
The Impact and Treatment of COVID-19 in Hemodialysis Patients

Abstract
:1. Introduction
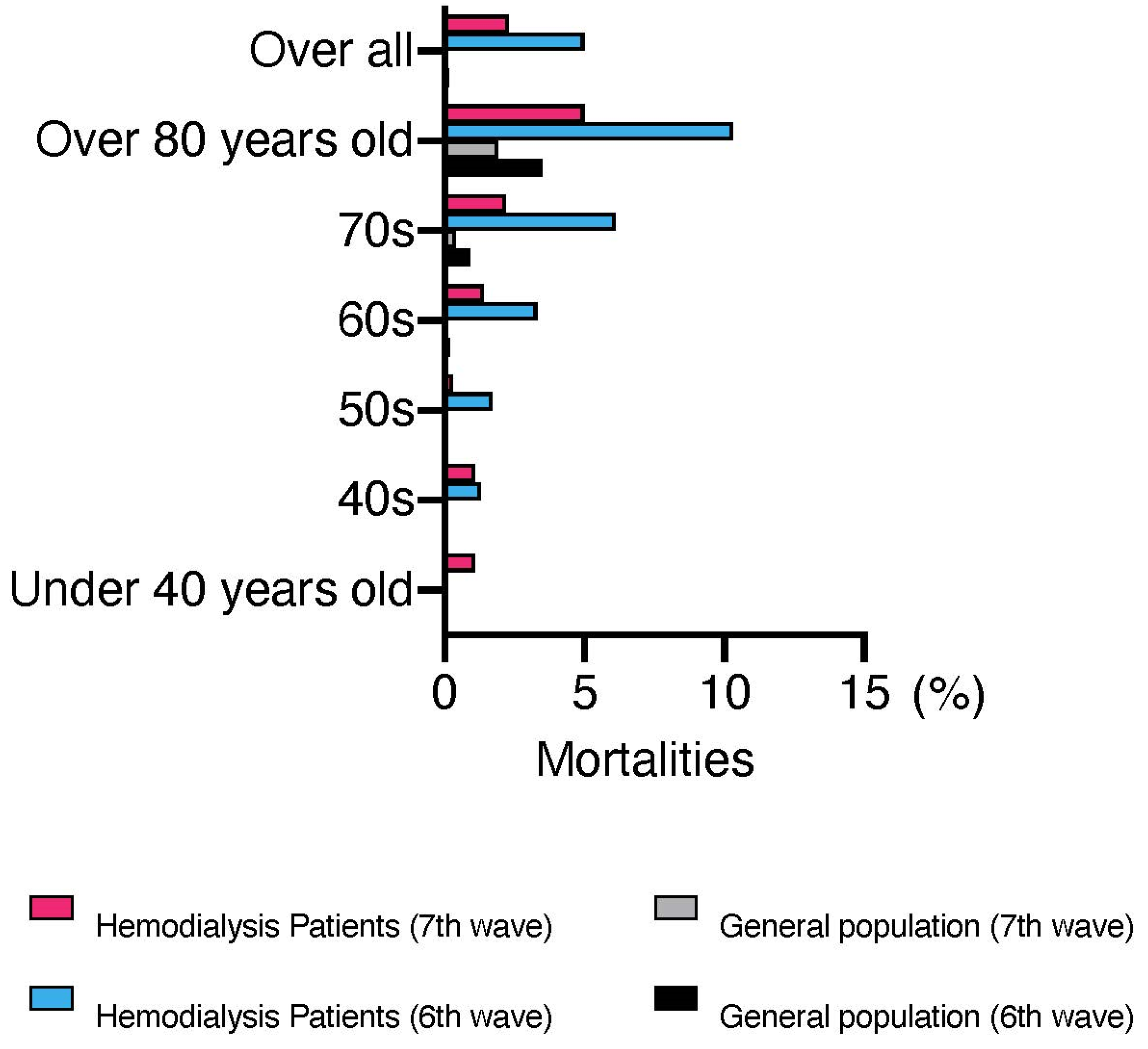
2. Number and Severity of Patients with COVID-19 Undergoing Dialysis in Japan
3. Efficacy of COVID-19 Vaccination in Patients with End-Stage Renal Disease
4. Infection Control and Hospitalization of Patients Undergoing Dialysis in Japan
5. Current Treatment of COVID-19 in Patients Undergoing Dialysis
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M.; et al. Clinical Epidemiology of Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) in Japan: Report of the COVID-19 Registry Japan. Clin. Infect. Dis. 2021, 73, e3677–e3689. [Google Scholar] [CrossRef]
- Katagiri, D.; Ishikane, M.; Asai, Y.; Kinoshita, N.; Ota, M.; Moriyama, Y.; Ide, S.; Nakamura, K.; Nakamoto, T.; Nomoto, H.; et al. Evaluation of Coronavirus Disease 2019 Severity Using Urine Biomarkers. Crit. Care Explor. 2020, 2, e0170. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. Negative Impact of the COVID-19 Pandemic on Kidney Disease Management-A Single-Center Experience in Romania. J. Clin. Med. 2022, 11, 2452. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, D. For safe and adequate blood purification therapy in severe COVID-19—What we have learned so far. Glob. Health Med. 2022, 4, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, D.; Ishikane, M.; Asai, Y.; Izumi, S.; Takasaki, J.; Katsuoka, H.; Kondo, I.; Ide, S.; Nakamura, K.; Nakamoto, T.; et al. Direct hemoperfusion using a polymyxin B-immobilized polystyrene column for COVID-19. J. Clin. Apher. 2021, 36, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Nangaku, M.; Ryuzaki, M.; Yamakawa, T.; Hanafusa, N.; Sakai, K.; Kanno, Y.; Ando, R.; Shinoda, T.; Nakamoto, H.; et al. COVID-19 of dialysis patients in Japan: Current status and guidance on preventive measures. Ther. Apher. Dial. 2020, 24, 361–365. [Google Scholar] [CrossRef]
- Ashby, D.R.; Caplin, B.; Corbett, R.W.; Asgari, E.; Kumar, N.; Sarnowski, A.; Hull, R.; Makanjuola, D.; Cole, N.; Chen, J.; et al. Severity of COVID-19 after Vaccination among Hemodialysis Patients: An Observational Cohort Study. Clin. J. Am. Soc. Nephrol. CJASN 2022, 17, 843–850. [Google Scholar] [CrossRef]
- Brunelli, S.M.; Sibbel, S.; Karpinski, S.; Marlowe, G.; Walker, A.G.; Giullian, J.; Van Wyck, D.; Kelley, T.; Lazar, R.; Zywno, M.L.; et al. Comparative Effectiveness of mRNA-based BNT162b2 Vaccine versus Adenovirus Vector-Based Ad26.COV2.S Vaccine for the Prevention of COVID-19 among Dialysis Patients. J. Am. Soc. Nephrol. 2022, 33, 688–697. [Google Scholar] [CrossRef]
- Frittoli, M.; Cassia, M.; Barassi, A.; Ciceri, P.; Galassi, A.; Conte, F.; Cozzolino, M.G. Efficacy and Safety of COVID-19 Vaccine in Patients on Renal Replacement Therapy. Vaccines 2022, 10, 1395. [Google Scholar] [CrossRef]
- Babel, N.; Hugo, C.; Westhoff, T.H. Vaccination in patients with kidney failure: Lessons from COVID-19. Nat. Rev. Nephrol. 2022, 18, 708–723. [Google Scholar] [CrossRef]
- Blake, P.G.; Hladunewich, M.A.; Oliver, M.J. COVID-19 Vaccination Imperatives in People on Maintenance Dialysis: An International Perspective. Clin. J. Am. Soc. Nephrol. 2021, 16, 1746–1748. [Google Scholar] [CrossRef] [PubMed]
- Moreno, N.F.; McAdams, R.; Goss, J.A.; Galvan, N.T.N. COVID-19 Vaccine Efficacy and Immunogenicity in End-Stage Renal Disease Patients and Kidney Transplant Recipients. Curr. Transplant. Rep. 2022, 9, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Nangaku, M.; Ryuzaki, M.; Yamakawa, T.; Yoshihiro, O.; Hanafusa, N.; Sakai, K.; Kanno, Y.; Ando, R.; Shinoda, T.; et al. Effectiveness of SARS-CoV-2 vaccines on hemodialysis patients in Japan: A nationwide cohort study. Ther. Apher. Dial. 2022, 27, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Mahalingasivam, V.; Su, G.; Iwagami, M.; Davids, M.R.; Wetmore, J.B.; Nitsch, D. COVID-19 and kidney disease: Insights from epidemiology to inform clinical practice. Nat. Rev. Nephrol. 2022, 18, 485–498. [Google Scholar] [CrossRef]
- Perl, J.; Thomas, D.; Tang, Y.; Yeung, A.; Ip, J.; Oliver, M.J.; Blake, P.G. COVID-19 among Adults Receiving Home versus In-Center Dialysis. Clin. J. Am. Soc. Nephrol. CJASN 2021, 16, 1410–1412. [Google Scholar] [CrossRef]
- Kikuchi, K.; Nangaku, M.; Ryuzaki, M.; Yamakawa, T.; Yoshihiro, O.; Hanafusa, N.; Sakai, K.; Kanno, Y.; Ando, R.; Shinoda, T.; et al. Survival and predictive factors in dialysis patients with COVID-19 in Japan: A nationwide cohort study. Ren. Replace. Ther. 2021, 7, 59. [Google Scholar] [CrossRef]
- The Japanese Associations of Dialysis Physicians. Guidelines for Standard Hemodialysis Procedure and Prevention of Infection in Maintenance Hemodialysis Facilities, 5th ed.; The Japanese Associations of Dialysis Physicians: Tokyo, Japan, 2020. [Google Scholar]
- Sugawara, Y.; Iwagami, M.; Kikuchi, K.; Yoshida, Y.; Ando, R.; Shinoda, T.; Ryuzaki, M.; Nakamoto, H.; Sakai, K.; Hanafusa, N.; et al. Infection prevention measures for patients undergoing hemodialysis during the COVID-19 pandemic in Japan: A nationwide questionnaire survey. Ren. Replace. Ther. 2021, 7, 27. [Google Scholar] [CrossRef]
- Behlul, S.; Artac Ozdal, M. Risk of COVID-19 and Cost Burden in End-Stage Renal Disease Patients and Policy Implications for Managing Nephrology Services during the COVID-19 Pandemic. Healthcare 2022, 10, 2351. [Google Scholar] [CrossRef]
- Naito, K.; Kikuchi, K.; Watanabe, Y.; Narita, T. Implementation of two novel schemes for patients on dialysis as a response to the COVID-19 surge in Tokyo. Glob. Health Med. 2022, 4, 253–258. [Google Scholar] [CrossRef]
- Zaki, K.E.; Huang, C.W.; Zhou, H.; Chung, J.; Selevan, D.C.; Rutkowski, M.P.; Sim, J.J. Comparison of safety and outcomes related to remdesivir treatment among dialysis patients hospitalized with COVID-19. Clin. Kidney J. 2022, 15, 2056–2062. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Poznański, P.; Augustyniak-Bartosik, H.; Magiera-Żak, A.; Skalec, K.; Jakuszko, K.; Mazanowska, O.; Janczak, D.; Krajewska, M.; Kamińska, D. Molnupiravir When Used Alone Seems to Be Safe and Effective as Outpatient COVID-19 Therapy for Hemodialyzed Patients and Kidney Transplant Recipients. Viruses 2022, 14, 2224. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Yamayoshi, S.; Simon, V.; van Bakel, H.; Sordillo, E.M.; Pekosz, A.; Fukushi, S.; Suzuki, T.; Maeda, K.; Halfmann, P.; et al. Efficacy of Antibodies and Antiviral Drugs against Omicron BA.2.12.1, BA.4, and BA.5 Subvariants. N. Engl. J. Med. 2022, 387, 468–470. [Google Scholar] [CrossRef]
- Terakawa, K.; Katagiri, D.; Shimada, K.; Sato, L.; Takano, H. Safety of casirivimab/imdevimab administration in a SARS-CoV-2 positive maintenance dialysis patient in Japan. CEN Case Rep. 2022, 11, 328–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type | Antiviral Drug | Immunity Suppressants/Regulators | Neutralizing Antibody | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Name | Remdesivir | Molnupiravir | Nirmatrelvir/ Ritonavir | Ensitrelvir | Dexamethasone | Baricitinib | Tocilizumab | Sotrovimab | Casirivimab–imdevimab |
| Severity to be administered | Mild, Moderate Severe | Mild, Moderate | Mild, Moderate | Mild, Moderate | Moderate, Severe | Moderate, Severe | Moderate, Severe | Mild | Mild |
| Response to Omicron | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | No |
| Route of administration | Intravenous | Oral | Oral | Oral | Intravenous, oral | Oral | Intravenous | Intravenous | Intravenous |
| Length of treatment | 3–10 days | 5 days | 5 days | 5 days | 10 days | 14 days | Single dose | Single dose | Single dose |
| Dosage in dialysis patients | 100 mg 4 h before dialysis initiation. Approximately 6 doses | No adjustment required | No administration to dialysis patients | No clinical trials have been conducted in patients with renal dysfunction | No adjustment required | No administration to dialysis patients | No adjustment required | No adjustment required | No adjustment required |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katagiri, D.; Kikuchi, K. The Impact and Treatment of COVID-19 in Hemodialysis Patients. J. Clin. Med. 2023, 12, 838. https://doi.org/10.3390/jcm12030838
Katagiri D, Kikuchi K. The Impact and Treatment of COVID-19 in Hemodialysis Patients. Journal of Clinical Medicine. 2023; 12(3):838. https://doi.org/10.3390/jcm12030838
Chicago/Turabian StyleKatagiri, Daisuke, and Kan Kikuchi. 2023. "The Impact and Treatment of COVID-19 in Hemodialysis Patients" Journal of Clinical Medicine 12, no. 3: 838. https://doi.org/10.3390/jcm12030838