
Investigating the Ischaemic Phase of Skin NADH Fluorescence Dynamics in Recently Diagnosed Primary Hypertension: A Time Series Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Flow Mediated Skin Fluorescence
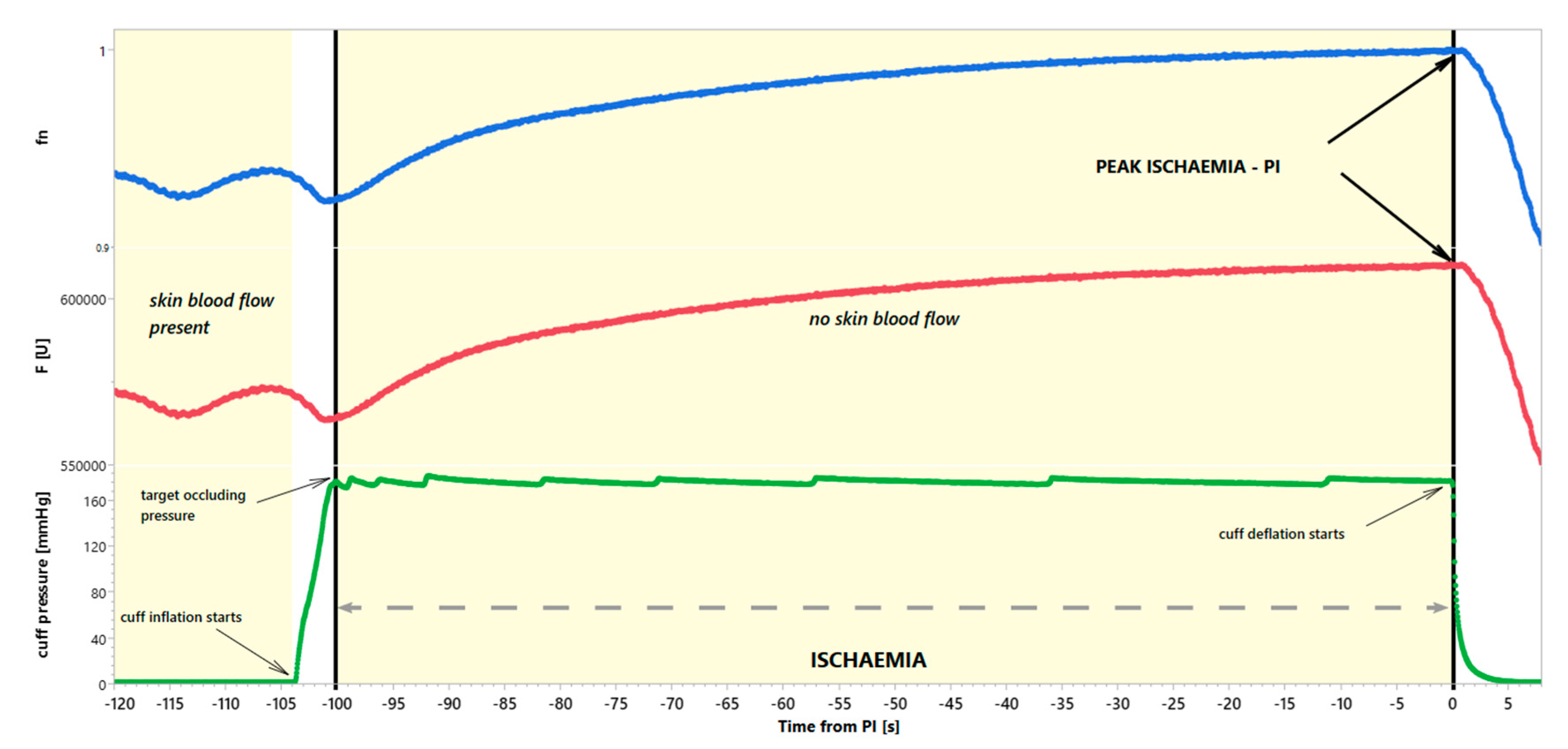
2.2. The Ischaemic Phase of the 460 nm Forearm Skin Fluorescence
2.3. Estimation of Sample Size
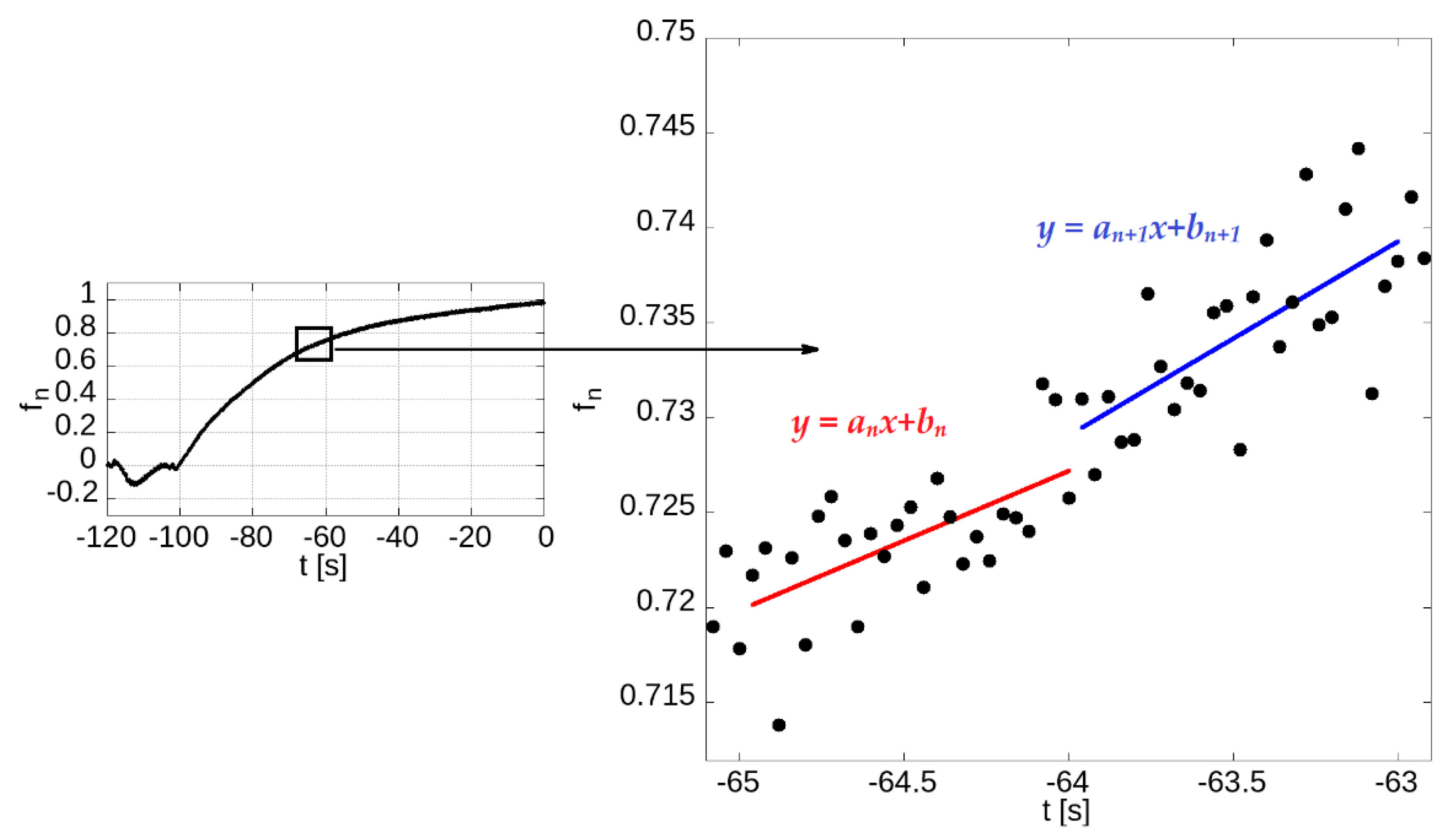
2.4. Statistical Analysis
2.5. Ethics Approval Statement
3. Results
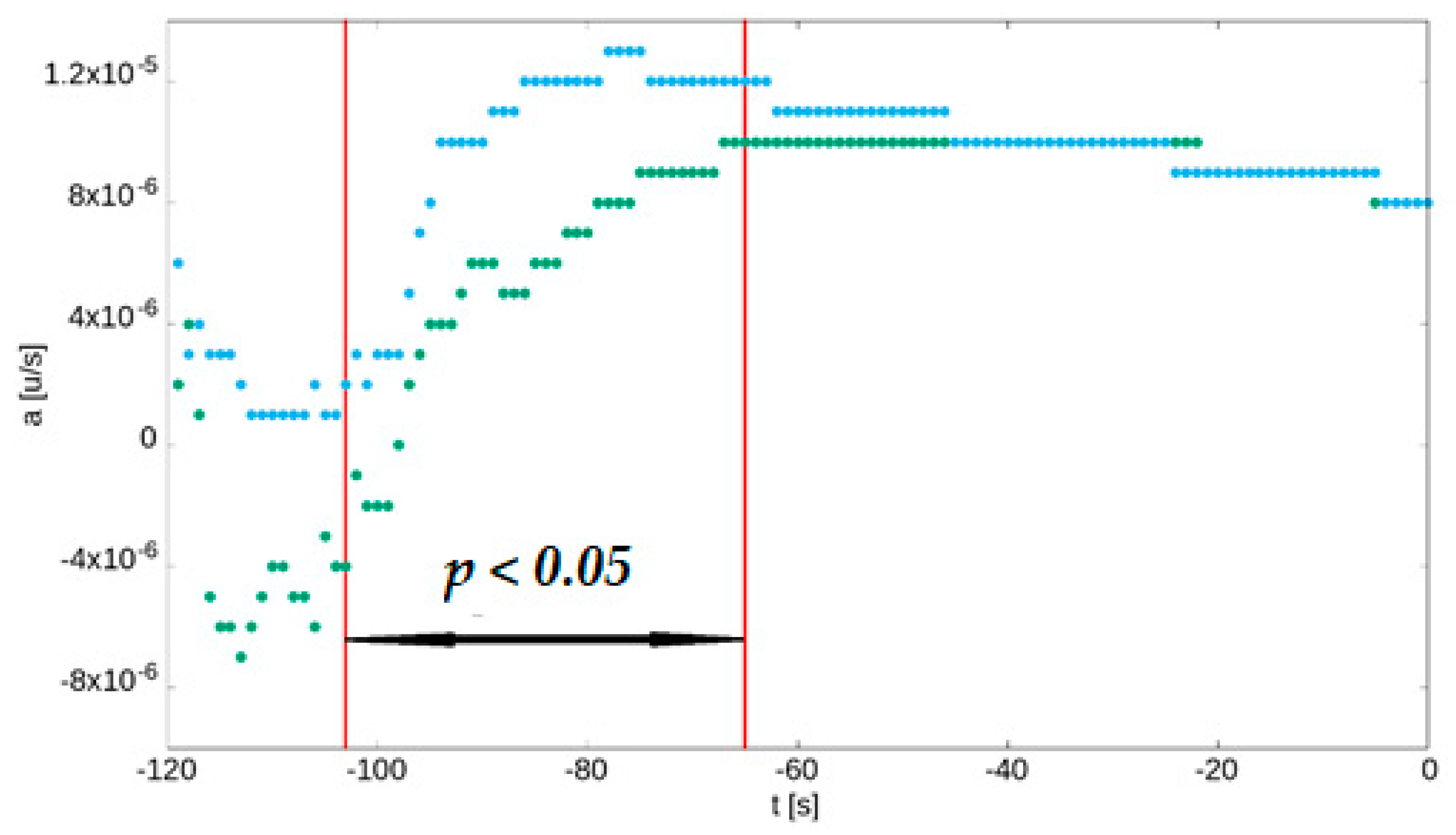
Ischaemia-Related Dynamic Changes in the FMSF Signal
4. Discussion
4.1. Study Limitations
4.2. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESHGuidelines for themanagement of arterial hypertension. J. Hypertens. 2018, 36, 1956–2041. [Google Scholar]
- Flammer, A.J.; Anderson, T.; Celermajer, D.S.; Creager, M.A.; Deanfield, J.; Ganz, P.; Hamburg, N.; Lüscher, T.F.; Shechter, M.; Taddei, S.; et al. The assessment of endothelial function: From research into clinical practice. Circulation 2012, 126, 753–767. [Google Scholar] [CrossRef]
- Dikalov, S.; Dikalova, A. Mitochondrial deacetylase Sirt3 in vascular dysfunction and hypertension. Curr. Opin. Nephrol. Hypertens. 2022, 31, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Nunnari, J.; Suomalainen, A. Mitochondria: In sickness and in health. Cell 2012, 148, 1145–1159. Available online: https://pubmed.ncbi.nlm.nih.gov/22424226/ (accessed on 28 September 2022). [CrossRef] [PubMed]
- Annesley, S.J.; Fisher, P.R. Mitochondria in Health and Disease. Cells 2019, 8, 680. Available online: https://pubmed.ncbi.nlm.nih.gov/31284394/ (accessed on 28 September 2022). [CrossRef] [PubMed]
- Balu, M.; Mazhar, A.; Hayakawa, C.K.; Mittal, R.; Krasieva, T.B.; König, K.; Venugopalan, V.; Tromberg, B.J. In vivo multiphoton NADH fluorescence reveals depth-dependent keratinocyte metabolism in human skin. Biophys. J. 2013, 104, 258–267. [Google Scholar] [CrossRef]
- Gȩbicki, J.; Marcinek, A.; Zielonka, J. Transient Species in the Stepwise Interconversion of NADH and NAD+. Accounts Chem. Res. 2004, 37, 379–386. [Google Scholar] [CrossRef]
- Bugaj, O.; Zieliński, J.; Kusy, K.; Kantanista, A.; Wielinski, D.; Guzik, P. The Effect of Exercise on the Skin Content of the Reduced Form of NAD and Its Response to Transient Ischemia and Reperfusion in Highly Trained Athletes. Front. Physiol. 2019, 10, 600. [Google Scholar] [CrossRef]
- Piotrowski, L.; Urbaniak, M.; Jedrzejczak, B.; Marcinek, A.; Gebicki, J. Note: Flow mediated skin fluorescence—A novel technique for evaluation of cutaneous microcirculation. Rev. Sci. Instrum. 2016, 87, 036111. [Google Scholar] [CrossRef]
- Bogaczewicz, J.; Tokarska, K.; Wozniacka, A. Changes of NADH Fluorescence from the Skin of Patients with Systemic Lupus Erythematosus. BioMed Res. Int. 2019, 2019, 5897487. Available online: https://pubmed.ncbi.nlm.nih.gov/31930128/ (accessed on 26 October 2022). [CrossRef]
- Pawlak-Chomicka, R.; Krauze, T.; Uruski, P.; Piskorski, J.; Wykretowicz, A.; Tykarski, A.; Guzik, P. The Effect of Antihypertensive Drugs on NADH in Newly Diagnosed Primary Hypertension. Cardiol. Res. Pract. 2022, 2022, 6159883. Available online: https://pubmed.ncbi.nlm.nih.gov/35402043/ (accessed on 28 September 2022). [CrossRef] [PubMed]
- Tarnawska, M.; Dorniak, K.; Kaszubowski, M.; Dudziak, M.; Hellmann, M. A pilot study with flow mediated skin fluorescence: A novel device to assess microvascular endothelial function in coronary artery disease. Cardiol. J. 2018, 25, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Katarzynska, J.; Borkowska, A.; Czajkowski, P.; Los, A.; Szczerbinski, L.; Milewska-Kranc, A.; Marcinek, A.; Kretowski, A.; Cypryk, K.; Gebicki, J. Flow Mediated Skin Fluorescence technique reveals remarkable effect of age on microcirculation and metabolic regulation in type 1 diabetes. Microvasc. Res. 2019, 124, 19–24. [Google Scholar] [CrossRef]
- Majewski, S.; Szewczyk, K.; Białas, A.J.; Miłkowska-Dymanowska, J.; Kurmanowska, Z.; Górski, P. Assessment of microvascular function in vivo using flow mediated skin fluorescence (FMSF) in patients with obstructive lung diseases: A preliminary study. Microvasc. Res. 2019, 127, 103914. [Google Scholar] [CrossRef] [PubMed]
- Bugaj, O.; Kusy, K.; Kantanista, A.; Korman, P.; Wieliński, D.; Zieliński, J. The Effect of a 7-Week Training Period on Changes in Skin NADH Fluorescence in Highly Trained Athletes. Appl. Sci. 2020, 10, 5133. [Google Scholar] [CrossRef]
- Nizinski, J.; Kamieniarz, L.; Filberek, P.; Sibrecht, G.; Guzik, P. Monitoring the skin NADH changes during ischaemia and reperfusion in humans. J. Med. Sci. 2020, 89, e405. [Google Scholar] [CrossRef]
- Nizinski, J.; Filberek, P.; Sibrecht, G.; Krauze, T.; Zielinski, J.; Piskorski, J.; Wykretowicz, A.; Guzik, P. Non-invasive in vivo human model of post ischaemic skin preconditioning by measurement of flow-mediated 460-nm autofluorescence. Br. J. Clin. Pharmacol. 2021, 87, 4283–4292. Available online: https://pubmed.ncbi.nlm.nih.gov/33792076/ (accessed on 20 April 2021). [CrossRef]
- Hellmann, M.; Tarnawska, M.; Dudziak, M.; Dorniak, K.; Roustit, M.; Cracowski, J.-L. Reproducibility of flow mediated skin fluorescence to assess microvascular function. Microvasc. Res. 2017, 113, 60–64. [Google Scholar] [CrossRef]
- Feihl, F.; Liaudet, L.; Waeber, B.; Levy, B.I. Hypertension: A disease of the microcirculation? Hypertension 2006, 48, 1012–1017. [Google Scholar] [CrossRef]
- Krzemińska, J.; Wronka, M.; Młynarska, E.; Franczyk, B.; Rysz, J. Arterial Hypertension—Oxidative Stress and Inflammation. Antioxidants 2022, 11, 172. [Google Scholar] [CrossRef]
- Holowatz, L.A.; Kenney, W.L. Up-regulation of arginase activity contributes to attenuated reflex cutaneous vasodilatation in hypertensive humans. J. Physiol. 2007, 581, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Baldini, N.; Avnet, S. The Effects of Systemic and Local Acidosis on Insulin Resistance and Signaling. Int. J. Mol. Sci. 2018, 20, 126. [Google Scholar] [CrossRef] [PubMed]
- Ertuglu, L.A.; Elijovich, F.; Laffer, C.L.; Kirabo, A. Salt-Sensitivity of Blood Pressure and Insulin Resistance. Front. Physiol. 2021, 12, 793924. [Google Scholar] [CrossRef]
- Sinha, S.; Haque, M. Insulin Resistance Is Cheerfully Hitched with Hypertension. Life 2022, 12, 564. [Google Scholar] [CrossRef]
- Eirin, A.; Lerman, A.; Lerman, L.O. Enhancing Mitochondrial Health to Treat Hypertension. Curr. Hypertens. Rep. 2018, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Forte, M.; Stanzione, R.; Cotugno, M.; Bianchi, F.; Marchitti, S.; Rubattu, S. Vascular ageing in hypertension: Focus on mitochondria. Mech. Ageing Dev. 2020, 189, 111267. [Google Scholar] [CrossRef] [PubMed]
- Dikalova, A.E.; Pandey, A.; Xiao, L.; Arslanbaeva, L.; Sidorova, T.; Lopez, M.G.; Billings, F.T.; Verdin, E.; Auwerx, J.; Harrison, D.G.; et al. Mitochondrial Deacetylase Sirt3 Reduces Vascular Dysfunction and Hypertension While Sirt3 Depletion in Essential Hypertension Is Linked to Vascular Inflammation and Oxidative Stress. Circ. Res. 2020, 126, 439–452. [Google Scholar] [CrossRef]
- Baltatu, O.C.; Amaral, F.G.; Campos, L.A.; Cipolla-Neto, J. Melatonin, mitochondria and hypertension. Cell. Mol. Life Sci. 2017, 74, 3955–3964. [Google Scholar] [CrossRef]
- Mayevsky, A.; Chance, B. Oxidation–reduction states of NADH in vivo: From animals to clinical use. Mitochondrion 2007, 7, 330–339. [Google Scholar] [CrossRef]
- Chan, S.H.; Chan, J.Y. Mitochondria and Reactive Oxygen Species Contribute to Neurogenic Hypertension. Physiology 2017, 32, 308–321. [Google Scholar] [CrossRef]
- Dikalova, A.E.; Itani, H.A.; Nazarewicz, R.R.; McMaster, W.G.; Flynn, C.R.; Uzhachenko, R.; Fessel, J.P.; Gamboa, J.L.; Harrison, D.G.; Dikalov, S.I.; et al. Sirt3 Impairment and SOD2 Hyperacetylation in Vascular Oxidative Stress and Hypertension. Circ. Res. 2017, 121, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Mayevsky, A.; Rogatsky, G.G. Mitochondrial function in vivo evaluated by NADH fluorescence: From animal models to human studies. Am. J. Physiol. Physiol. 2007, 292, C615–C640. [Google Scholar] [CrossRef] [PubMed]
- Kléber, A.G.; Riegger, C.B.; Janse, M.J. Extracellular K+ and H+ shifts in early ischemia: Mechanisms and relation to changes in impulse propagation. J. Mol. Cell. Cardiol. 1987, 19, 35–44. [Google Scholar] [CrossRef]
- Theodorakopoulou, M.P.; Bakaloudi, D.R.; Dipla, K.; Zafeiridis, A.; Boutou, A.K. Vascular endothelial damage in COPD: Current functional assessment methods and future perspectives. Expert Rev. Respir. Med. 2021, 15, 1121–1133. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control Group n =16 | Patients with HA n = 65 | p-Value (Mann-Whitney Test) | |||
|---|---|---|---|---|---|
| Median | Q1–Q3 | Median | Q1–Q3 | ||
| SBP WT [mmHg] | 129 | 122–133 | 148 | 143–156 | <0.01 |
| DBP WT [mmHg] | 79 | 76–83 | 88 | 84–93 | <0.01 |
| HR WT [beats/min] | 82 | 77–93 | 82 | 76–90 | 0.96 |
| SBP ST [mmHg] | 105 | 102–112 | 122 | 113–131 | <0.01 |
| DBP ST [mmHg] | 63 | 58–69 | 70 | 66–77 | <0.01 |
| HR ST [beats/min] | 63 | 60–69 | 65 | 60–73 | 0.64 |
| SBP 24-h [mmHg] | 125 | 117–127 | 143 | 138–149 | <0.01 |
| DBP 24-h [mmHg] | 76 | 71–79 | 84 | 81–90 | <0.01 |
| HR 24-h [beats/min] | 77 | 74–87 | 79 | 74–85 | 0.91 |
| Baseline fluorescence [kU] | 876 | 556–1010 | 687 | 495–846 | 0.17 |
| Peak ischaemic fluorescence [kU] | 966 | 604–1096 | 744 | 536–909 | 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawlak-Chomicka, R.; Chomicki, W.; Krauze, T.; Uruski, P.; Guzik, M.; Piskorski, J.; Tykarski, A.; Guzik, P. Investigating the Ischaemic Phase of Skin NADH Fluorescence Dynamics in Recently Diagnosed Primary Hypertension: A Time Series Analysis. J. Clin. Med. 2023, 12, 1247. https://doi.org/10.3390/jcm12041247
Pawlak-Chomicka R, Chomicki W, Krauze T, Uruski P, Guzik M, Piskorski J, Tykarski A, Guzik P. Investigating the Ischaemic Phase of Skin NADH Fluorescence Dynamics in Recently Diagnosed Primary Hypertension: A Time Series Analysis. Journal of Clinical Medicine. 2023; 12(4):1247. https://doi.org/10.3390/jcm12041247
Chicago/Turabian StylePawlak-Chomicka, Regina, Wojciech Chomicki, Tomasz Krauze, Paweł Uruski, Maria Guzik, Jarosław Piskorski, Andrzej Tykarski, and Przemysław Guzik. 2023. "Investigating the Ischaemic Phase of Skin NADH Fluorescence Dynamics in Recently Diagnosed Primary Hypertension: A Time Series Analysis" Journal of Clinical Medicine 12, no. 4: 1247. https://doi.org/10.3390/jcm12041247