
A Prospective Observational Study on Short and Long-Term Outcomes of COVID-19 Patients with Acute Hypoxic Respiratory Failure Treated with High-Flow Nasal Cannula
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
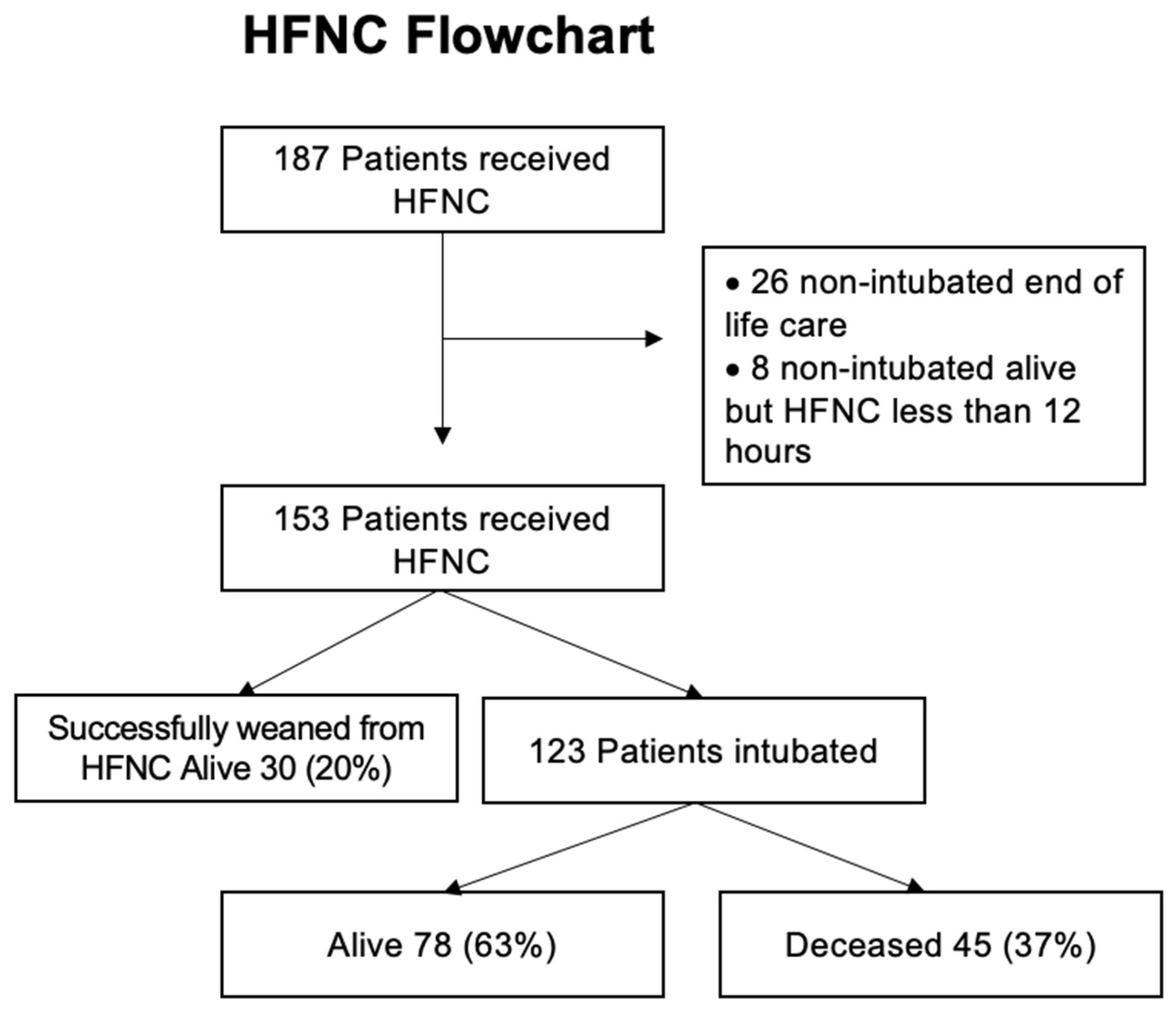
3.1. Short-Term Outcomes with HFNC on Intubation
3.2. Long-Term Survey
3.3. Predictors of HFNC Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Munshi, L.; Mancebo, J.; Brochard, L.J. Noninvasive Respiratory Support for Adults with Acute Respiratory Failure. N. Engl. J. Med. 2022, 387, 1688–1698. [Google Scholar] [CrossRef] [PubMed]
- Mauri, T.; Turrini, C.; Eronia, N.; Grasselli, G.; Volta, C.A.; Bellani, G.; Pesenti, A. Physiologic Effects of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 1207–1215. [Google Scholar] [CrossRef]
- Sztrymf, B.; Messika, J.; Bertrand, F.; Hurel, D.; Leon, R.; Dreyfuss, D.; Ricard, J.-D. Beneficial effects of humidified high flow nasal oxygen in critical care patients: A prospective pilot study. Intensive Care Med. 2011, 37, 1780–1786. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, Z.P.; Zazzeron, L.; Berra, L.; Hess, D.R.; Bittner, E.A.; Chang, M.G. Noninvasive respiratory support for COVID-19 patients: When, for whom, and how? J. Intensive Care. 2022, 10, 3. [Google Scholar] [CrossRef]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Møller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Natl. Inst. Health 2020, 2019, 130. [Google Scholar]
- Bellani, G.; Laffey, J.G.; Pham, T.; Madotto, F.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Bumbasirevic, V.; Piquilloud, L.; et al. Noninvasive Ventilation of Patients with Acute Respiratory Distress Syndrome. Insights from the LUNG SAFE Study. Am. J. Respir. Crit. Care Med. 2017, 195, 67–77. [Google Scholar] [CrossRef]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef]
- Mascheroni, D.; Kolobow, T.; Fumagalli, R.; Moretti, M.P.; Chen, V.; Buckhold, D. Acute respiratory failure following pharmacologically induced hyperventilation: An experimental animal study. Intensive Care Med. 1988, 15, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Shintani, A.K.; Hagerman, H.E.; St Jacques, P.J.; Rice, T.W.; Sanders, N.W.; Ware, L.B.; Bernard, G.R.; Ely, E.W. Derivation and validation of Spo2/Fio2 ratio to impute for Pao2/Fio2 ratio in the respiratory component of the Sequential Organ Failure Assessment score. Crit. Care Med. 2009, 37, 1317–1321. [Google Scholar] [CrossRef]
- Roca, O.; Caralt, B.; Messika, J.; Samper, M.; Sztrymf, B.; Hernández, G.; García-De-Acilu, M.; Frat, J.-P.; Masclans, J.R.; Ricard, J.-D. An Index Combining Respiratory Rate and Oxygenation to Predict Outcome of Nasal High-Flow Therapy. Am. J. Respir. Crit. Care Med. 2019, 199, 1368–1376. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Olde Hartman, T.C.; Rosmalen, J.G.M. Lifelines Corona Research Initiative. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef]
- Li, M.D.; Arun, N.T.; Gidwani, M.; Chang, K.; Deng, F.; Little, B.P.; Mendoza, D.P.; Lang, M.; Lee, S.I.; O’Shea, A.; et al. Automated Assessment and Tracking of COVID-19 Pulmonary Disease Severity on Chest Radiographs using Convolutional Siamese Neural Networks. Radiol. Artif. Intell. 2020, 2, e200079. [Google Scholar] [CrossRef] [PubMed]
- Li, M.D.; Arun, N.T.; Aggarwal, M.; Gupta, S.; Singh, P.; Little, B.P.; Mendoza, D.P.; Corradi, G.C.; Takahashi, M.S.; Ferraciolli, S.F.; et al. Improvement and Multi-Population Generalizability of a Deep Learning-Based Chest Radiograph Severity Score for COVID-19. Preprint. medRxiv 2020. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Roca, O.; Riera, J.; Torres, F.; Masclans, J.R. High-flow oxygen therapy in acute respiratory failure. Respir. Care 2010, 55, 408–413. [Google Scholar]
- Dysart, K.; Miller, T.L.; Wolfson, M.R.; Shaffer, T.H. Research in high flow therapy: Mechanisms of action. Respir Med. 2009, 103, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Goodman, A.B.; Belay, B.; Freedman, D.S.; Sucosky, M.S.; Lange, S.J.; Gundlapalli, A.V.; Boehmer, T.K.; Blanck, H.M. Body Mass Index and Risk for COVID-19-Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death-United States, March-December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 355–361. [Google Scholar] [CrossRef]
- Chandel, A.; Patolia, S.; Brown, A.W.; Collins, A.C.; Sahjwani, D.; Khangoora, V.; Cameron, P.C.; Desai, M.; Kasarabada, A.; Kilcullen, J.K.; et al. High-Flow Nasal Cannula Therapy in COVID-19: Using the ROX Index to Predict Success. Respir. Care 2021, 66, 909–919. [Google Scholar] [CrossRef]
- Prakash, J.; Bhattacharya, P.K.; Yadav, A.K.; Kumar, A.; Tudu, L.C.; Prasad, K. ROX index as a good predictor of high flow nasal cannula failure in COVID-19 patients with acute hypoxemic respiratory failure: A systematic review and meta-analysis. J. Crit. Care 2021, 66, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.V.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.S.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All Subjects | Success (Weaned off HFNC) | Failure (Required Intubation) | p | |
|---|---|---|---|---|
| Long term survey | ||||
| Discharge from hospital alive, n | 108 | 30 | 78 | |
| Alive at 6-month follow-up, n (%discharged) | 104 (96) | 29 (97) | 75 (96) | 0.90 |
| Age deceased, years | ||||
| Median (IQR) | 67.5 (57–73) | 67 | 68 (53–75) | |
| Job before hospital, tot | 78 | 25 | 53 | |
| Y, n (%) | 40 (51) | 15 (60) | 25 (47) | 0.29 |
| Back to work, tot | 40 | 15 | 25 | |
| Y, n (%) | 24 (60) | 10 (66) | 14 (56) | 0.50 |
| Days back, tot | 19 | 7 | 12 | |
| Median (IQR) | 30 (15–60) | 75 (38–143) | 0.03 | |
| New problem after discharge, tot | 82 | 25 | 57 | |
| Y, n (%) | 61 (74) | 15 (60) | 46 (81) | 0.048 |
| Quality of life equal similar, tot | 78 | 25 | 57 | |
| Y, n (%) | 31 (40) | 12 (48) | 19 (36) | 0.31 |
| Able to walk 1–2 flight of stairs, tot | 79 | 25 | 54 | |
| Y, n (%) | 29 (37) | 13 (52) | 16 (30) | 0.06 |
| Any new medications, (tot) | 76 | 24 | 52 | |
| Y, n (%) | 41 (54) | 10 (42) | 31 (60) | 0.14 |
| New medical conditions, tot | 80 | 24 | 56 | |
| Y, n (%) | 26 (33) | 7 (29) | 19 (34) | 0.68 |
| Limitations before, tot | 80 | 26 | 54 | |
| Y, n (%) | 12 (15) | 4 (15) | 8 (15) | >0.95 |
| New limitations, tot | 67 | 21 | 46 | |
| Y, n (%) | 26 (39) | 7 (33) | 19 (41) | 0.53 |
| Katz, tot | 20 | 6 | 14 | |
| Median (IQR) | 4.5 (4–6) | 6 (4–6) | 0.37 | |
| New oxygen supplementation, tot | 81 | 25 | 56 | |
| Y, n (%) | 13 (16) | 3 (12) | 10 (18) | 0.51 |
| Breathing problem, tot | 76 | 24 | 52 | |
| Y, n (%) | 35 (46) | 11 (46) | 24 (46) | 0.98 |
| Sensory loss, tot | 70 | 24 | 46 | |
| Y, n (%) | 32 (46) | 9 (38) | 23 (50) | 0.71 |
| Motor deficit, tot | 74 | 24 | 50 | |
| Y, n (%) | 36 (49) | 11 (46) | 25 (50) | 0.74 |
| Hospital readmission, tot | 87 | 26 | 61 | |
| Y, n (%) | 29 (33) | 8 (31) | 21 (34) | 0.74 |
| Medical reason, tot | 29 | 8 | 21 | |
| n (%) | 23 (79) | 6 (75) | 17 (81) | 0.72 |
| Reintubated, tot | 29 | 8 | 21 | |
| n (%) | 2 (7) | 1 (13) | 1 (5) | 0.46 |
| Covariate | n/Total N (%) | Unadjusted | Adjusted | ||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Age, years | 0.67 (0.48, 0.91) | 0.02 | 0.79 (0.53, 1.15) a | 0.24 | |
| Sex | |||||
| Male | 23/46(50.0) | 4.50 (1.64, 13.93) | 0.005 | 4.65 (1.28, 20.6) | 0.03 |
| Female | 6/33(18.2) | Reference (1.00) | Reference (1.00) | ||
| Body Mass Index, kg/m2 | 1.5 (0.86, 2.71) | 0.16 | 2.63 (1.14, 6.76) b | 0.03 | |
| Asthma | |||||
| Yes | 3/18(16.7) | 0.27 (0.06, 0.93) | 0.057 | 0.21 (0.03, 1.01) | 0.07 |
| No | 25/59(42.4) | Reference (1.00) | Reference (1.00) | ||
| Diabetes Mellitus | |||||
| Yes | 9/35 (25.7) | 0.40 (0.15, 1.03) | 0.06 | 0.34 (0.09, 1.10) | 0.08 |
| No | 20/43 (46.5) | Reference (1.00) | Reference (1.00) | ||
| Intubation during hospitalization | |||||
| Yes | 16/54(29.6) | 0.40 (0.14, 1.03) | 0.058 | 0.39 (0.11, 1.31) | 0.13 |
| No | 13/25 (52.0) | Reference (1.00) | Reference (1.00) | ||
| HFNC Success | HFNC Failure | p | |
|---|---|---|---|
| Demographic information, body max index and HFNC duration | |||
| Subject, n (%) | 30 (19.6) | 123 (80.4) | |
| Age, y | 62 ± 20 | 66 ± 13 | 0.23 |
| Gender (female) n (% | 9 (30) | 47 (38) | 0.4 |
| Race, non-White, n (%) | 14 (47) | 61 (50) | 0.99 |
| Ethnicity non-Hispanic, n (%) | 19 (63) | 72 (59) | 0.76 |
| Body mass index, kg/m2 | 27.5 (23.3–35.1) | 29.6 (26.1–34.3) | 0.45 |
| HFNC duration, hours | 68.5 (28.5–111) | 12 (3–28) | <0.01 |
| Comorbidities | |||
| No comorbid disease, n (%) | 6 (20) | 6 (5) | <0.01 |
| Hypertension, n (%) | 19 (63) | 94 (80) | 0.06 |
| Diabetes mellitus, n (%) | 11 (27) | 62 (53) | 0.01 |
| Chronic kidney disease, n (%) | 6 (17) | 30 (26) | 0.52 |
| Asthma, n (%) | 6 (20) | 23 (20) | 0.98 |
| COPD, n (%) | 5 (17) | 14 (12) | 0.52 |
| Active cancer, n (%) | 6 (20) | 20 (17) | 0.74 |
| HFrEF, n (%) | 2 (7) | 10 (9) | 0.71 |
| Coronary artery disease, n (%) | 4 (13) | 26 (23) | 0.25 |
| Vital signs and x-ray findings | |||
| Oxygen saturation, (%) | 93.5 (91–95) | 93 (90–96) | 0.78 |
| Respiratory rate, breaths/min | 26.5 (22.5–30) | 32 (26–38) | <0.01 |
| FiO2 before HFNC (%) | 90 (45–90) | 90 (72–90) | 0.02 |
| Heart rate, beats/min | 85 ±15 | 89 ±20 | 0.29 |
| Mean arterial pressure, mmHg | 86 (83–101) | 89 (82–97) | 0.83 |
| SpO2/FiO2 | 110 (102–203.5) | 106 (100–132) | 0.03 |
| Last SpO2/FiO2 during HFNC | 193 (143–238) | 99 (95–137) | <0.01 |
| Pulmonary x-ray severity (PXS) score, severe (%) | 9 (33) | 34 (39) | 0.84 |
| Modified SOFA Score | 4 (3–6.75) | 4 (3–5) | 0.359 |
| Laboratory values | |||
| Creatinine | 0.83 (0.67–1) | 1 (0.82–1.44) | <0.01 |
| Urea | 22 (14–26) | 21 (16–37) | 0.19 |
| White blood cells | 8.36 (5.38–11.45) | 9.46 (6.27–12.48) | 0.23 |
| Platelets | 259 (189–325) | 223 (167–279) | 0.09 |
| Bilirubin | 0.4 (0.3–0.6) | 0.5 (0.4–0.6) | 0.07 |
| C-reactive protein | 102.6 (70.7–245.3) | 141.5 (73.7–218.6) | 0.64 |
| Variable | Time (h) | Success (n = 30) | Failure (n = 123) | p |
|---|---|---|---|---|
| Respiratory rate, breath/min | 2 | 25 (22–33) | 30 (23–35) | 0.21 |
| 6 | 25 (22–30) | 27 (22–31) | 0.29 | |
| 12 | 23 (20–25) | 26 (23–31) | <0.01 | |
| 24 | 21 (19–28) | 24 (20–31) | 0.20 | |
| SpO2, % | 2 | 96 (95–98) | 96 (94–97) | 0.23 |
| 6 | 96 (94–98) | 94 (92–97) | 0.04 | |
| 12 | 95 (94–97) | 95 (94–97) | 0.77 | |
| 24 | 95 (94–97) | 96 (93–97) | 0.90 | |
| FiO2, % | 2 | 69 (60–100) | 100 (80–100) | <0.01 |
| 6 | 60 (50–88) | 85 (70–100) | <0.01 | |
| 12 | 55 (40–70) | 80 (70–90) | <0.01 | |
| 24 | 50 (40–70) | 75 (63–100) | <0.01 | |
| ROX Index | 2 | 4.85 (3.65–6.73) | 3.7 (3–4.9) | <0.01 |
| 6 | 6.75 (4–7.88) | 4.6 (3.3–5.65) | <0.01 | |
| 12 | 8.15 (5.78–10.65) | 4.65 (3.78–5.95) | <0.01 | |
| 24 | 7.2 (6.1–10.38) | 5 (3.23–6.95) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medeiros, K.J.; Valsecchi, C.; Winterton, D.; Morais, C.A.; Delgado, E.D.; Smith, S.; Safaee Fakhr, B.; Ranjeva, S.; Capriles, M.; Gaulton, T.; et al. A Prospective Observational Study on Short and Long-Term Outcomes of COVID-19 Patients with Acute Hypoxic Respiratory Failure Treated with High-Flow Nasal Cannula. J. Clin. Med. 2023, 12, 1249. https://doi.org/10.3390/jcm12041249
Medeiros KJ, Valsecchi C, Winterton D, Morais CA, Delgado ED, Smith S, Safaee Fakhr B, Ranjeva S, Capriles M, Gaulton T, et al. A Prospective Observational Study on Short and Long-Term Outcomes of COVID-19 Patients with Acute Hypoxic Respiratory Failure Treated with High-Flow Nasal Cannula. Journal of Clinical Medicine. 2023; 12(4):1249. https://doi.org/10.3390/jcm12041249
Chicago/Turabian StyleMedeiros, Kyle J., Carlo Valsecchi, Dario Winterton, Caio A. Morais, Eduardo Diaz Delgado, Shaun Smith, Bijan Safaee Fakhr, Sylvia Ranjeva, Martin Capriles, Timothy Gaulton, and et al. 2023. "A Prospective Observational Study on Short and Long-Term Outcomes of COVID-19 Patients with Acute Hypoxic Respiratory Failure Treated with High-Flow Nasal Cannula" Journal of Clinical Medicine 12, no. 4: 1249. https://doi.org/10.3390/jcm12041249