G.L.; Worrell, G.; Hu, W.; Cendes, F.; Morita, M.; Bartolomei, F.; et al. Development and validation of nomograms to provide individualised predictions of seizure outcomes after epilepsy surgery: A retrospective analysis. Lancet Neurol. 2015, 14, 283–290. [Google Scholar] [CrossRef]
- Wang, W.; Liu, W. PCLasso: A protein complex-based, group lasso-Cox model for accurate prognosis and risk protein complex discovery. Brief. Bioinform. 2021, 22, bbab212. [Google Scholar] [CrossRef]
- Tang, C.X.; Guo, B.J.; Schoepf, J.U.; Bayer, R.R., 2nd; Liu, C.Y.; Qiao, H.Y.; Zhou, F.; Lu, G.M.; Zhou, C.S.; Zhang, L.J. Feasibility and prognostic role of machine learning-based FFR(CT) in patients with stent implantation. Eur. Radiol. 2021, 31, 6592–6604. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, A.; Shiradkar, R.; Fu, P.; Mahran, A.; Rastinehad, A.R.; Tewari, A.; Tirumani, S.H.; Purysko, A.; Ponsky, L.; Madabhushi, A. An integrated nomogram combining deep learning, Prostate Imaging–Reporting and Data System (PI-RADS) scoring, and clinical variables for identification of clinically significant prostate cancer on biparametric MRI: A retrospective multicentre study. Lancet Digit. Health 2021, 3, e445–e454. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Miceli, R.; Rimassa, L.; Lonardi, S.; Aprile, G.; Mennitto, A.; Marmorino, F.; Bozzarelli, S.; Antonuzzo, L.; Tamburini, E.; et al. Estimating 12-week death probability in patients with refractory metastatic colorectal cancer: The Colon Life nomogram. Ann. Oncol. 2016, 28, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Tang, L.; Li, Z.Y.; Fang, M.J.; Gao, J.B.; Shan, X.H.; Ying, X.J.; Sun, Y.S.; Fu, J.; Wang, X.X.; et al. Development and validation of an individualized nomogram to identify occult peritoneal metastasis in patients with advanced gastric cancer. Ann. Oncol. 2019, 30, 431–438. [Google Scholar] [CrossRef]
- Pluskiewicz, W.; Adamczyk, P.; Franek, E.; Leszczynski, P.; Sewerynek, E.; Wichrowska, H.; Napiorkowska, L.; Kostyk, T.; Stuss, M.; Stepien-Klos, W.; et al. Ten-year probability of osteoporotic fracture in 2012 Polish women assessed by FRAX and nomogram by Nguyen et al.—Conformity between methods and their clinical utility. Bone 2010, 46, 1661–1667. [Google Scholar] [CrossRef]
- Dong, Y.-M.; Sun, J.; Li, Y.-X.; Chen, Q.; Liu, Q.-Q.; Sun, Z.; Pang, R.; Chen, F.; Xu, B.-Y.; Manyande, A.; et al. Development and Validation of a Nomogram for Assessing Survival in Patients With COVID-19 Pneumonia. Clin. Infect. Dis. 2021, 72, 652–660. [Google Scholar] [CrossRef]
- Liu, L.; Xie, J.; Wu, W.; Chen, H.; Li, S.; He, H.; Yu, Y.; Hu, M.; Li, J.; Zheng, R.; et al. A simple nomogram for predicting failure of non-invasive respiratory strategies in adults with COVID-19: A retrospective multicentre study. Lancet Digit. Health 2021, 3, e166–e174. [Google Scholar] [CrossRef]
- Long, S.-Y.; Sun, J.-Y.; Wang, L.; Long, H.; Jiang, H.-Q.; Shi, Y.; Zhang, W.-Y.; Xiong, J.-S.; Sun, P.-W.; Chen, Y.-Q.; et al. Predictive nomogram for leprosy using genetic and epidemiological risk factors in Southwestern China: Case–control and prospective analyses. EBioMedicine 2021, 68, 103408. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How To Build and Interpret a Nomogram for Cancer Prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Chen, F.-P.; Huang, T.-S.; Fu, T.-S.; Sun, C.-C.; Chao, A.-S.; Tsai, T.-L. Secular trends in incidence of osteoporosis in Taiwan: A nationwide population-based study. Biomed. J. 2018, 41, 314–320. [Google Scholar] [CrossRef]
- Tuzun, S.; Eskiyurt, N.; Akarirmak, U.; Saridogan, M.; Senocak, M.; Johansson, H.; Kanis, J.A.; Turkish Osteoporosis, S. Incidence of hip fracture and prevalence of osteoporosis in Turkey: The FRACTURK study. Osteoporos. Int. 2011, 23, 949–955. [Google Scholar] [CrossRef]
- Pouresmaeili, F.; Dehghan, B.K.; Kamarehei, M.; Meng, G.Y. A comprehensive overview on osteoporosis and its risk factors. Ther. Clin. Risk Manag. 2018, 14, 2029–2049. [Google Scholar] [CrossRef]
- Wong, C.P.; Lok, M.K.; Wun, Y.T.; Pang, S.M. Chinese men’s knowledge and risk factors of osteoporosis: Compared with women’s. Am. J. Mens. Health 2014, 8, 159–166. [Google Scholar] [CrossRef]
- DongMei, N.; Japanese Population-based Osteoporosis (JPOS) Study Group; Iki, M.; Tamaki, J.; Sato, Y.; Kagamimori, S.; Kagawa, Y.; Yoneshima, H. Association between weight changes and changes in hip geometric indices in the Japanese female population during 10-year follow-up: Japanese Population-based Osteoporosis (JPOS) Cohort Study. Osteoporos. Int. 2012, 23, 1581–1591. [Google Scholar] [CrossRef]
- Bui, M.H.; Dao, P.T.; Khuong, Q.L.; Le, P.-A.; Nguyen, T.-T.T.; Du Hoang, G.; Le, T.H.; Pham, H.T.; Hoang, H.-X.T.; Le, Q.C.; et al. Evaluation of community-based screening tools for the early screening of osteoporosis in postmenopausal Vietnamese women. PLoS ONE 2022, 17, e0266452. [Google Scholar] [CrossRef]
- Liu, M.-Y.; Li, C.-L.; Pei, Y.; Xiao, Y.-J.; Zhang, Y.; Cheng, X.-L. Diagnostic values of self-assessment tool for Asians for osteoporosis in aged men. Zhonghua Yi Xue Za Zhi 2011, 91, 2112–2115. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Group | Validation Group | |||||||
|---|---|---|---|---|---|---|---|---|
| [All] | No Osteoporosis | Osteoporosis | p Value | [All] | No Osteoporosis | Osteoporosis | p Value | |
| n = 438 | n = 253 | n = 185 | n = 146 | n = 83 | n = 63 | |||
| Age (years): | 67.2 ± 6.48 | 66.9 ± 6.66 | 67.5 ± 6.23 | 0.312 | 66.1 ± 6.31 | 65.6 ± 6.94 | 66.8 ± 5.37 | 0.240 |
| Gender: | <0.001 | <0.001 | ||||||
| Female | 319 (72.8%) | 160 (63.2%) | 159 (85.9%) | 104 (71.2%) | 49 (59.0%) | 55 (87.3%) | ||
| Male | 119 (27.2%) | 93 (36.8%) | 26 (14.1%) | 42 (28.8%) | 34 (41.0%) | 8 (12.7%) | ||
| Manual Laborers: | 0.231 | 0.974 | ||||||
| No | 292 (66.7%) | 175 (69.2%) | 117 (63.2%) | 89 (61.0%) | 50 (60.2%) | 39 (61.9%) | ||
| Yes | 146 (33.3%) | 78 (30.8%) | 68 (36.8%) | 57 (39.0%) | 33 (39.8%) | 24 (38.1%) | ||
| Education Level: | <0.001 | 0.001 | ||||||
| Junior high school | 133 (30.4%) | 49 (19.4%) | 84 (45.4%) | 46 (31.5%) | 18 (21.7%) | 28 (44.4%) | ||
| High school | 192 (43.8%) | 125 (49.4%) | 67 (36.2%) | 64 (43.8%) | 36 (43.4%) | 28 (44.4%) | ||
| Undergraduate | 113 (25.8%) | 79 (31.2%) | 34 (18.4%) | 36 (24.7%) | 29 (34.9%) | 7 (11.1%) | ||
| Height (cm) | 160 [156;167] | 162 [158;169] | 160 [155;164] | <0.001 | 161 [157;168] | 163 [160; 171] | 158 [156; 162] | <0.001 |
| Weight (kg) | 64.0 [58.0; 70.0] | 67.0 [60.0; 75.0] | 60.0 [55.0;65.0] | <0.001 | 65.0 [59.0;70.0] | 67.0 [61.0; 74.5] | 60.0 [54.0; 65.0] | <0.001 |
| Waistline (cm) | 84.0 [79.0; 90.0] | 86.0 [80.0; 92.0] | 80.0 [76.0;86.0] | <0.001 | 84.0 [79.0; 90.0] | 85.0 [80.0; 90.0] | 80.0 [76.0;86.5] | 0.001 |
| Smoking: | 0.160 | 0.013 | ||||||
| No | 388 (88.6%) | 219 (86.6%) | 169 (91.4%) | 126 (86.3%) | 66 (79.5%) | 60 (95.2%) | ||
| Yes | 50 (11.4%) | 34 (13.4%) | 16 (8.65%) | 20 (13.7%) | 17 (20.5%) | 3 (4.76%) | ||
| Drinking: | 0.027 | 0.030 | ||||||
| No | 389 (88.8%) | 217 (85.8%) | 172 (93.0%) | 128 (87.7%) | 68 (81.9%) | 60 (95.2%) | ||
| Yes | 49 (11.2%) | 36 (14.2%) | 13 (7.03%) | 18 (12.3%) | 15 (18.1%) | 3 (4.76%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Kong, C.; Pan, F.; Lu, S. Construction and Validation of a Nomogram Clinical Prediction Model for Predicting Osteoporosis in an Asymptomatic Elderly Population in Beijing. J. Clin. Med. 2023, 12, 1292. https://doi.org/10.3390/jcm12041292
Wang J, Kong C, Pan F, Lu S. Construction and Validation of a Nomogram Clinical Prediction Model for Predicting Osteoporosis in an Asymptomatic Elderly Population in Beijing. Journal of Clinical Medicine. 2023; 12(4):1292. https://doi.org/10.3390/jcm12041292
Chicago/Turabian StyleWang, Jialin, Chao Kong, Fumin Pan, and Shibao Lu. 2023. "Construction and Validation of a Nomogram Clinical Prediction Model for Predicting Osteoporosis in an Asymptomatic Elderly Population in Beijing" Journal of Clinical Medicine 12, no. 4: 1292. https://doi.org/10.3390/jcm12041292