
Plasma Troponins Identify Patients with Very Low-Risk Acute Pulmonary Embolism
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
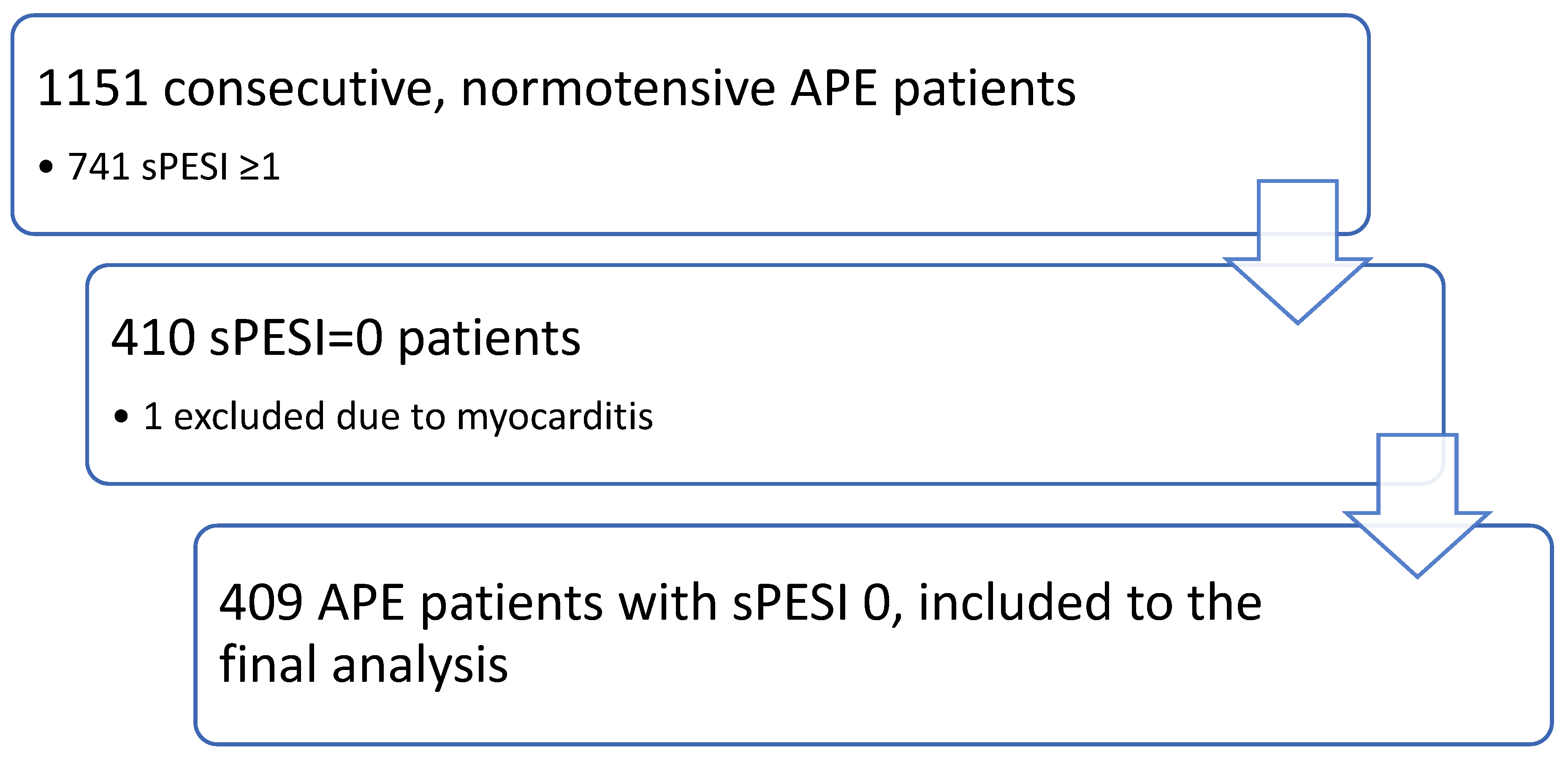
2.1. Study Population
2.2. Echocardiography
2.3. Biochemical Analysis
2.4. The Clinical Endpoint (CE) of the Study
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstantinides, S.V.; Meyer, G. The 2019 ESC Guidelines on the Diagnosis and Management of Acute Pulmonary Embolism. Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Miró, Ò.; Jiménez, S.; Mebazaa, A.; Freund, Y.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; García-Lamberechts, E.J.; Alquézar-Arbé, A.; Jacob, J.; et al. Pulmonary embolism in patients with COVID-19: Incidence, risk factors, clinical characteristics, and outcome. Eur. Heart J. 2021, 42, 3127–3142. [Google Scholar] [CrossRef]
- Porfidia, A.; Valeriani, E.; Pola, R.; Porreca, E.; Rutjes, A.W.S.; Di Nisio, M. Venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis. Thromb. Res. 2020, 196, 67–74. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G. Predictors of mortality from pulmonary embolism and their influence on clinical management. Thromb. Haemost. 2008, 100, 747–751. [Google Scholar]
- Marti, C.; John, G.; Konstantinides, S.; Combescure, C.; Sanchez, O.; Lankeit, M.; Meyer, G.; Perrier, A. Systemic thrombolytic therapy for acute pulmonary embolism: A systematic review and meta-analysis. Eur. Heart J. 2015, 36, 605–614. [Google Scholar] [CrossRef]
- Barco, S.; Schmidtmann, I.; Ageno, W.; Bauersachs, R.M.; Becattini, C.; Bernardi, E.; Beyer-Westendorf, J.; Bonacchini, L.; Brachmann, J.; Christ, M.; et al. Early discharge and home treatment of patients with low-risk pulmonary embolism with the oral factor Xa inhibitor rivaroxaban: An international multicentre single-arm clinical trial. Eur. Heart J. 2020, 41, 509–518. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G.; Lankeit, M.; Masotti, L.; Pruszczyk, P.; Casazza, F.; Vanni, S.; Nitti, C.; Kamphuisen, P.; Vedovati, M.C.; et al. Acute pulmonary embolism: Mortality prediction by the 2014 European Society of Cardiology risk stratification model. Eur. Respir. J. 2016, 48, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Barco, S.; Woersching, A.L.; Spyropoulos, A.C.; Piovella, F.; Mahan, C.E. European Union-28: An annualized cost-of-illness model for venous thromboembolism. Thromb. Haemost. 2016, 115, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Bledsoe, J.R.; Woller, S.C.; Stevens, S.M.; Aston, V.; Patten, R.; Allen, T.; Horne, B.D.; Dong, L.; Lloyd, J.; Snow, G.; et al. Management of Low-Risk Pulmonary Embolism Patients without Hospitalization: The Low-Risk Pulmonary Embolism Prospective Management Study. Chest 2018, 154, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; de Wit, K. Pulmonary Embolism. N. Engl. J. Med. 2022, 387, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Paczyńska, M.; Kurnicka, K.; Lichodziejewska, B.; Goliszek, S.; Dzikowska-Diduch, O.; Sobieraj, P.; Burzyński, Ł.; Kostrubiec, M.; Pruszczyk, P.; Ciurzyński, M. Acute pulmonary embolism treatment with rivaroxaban results in a shorter duration of hospitalisation compared to standard therapy: An academic centre experience. Kardiol. Pol. 2016, 74, 650–656. [Google Scholar] [CrossRef]
- Barco, S.; Mahmoudpour, S.H.; Planquette, B.; Sanchez, O.; Konstantinides, S.V.; Meyer, G. Prognostic value of right ventricular dysfunction or elevated cardiac biomarkers in patients with low-risk pulmonary embolism: A systematic review and meta-analysis. Eur. Heart J. 2019, 40, 902–910. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270, Erratum in Eur. Heart J. Cardiovasc. Imaging 2016, 17, 412; Erratum in Eur. Heart J. Cardiovasc. Imaging 2016, 17, 969. [Google Scholar] [CrossRef]
- Kurnicka, K.; Lichodziejewska, B.; Goliszek, S.; Dzikowska-Diduch, O.; Zdończyk, O.; Kozłowska, M.; Kostrubiec, M.; Ciurzyński, M.; Palczewski, P.; Grudzka, K.; et al. Echocardiographic Pattern of Acute Pulmonary Embolism: Analysis of 511 Consecutive Patients. J. Am. Soc. Echocardiogr. 2016, 29, 907–913. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.M.; Moumneh, T.; Penaloza, A.; Sanchez, O. Outpatient management of pulmonary embolism. Thromb. Res. 2017, 155, 92–100. [Google Scholar] [CrossRef]
- Elias, A.; Mallett, S.; Daoud-Elias, M.; Poggi, J.N.; Clarke, M. Prognostic models in acute pulmonary embolism: A systematic review and meta-analysis. BMJ Open 2016, 6, e010324. [Google Scholar] [CrossRef] [PubMed]
- Aujesky, D.; Roy, P.M.; Verschuren, F.; Righini, M.; Osterwalder, J.; Egloff, M.; Renaud, B.; Verhamme, P.; Stone, R.A.; Legall, C.; et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: An international, open-label, randomised, non-inferiority trial. Lancet 2011, 378, 41–48. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G.; Vedovati, M.C.; Pruszczyk, P.; Casazza, F.; Grifoni, S.; Salvi, A.; Bianchi, M.; Douma, R.; Konstantinides, S.; et al. Multidetector computed tomography for acute pulmonary embolism: Diagnosis and risk stratification in a single test. Eur. Heart J. 2011, 32, 1657–1663. [Google Scholar] [CrossRef]
- Pruszczyk, P.; Kurnicka, K.; Ciurzyński, M.; Hobohm, L.; Thielmann, A.; Sobkowicz, B.; Sawicka, E.; Kostrubiec, M.; Ptaszyńska-Kopczyńska, K.; Dzikowska-Diduch, O.; et al. Defining right ventricular dysfunction by echocardiography in normotensive patients with pulmonary embolism. Pol. Arch. Intern. Med. 2020, 130, 741–747. [Google Scholar] [CrossRef]
- Becattini, C.; Maraziti, G.; Vinson, D.R.; Ng, A.C.C.; den Exter, P.L.; Côté, B.; Vanni, S.; Doukky, R.; Khemasuwan, D.; Weekes, A.J.; et al. Right ventricle assessment in patients with pulmonary embolism at low risk for death based on clinical models: An individual patient data meta-analysis. Eur. Heart J. 2021, 42, 3190–3199. [Google Scholar] [CrossRef]
- El-Menyar, A.; Sathian, B.; Al-Thani, H. Elevated serum cardiac troponin and mortality in acute pulmonary embolism: Systematic review and meta-analysis. Respir. Med. 2019, 157, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Hakemi, E.U.; Alyousef, T.; Dang, G.; Hakmei, J.; Doukky, R. The prognostic value of undetectable highly sensitive cardiac troponin I in patients with acute pulmonary embolism. Chest 2015, 147, 685–694. [Google Scholar] [CrossRef]
- Becattini, C.; Lignani, A.; Masotti, L.; Forte, M.B.; Agnelli, G. D-dimer for risk stratification in patients with acute pulmonary embolism. J. Thromb. Thrombolysis 2012, 33, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.K.; Wu, H.; Xu, X.; Cao, H.; Wei, Q.; Wang, J.; Wang, X.; Zhang, X.; Tang, M.; Yang, S.; et al. Association between D-Dimer Level and In-Hospital Death of Pulmonary Embolism Patients. Dose Response 2020, 18, 1559325820968430. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.D.; Janjua, M.; Matta, F.; Alrifai, A.; Jaweesh, F.; Chughtai, H.L. Prognostic value of D-dimer in stable patients with pulmonary embolism. Clin. Appl. Thromb. Hemost. 2011, 17, E183–E185. [Google Scholar] [CrossRef]
- Pruszczyk, P.; Goliszek, S.; Lichodziejewska, B.; Kostrubiec, M.; Ciurzyński, M.; Kurnicka, K.; Dzikowska-Diduch, O.; Palczewski, P.; Wyzgal, A. Prognostic value of echocardiography in normotensive patients with acute pulmonary embolism. JACC Cardiovasc. Imaging 2014, 7, 553–560. [Google Scholar] [CrossRef]
- Jiménez, D.; Lobo, J.L.; Monreal, M.; Moores, L.; Oribe, M.; Barrón, M.; Otero, R.; Nauffal, D.; Rabuñal, R.; Valle, R.; et al. Prognostic significance of multidetector CT in normotensive patients with pulmonary embolism: Results of the protect study. Thorax 2014, 69, 109–115. [Google Scholar] [CrossRef]
- Côté, B.; Jiménez, D.; Planquette, B.; Roche, A.; Marey, J.; Pastré, J.; Meyer, G.; Sanchez, O. Prognostic value of right ventricular dilatation in patients with low-risk pulmonary embolism. Eur. Respir. J. 2017, 50, 1701611. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G.; Germini, F.; Vedovati, M.C. Computed tomography to assess risk of death in acute pulmonary embolism: A meta-analysis. Eur. Respir. J. 2014, 43, 1678–1690. [Google Scholar] [CrossRef]
- Trujillo-Santos, J.; den Exter, P.L.; Gómez, V.; Del Castillo, H.; Moreno, C.; van der Hulle, T.; Huisman, M.V.; Monreal, M.; Yusen, R.D.; Jiménez, D. Computed tomography-assessed right ventricular dysfunction and risk stratification of patients with acute non-massive pulmonary embolism: Systematic review and meta-analysis. J. Thromb. Haemost. 2013, 11, 1823–1832. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Non-CE (N = 405) | APE-Related Mortality, Embolectomy and Thrombolysis (N = 4) | All sPESI = 0 pts (N = 409) | p-Value | |
|---|---|---|---|---|
| Female/male | 197/208 | 2/2 | 199/210 | - |
| Age, years | 52 (39–66) | 73.5 (50–77.5) | 52 (39–66) | 0.12 |
| HR, 1 beat/min | 80 (70–90) | 92 (70–105) | 80 (70–90) | 0.4 |
| Systemic systolic blood pressure, mmHg | 130 (120–140) | 140 (120–155) | 130 (120–140) | 0.45 |
| Elevated troponin, n (%) | 122/405 (30%) | 4/4 (100%) | 126/409 (25.7%) | 0.008 |
| Troponin/ULN | 0.2 (0–1.3) | 7.8 (6.4–9.4) | 0.2 (0–1.36) | 0.000 |
| D-dimer, ng/mL | 4140 (1800–6631) | 20,680 (12,580–28,780) | 4169.6 (1839.5–6643.5) | 0.184 |
| RV/LV 4-chamber | 0.9 (0.8–1.00) | 1.0 (0.8–1.6) | 0.9 (0.8–1.0) | 0.27 |
| TRPG, mmHg | 25 (20–35.5) | 26.5 (17.5–38.5) | 25 (20–35.5) | 0.87 |
| RV/LV > 1.0 and/or TGPG >31 mmHg at echocardiography n (%) | 156/405 (38.5%) | 4/4 (100%) | 160/409 (39%) | 0.02 |
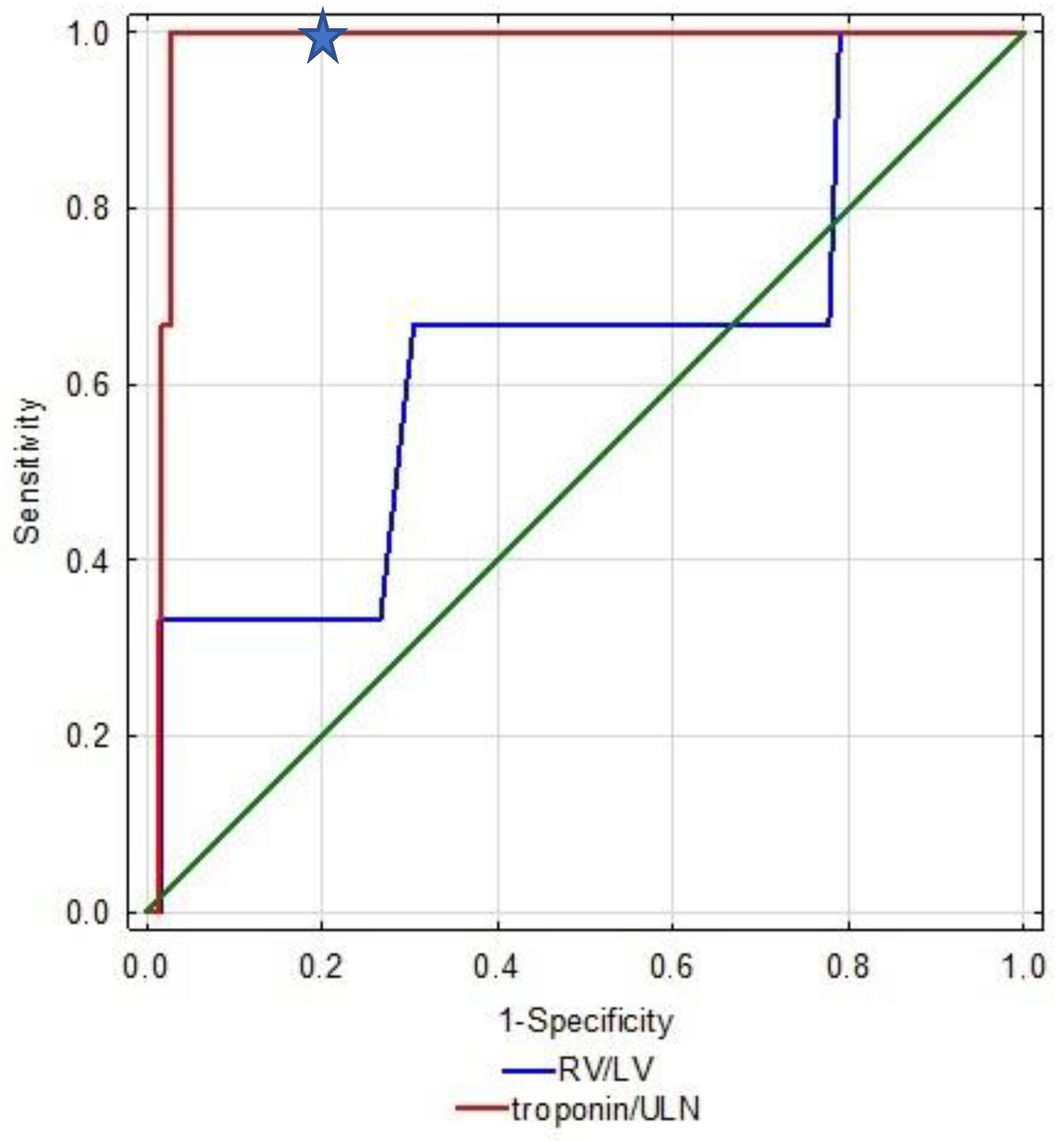
| Parameter | AUC | 95%CI | p-Value | Sensitivity | Specificity |
|---|---|---|---|---|---|
| Troponin/ULN | 0.908 | 0.831–0.984 | <0.001 | 100 | 79 |
| RV/LV > 1.0 | 0.725 | 0.417–0.999 | 0.15 | 75 | 69 |
| Parameter | OR | 95% CI | p |
|---|---|---|---|
| Troponin > 1.7 ULN | 26 | 1.34–513 | 0.03 |
| RV/LV > 1.0 | 4.6 | 0.41–51 | 0.21 |
| Parameter | Beta-Coefficient | Standard Error | OR 95% CI | p-Value |
|---|---|---|---|---|
| Troponin/ULN | 0.13 | 0.06 | 1.14 (1.11–1.29) | 0.03 |
| RV/LV > 1.0 | 2.48 | 2.24 | 11.9 (0.14–960) | 0.26 |
| Age | 0.03 | 0.044 | 1.14 (0.94–1.12) | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karolak, B.; Ciurzyński, M.; Skowrońska, M.; Kurnicka, K.; Pływaczewska, M.; Furdyna, A.; Perzanowska-Brzeszkiewicz, K.; Lichodziejewska, B.; Pacho, S.; Machowski, M.; et al. Plasma Troponins Identify Patients with Very Low-Risk Acute Pulmonary Embolism. J. Clin. Med. 2023, 12, 1276. https://doi.org/10.3390/jcm12041276
Karolak B, Ciurzyński M, Skowrońska M, Kurnicka K, Pływaczewska M, Furdyna A, Perzanowska-Brzeszkiewicz K, Lichodziejewska B, Pacho S, Machowski M, et al. Plasma Troponins Identify Patients with Very Low-Risk Acute Pulmonary Embolism. Journal of Clinical Medicine. 2023; 12(4):1276. https://doi.org/10.3390/jcm12041276
Chicago/Turabian StyleKarolak, Bartosz, Michał Ciurzyński, Marta Skowrońska, Katarzyna Kurnicka, Magdalena Pływaczewska, Aleksandra Furdyna, Katarzyna Perzanowska-Brzeszkiewicz, Barbara Lichodziejewska, Szymon Pacho, Michał Machowski, and et al. 2023. "Plasma Troponins Identify Patients with Very Low-Risk Acute Pulmonary Embolism" Journal of Clinical Medicine 12, no. 4: 1276. https://doi.org/10.3390/jcm12041276