
Comparison of Virtual Intersection and Occlusal Contacts between Intraoral and Laboratory Scans: An In-Vivo Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Implant Placement and Restoration
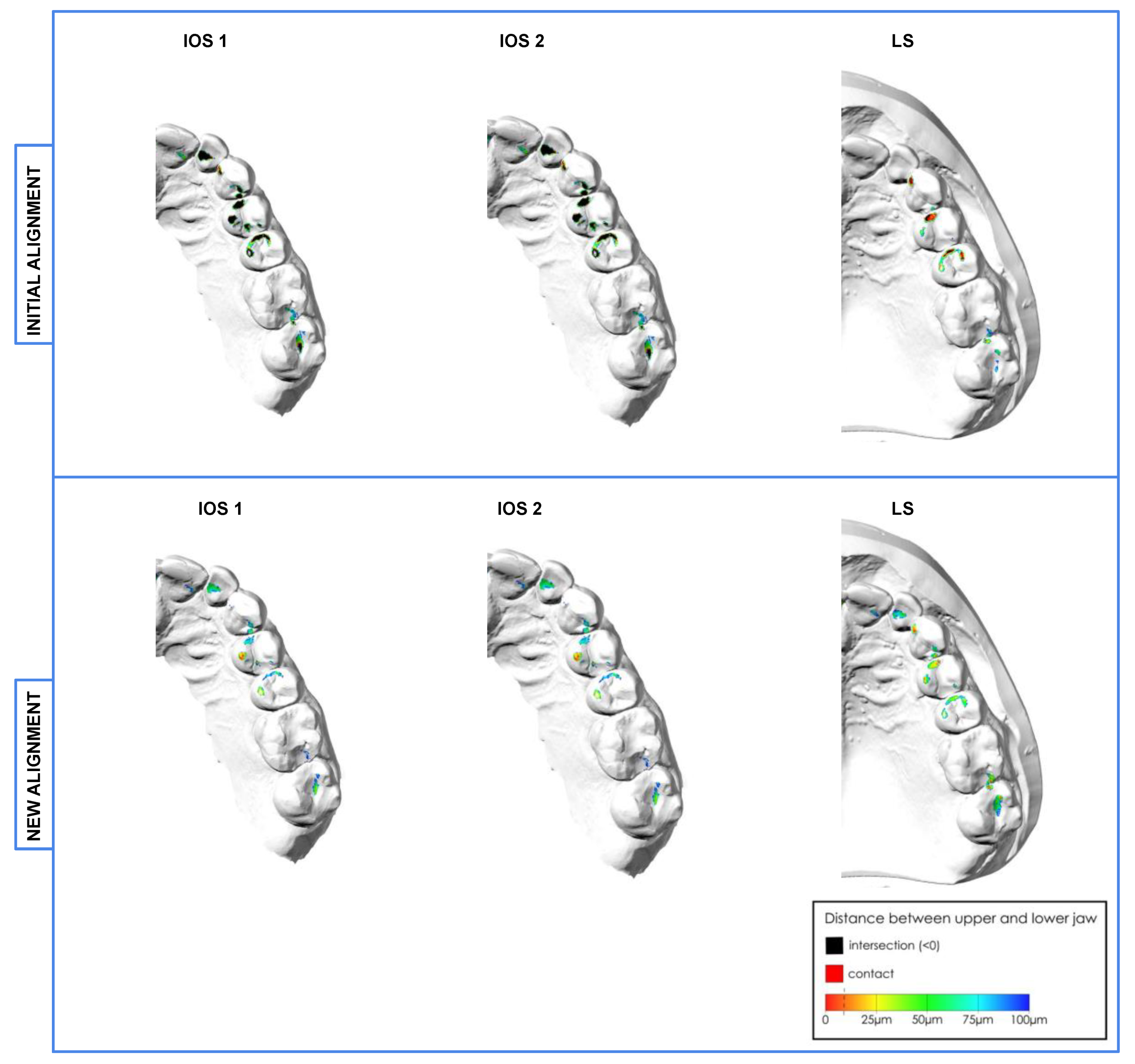
2.3. Initial Alignment of the Scans
2.4. New Alignment of the Scans
2.5. Measurement of Intersections and Occlusal Contacts
2.6. Statistical Analysis
3. Results
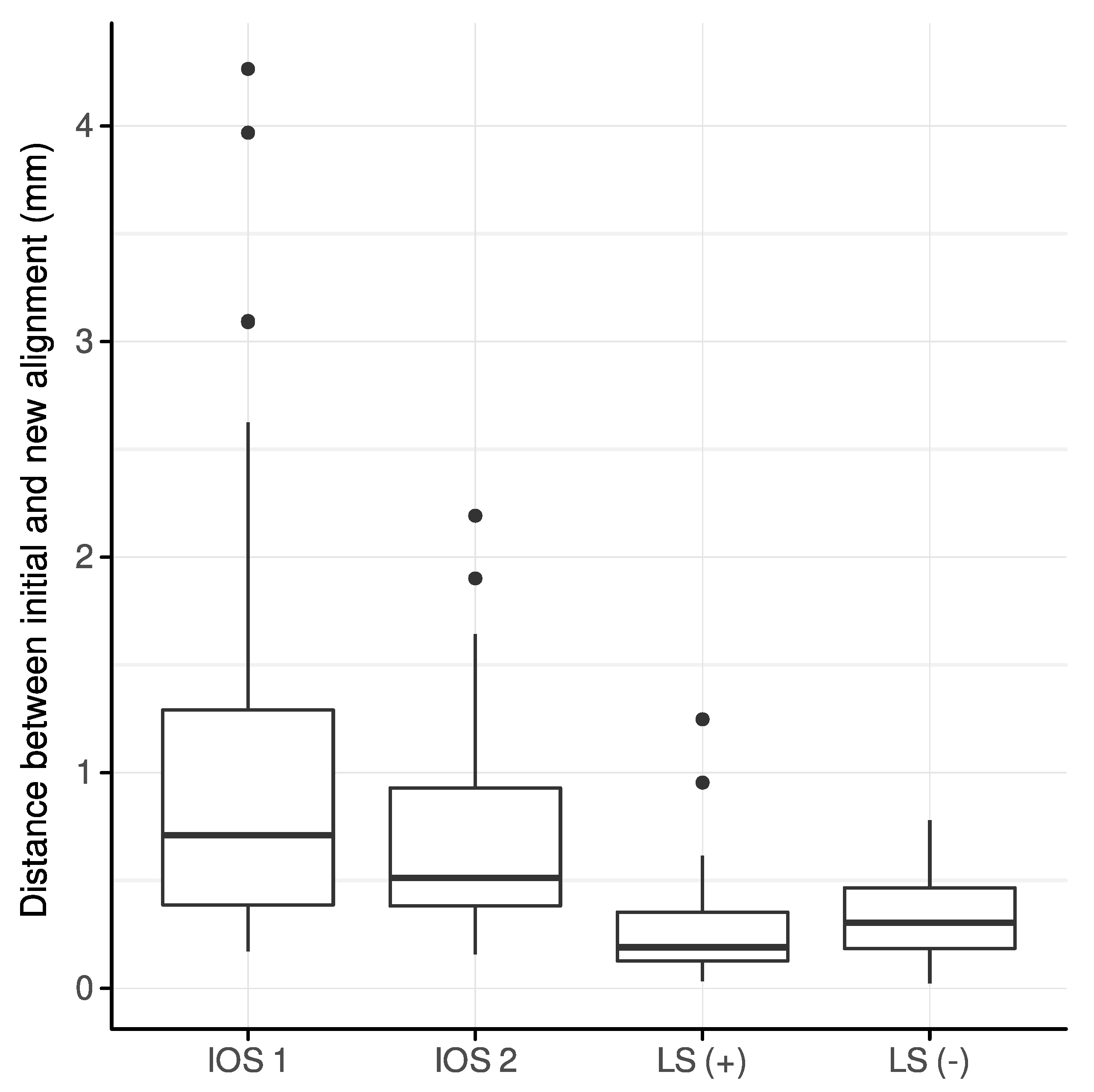
3.1. Interocclusal Distances between Initially and Newly Aligned Scans
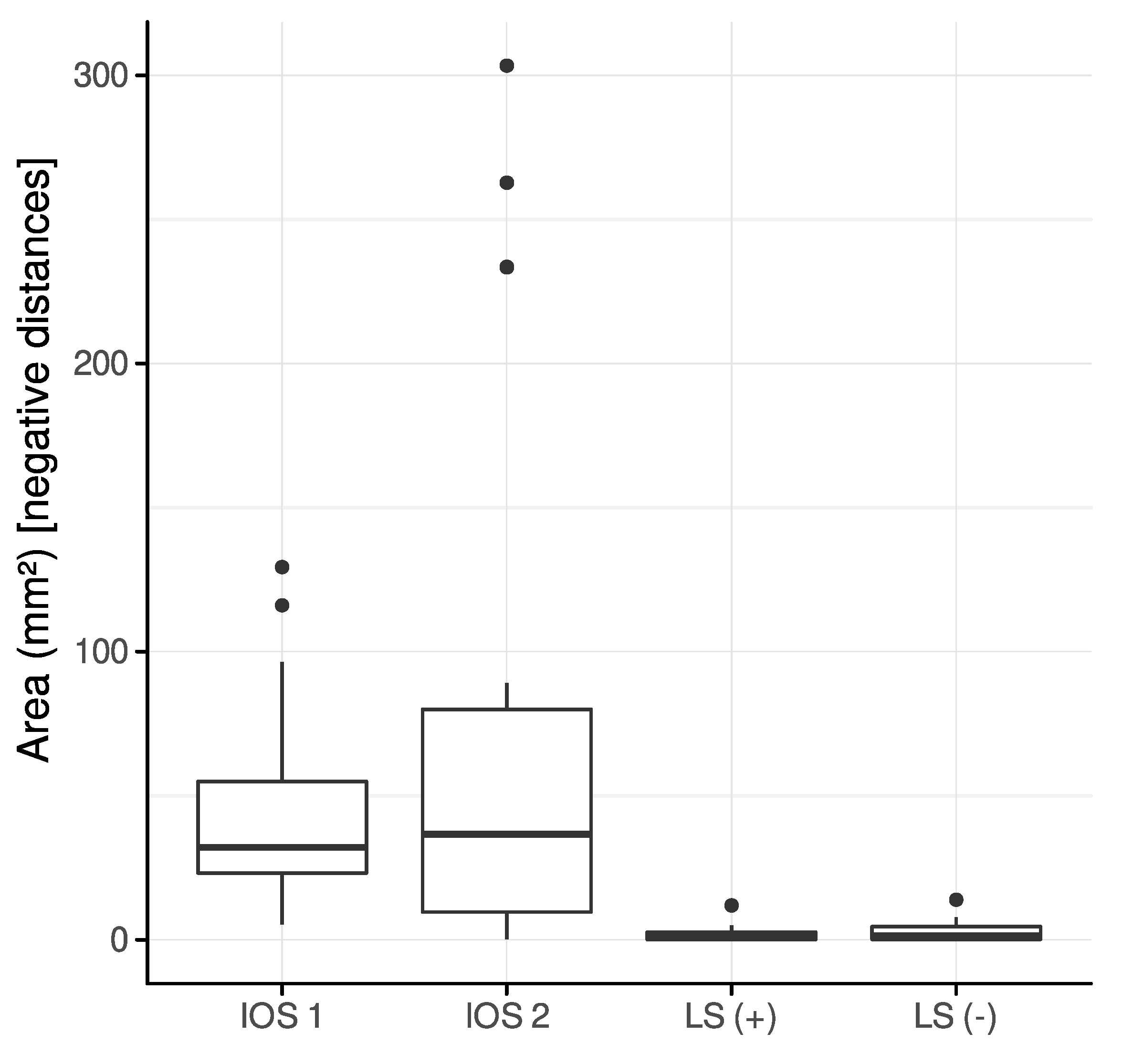
3.2. Intersection
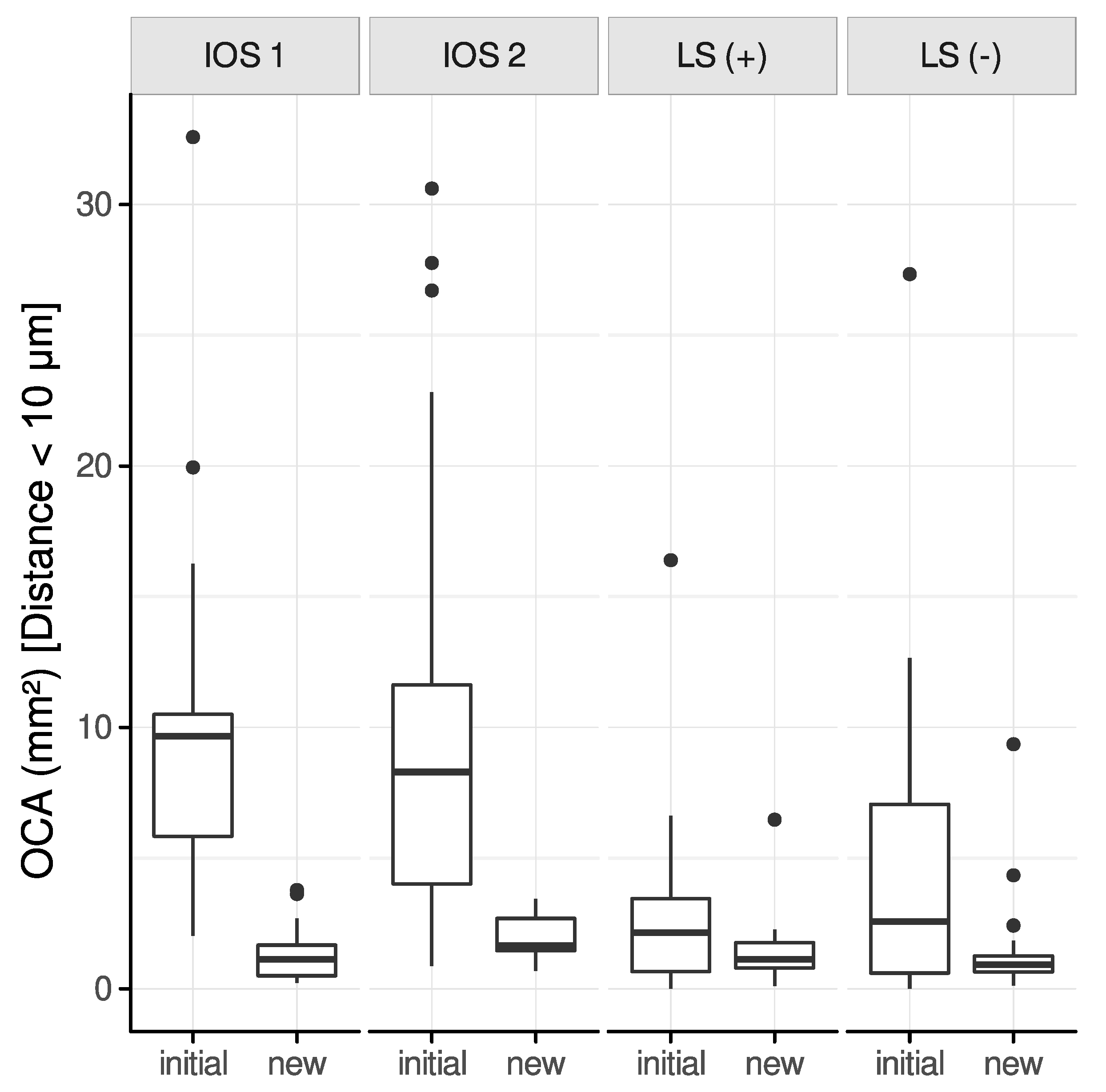
3.3. Difference of the Occlusal Contact Area (OCA) between Initial and New Alignment
3.3.1. Interocclusal Distance Range: 0–100 μm
3.3.2. Interocclusal Distance Range: 0–10 μm
3.4. Rating of Occlusal Contact Points
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waldecker, M.; Bömicke, W.; Behnisch, R.; Rammelsberg, P.; Rues, S. In-Vitro Accuracy of Complete Arch Scans of the Fully Dentate and the Partially Edentulous Maxilla. J. Prosthodont. Res. 2022, 66, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Ferrari, M.; Gallucci, G.O.; Wittneben, J.-G.; Brägger, U. Digital Technology in Fixed Implant Prosthodontics. Periodontol. 2000 2017, 73, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Guo, D.; Zhou, Y.; Jung, R.E.; Hämmerle, C.H.F.; Mühlemann, S. Time Efficiency and Quality of Outcomes in a Model-Free Digital Workflow Using Digital Impression Immediately after Implant Placement: A Double-Blind Self-Controlled Clinical Trial. Clin. Oral. Implants Res. 2019, 30, 617–626. [Google Scholar] [CrossRef]
- Flügge, T.; van der Meer, W.J.; Gonzalez, B.G.; Vach, K.; Wismeijer, D.; Wang, P. The Accuracy of Different Dental Impression Techniques for Implant-Supported Dental Prostheses: A Systematic Review and Meta-Analysis. Clin. Oral. Implants Res. 2018, 29, 374–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Vazouras, K.; Chen, Y.; Kotina, E.; Natto, Z.; Kang, K.; Chochlidakis, K. Digital vs Conventional Implant Impressions: A Systematic Review and Meta-Analysis. J. Prosthodont. 2020, 29, 660–678. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-J.; Shi, J.-Y.; Qian, S.-J.; Qiao, S.-C.; Lai, H.-C. Accuracy of Full-Arch Digital Implant Impressions Taken Using Intraoral Scanners and Related Variables: A Systematic Review. Int. J. Oral Implantol. Berl. Ger. 2021, 14, 157–179. [Google Scholar]
- Sanda, M.; Miyoshi, K.; Baba, K. Trueness and Precision of Digital Implant Impressions by Intraoral Scanners: A Literature Review. Int. J. Implant Dent. 2021, 7, 97. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The Complete Digital Workflow in Fixed Prosthodontics: A Systematic Review. BMC Oral. Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Arcuri, L.; Lio, F.; Campana, V.; Mazzetti, V.; Federici, F.R.; Nardi, A.; Galli, M. Influence of Implant Scanbody Wear on the Accuracy of Digital Impression for Complete-Arch: A Randomized In Vitro Trial. Materials 2022, 15, 927. [Google Scholar] [CrossRef]
- Morsy, N.; El Kateb, M. In Vivo Precision of Digital Static Interocclusal Registration for Full Arch and Quadrant Arch Scans: A Randomized Controlled Clinical Trial. BMC Oral. Health 2022, 22, 559. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gómez-Polo, M.; Zeitler, J.M.; Barmak, A.B.; Kois, J.C.; Pérez-Barquero, J.A. Does the Available Interocclusal Space Influence the Accuracy of the Maxillomandibular Relationship Captured with an Intraoral Scanner? J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Botsford, K.P.; Frazier, M.C.; Ghoneima, A.A.M.; Utreja, A.; Bhamidipalli, S.S.; Stewart, K.T. Precision of the Virtual Occlusal Record. Angle Orthod. 2019, 89, 751–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solaberrieta, E.; Garmendia, A.; Brizuela, A.; Otegi, J.R.; Pradies, G.; Szentpétery, A. Intraoral Digital Impressions for Virtual Occlusal Records: Section Quantity and Dimensions. BioMed Res. Int. 2016, 2016, e7173824. [Google Scholar] [CrossRef] [Green Version]
- Solaberrieta, E.; Otegi, J.R.; Goicoechea, N.; Brizuela, A.; Pradies, G. Comparison of a Conventional and Virtual Occlusal Record. J. Prosthet. Dent. 2015, 114, 92–97. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gohil, A.; Barmak, A.B.; Zandinejad, A.; Raigrodski, A.J.; Alonso Pérez-Barquero, J. Best-Fit Algorithm Influences on Virtual Casts’ Alignment Discrepancies. J. Prosthodont. 2022, jopr.13537. [Google Scholar] [CrossRef]
- Vág, J.; Nagy, Z.; Simon, B.; Mikolicz, Á.; Kövér, E.; Mennito, A.; Evans, Z.; Renne, W. A Novel Method for Complex Three-Dimensional Evaluation of Intraoral Scanner Accuracy. Int. J. Comput. Dent. 2019, 22, 239–249. [Google Scholar]
- Nagy, Z.; Simon, B.; Mennito, A.; Evans, Z.; Renne, W.; Vág, J. Comparing the Trueness of Seven Intraoral Scanners and a Physical Impression on Dentate Human Maxilla by a Novel Method. BMC Oral. Health 2020, 20, 97. [Google Scholar] [CrossRef] [Green Version]
- Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. The Accuracy of Virtual Interocclusal Registration during Intraoral Scanning. J. Prosthet. Dent. 2018, 120, 904–912. [Google Scholar] [CrossRef]
- Revilla-León, M.; Alonso Pérez-Barquero, J.; Zubizarreta-Macho, Á.; Barmak, A.B.; Att, W.; Kois, J.C. Influence of the Number of Teeth and Location of the Virtual Occlusal Record on the Accuracy of the Maxillo-Mandibular Relationship Obtained by Using An Intraoral Scanner. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2022. [Google Scholar] [CrossRef]
- Schneider, P.J.; Eberly, D.H. Intersection in 3D. In Geometric Tools for Computer Graphics; Schneider, P.J., Eberly, D.H., Eds.; The Morgan Kaufmann Series in Computer Graphics; Morgan Kaufmann: San Francisco, CA, USA, 2003; pp. 481–662. ISBN 978-1-55860-594-7. [Google Scholar]
- Jones, M.W.; Baerentzen, J.A.; Sramek, M. 3D Distance Fields: A Survey of Techniques and Applications. IEEE Trans. Vis. Comput. Graph. 2006, 12, 581–599. [Google Scholar] [CrossRef] [PubMed]
- Abdulateef, S.; Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. Clinical Accuracy and Reproducibility of Virtual Interocclusal Records. J. Prosthet. Dent. 2020, 124, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of Complete- and Partial-Arch Impressions of Actual Intraoral Scanning Systems in Vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar]
- Braian, M.; Wennerberg, A. Trueness and Precision of 5 Intraoral Scanners for Scanning Edentulous and Dentate Complete-Arch Mandibular Casts: A Comparative In Vitro Study. J. Prosthet. Dent. 2019, 122, 129–136.e2. [Google Scholar] [CrossRef] [Green Version]
- Ebeid, K.; Nouh, I.; Ashraf, Y.; Cesar, P.F. Accuracy of Different Laboratory Scanners for Scanning of Implant-Supported Full Arch Fixed Prosthesis. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2022, 34, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Dupagne, L.; Tapie, L.; Lebon, N.; Mawussi, B. Comparison of the Acquisition Accuracy and Digitizing Noise of 9 Intraoral and Extraoral Scanners: An Objective Method. J. Prosthet. Dent. 2021, 128, 1032–1040. [Google Scholar] [CrossRef]
- Brawek, P.K.; Wolfart, S.; Endres, L.; Kirsten, A.; Reich, S. The Clinical Accuracy of Single Crowns Exclusively Fabricated by Digital Workflow--the Comparison of Two Systems. Clin. Oral. Investig. 2013, 17, 2119–2125. [Google Scholar] [CrossRef]
- Wong, K.Y.; Esguerra, R.J.; Chia, V.A.P.; Tan, Y.H.; Tan, K.B.C. Three-Dimensional Accuracy of Digital Static Interocclusal Registration by Three Intraoral Scanner Systems: Digital Static Interocclusal Registration 3D Accuracy. J. Prosthodont. 2018, 27, 120–128. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing (Version 3.6.1). R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- DeLong, R.; Ko, C.-C.; Anderson, G.C.; Hodges, J.S.; Douglas, W.H. Comparing Maximum Intercuspal Contacts of Virtual Dental Patients and Mounted Dental Casts. J. Prosthet. Dent. 2002, 88, 622–630. [Google Scholar] [CrossRef]
- Schlager, S. Morpho and Rvcg–Shape Analysis in R: R-Packages for Geometric Morphometrics, Shape Analysis and Surface Manipulations. In Statistical Shape and Deformation Analysis; Academic Press: London, UK, 2017; pp. 217–256. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital Implant Impressions in Clinical Studies: A Systematic Review. Clin. Oral. Implants Res. 2022, 33, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Stavness, I.K.; Hannam, A.G.; Tobias, D.L.; Zhang, X. Simulation of Dental Collisions and Occlusal Dynamics in the Virtual Environment. J. Oral. Rehabil. 2016, 43, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ko, K.; Huh, Y.; Cho, L.; Park, C. Correlation between Occlusal Contact Area at Various Levels of Interocclusal Thicknesses and Masticatory Performance. J. Oral. Rehabil. 2021, joor.13292. [Google Scholar] [CrossRef] [PubMed]
- Straga, R.W. Comparison of Occlusal Contacts on Mounted Dental Models to Contacts Identified on Digital 3D Models Using a New Virtual Alignment Method. Master’s Thesis, University of British Columbia, Vancouver, BC, Canada, 2009. [Google Scholar]
- Patzelt, S.B.M.; Emmanouilidi, A.; Stampf, S.; Strub, J.R.; Att, W. Accuracy of Full-Arch Scans Using Intraoral Scanners. Clin. Oral. Investig. 2014, 18, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Fraile, C.; Ferreiroa, A.; Romeo, M.; Alonso, R.; Pradíes, G. Clinical Study Comparing the Accuracy of Interocclusal Records, Digitally Obtained by Three Different Devices. Clin. Oral. Investig. 2022, 26, 1957–1962. [Google Scholar] [CrossRef]
- Tappert, M.V.; Grabowski, H.; Dammaschke, T. Accuracy and Reproducibility of the Visualisation of Occlusal Contact Points Using Analogue Articulating Foil or Digital Intraoral Scanners in Vitro. Int. J. Comput. Dent. 2022. [Google Scholar] [CrossRef]
- DeLong, R.; Knorr, S.; Anderson, G.C.; Hodges, J.; Pintado, M.R. Accuracy of Contacts Calculated from 3D Images of Occlusal Surfaces. J. Dent. 2007, 35, 528–534. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beck, F.; Lettner, S.; Zupancic Cepic, L.; Schedle, A. Comparison of Virtual Intersection and Occlusal Contacts between Intraoral and Laboratory Scans: An In-Vivo Study. J. Clin. Med. 2023, 12, 996. https://doi.org/10.3390/jcm12030996
Beck F, Lettner S, Zupancic Cepic L, Schedle A. Comparison of Virtual Intersection and Occlusal Contacts between Intraoral and Laboratory Scans: An In-Vivo Study. Journal of Clinical Medicine. 2023; 12(3):996. https://doi.org/10.3390/jcm12030996
Chicago/Turabian StyleBeck, Florian, Stefan Lettner, Lana Zupancic Cepic, and Andreas Schedle. 2023. "Comparison of Virtual Intersection and Occlusal Contacts between Intraoral and Laboratory Scans: An In-Vivo Study" Journal of Clinical Medicine 12, no. 3: 996. https://doi.org/10.3390/jcm12030996