

Validation of Noninvasive Assessment of Pulmonary Gas Exchange in Patients with Chronic Obstructive Pulmonary Disease during Initial Exposure to High Altitude
 , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Experimental Protocol
- -
- Non-invasive AGM100 measurement was first performed: participants were asked to breathe through a mouthpiece (with a nose clip) to record PETO2 and PETCO2, while SpO2 was continuously measured with a finger pulse oximeter, connected to the device. After automatic detection of a breathing steady-state, the measurement was automatically stopped and values for SpO2, PETO2, and PETCO2 were recorded, and the cPaO2 and O2 deficit were calculated [10,11].
- -
- Immediately after the AGM100 measurement, an arterial blood sample was collected by radial artery puncture while participants were breathing ambient air. Each sample was analyzed using a point-of-care blood gas analyzer (EPOC®, Siemens Healthcare, Erlangen, Germany). PaO2, PaCO2, and arterial pH were analyzed. The EPOC has been previously validated in a high-altitude environment [20].
2.3. Clinical Assessment
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Measurements and Patients Included in the Study
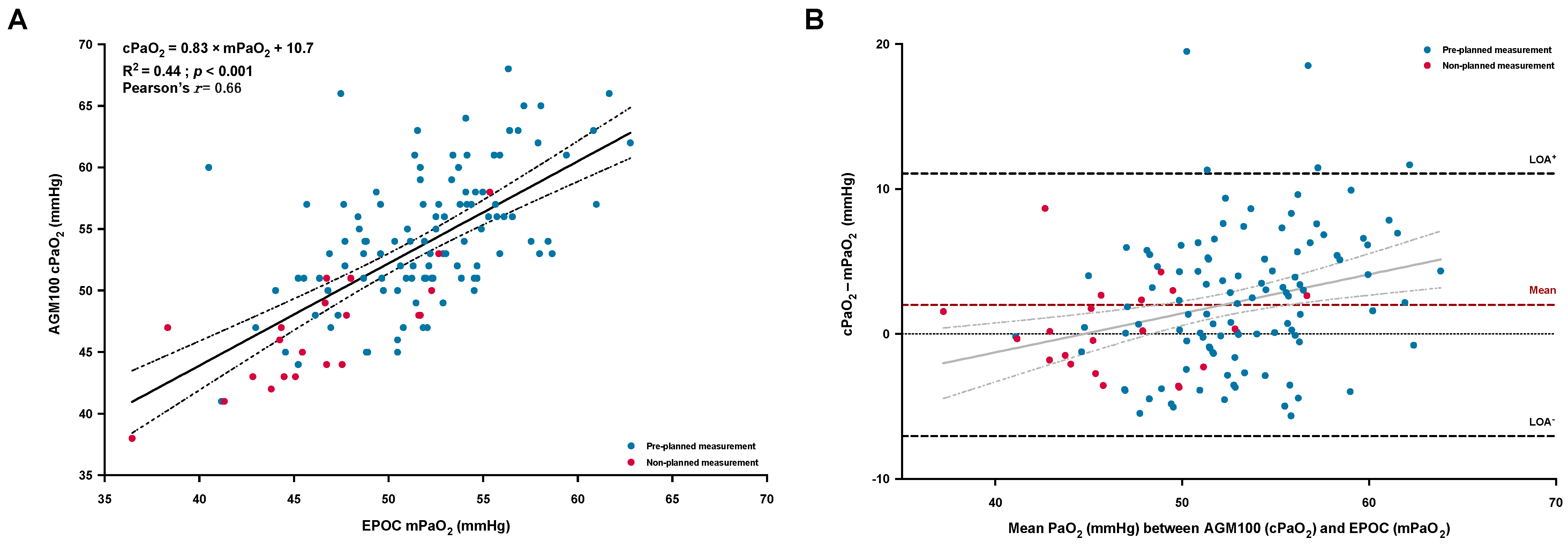
3.2. PaO2 Agreement between cPaO2 (AGM100) and mPaO2 (EPOC)
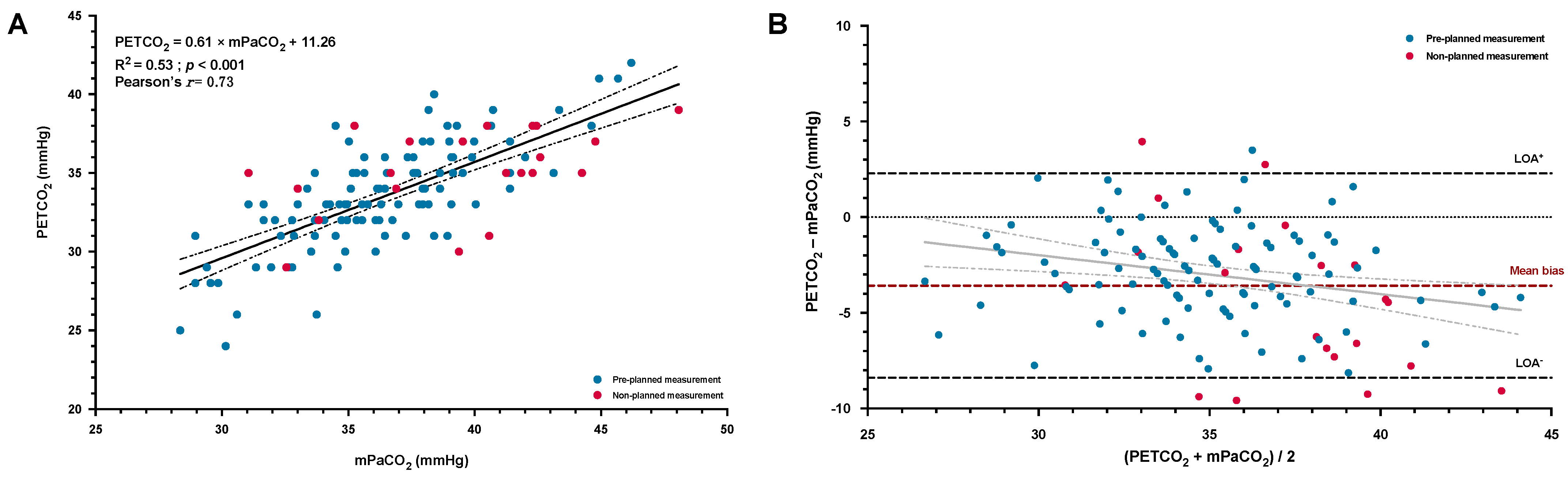
3.3. Agreement between PETCO2 (AGM100) and PaCO2 (EPOC)
3.4. Factors Associated with the Accuracy of the cPaO2 and Diagnosis Performance
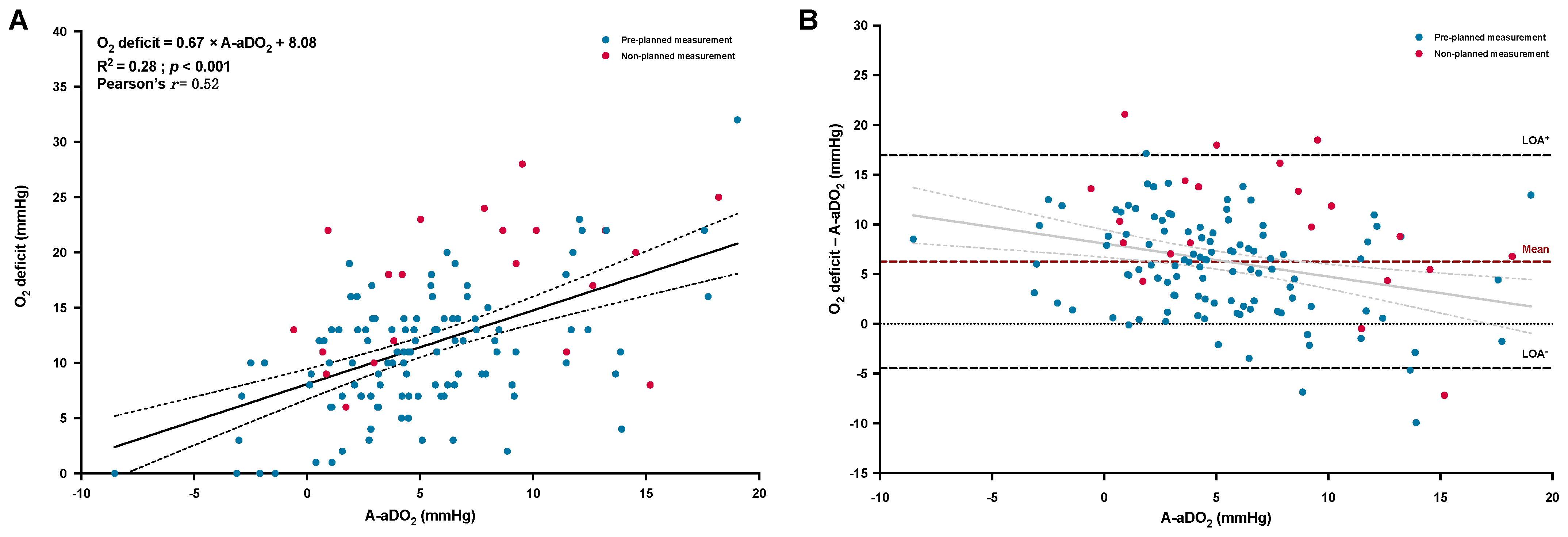
3.5. Agreement between O2 Deficit and A-aDO2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagner, P.D. The physiological basis of pulmonary gas exchange: Implications for clinical interpretation of arterial blood gases. Eur. Respir. J. 2015, 45, 227–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.L.; Cournand, A. ‘Ideal’ Alveolar Air and the Analysis of Ventilation-Perfusion Relationships in the Lungs. J. Appl. Physiol. 1949, 1, 825–847. [Google Scholar] [CrossRef] [PubMed]
- Petersson, J.; Glenny, R.W. Gas exchange and ventilation-perfusion relationships in the lung. Eur. Respir. J. 2014, 44, 1023–1041. [Google Scholar] [CrossRef] [Green Version]
- Uemasu, K.; Sato, S.; Muro, S.; Sato, A.; Tanabe, N.; Hasegawa, K.; Hamakawa, Y.; Mizutani, T.; Fuseya, Y.; Tanimura, K.; et al. Annual decline in arterial blood oxygen predicts development of chronic respiratory failure in COPD with mild hypoxaemia: A 6-year follow-up study. Respirology 2019, 24, 262–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agusti, A.; Faner, R. Lung function trajectories in health and disease. Lancet Respir. Med. 2019, 7, 358–364. [Google Scholar] [CrossRef]
- Hardinge, M.; Annandale, J.; Bourne, S.; Cooper, B.; Evans, A.; Freeman, D.; Green, A.; Hippolyte, S.; Knowles, V.; MacNee, W.; et al. British Thoracic Society guidelines for home oxygen use in adults. Thorax 2015, 70 (Suppl. S1), i1–i43. [Google Scholar] [CrossRef] [Green Version]
- Giner, J.; Casan, P.; Belda, J.; González, M.; Miralda, R.M.; Sanchis, J. Pain During Arterial Puncture. Chest 1996, 110, 1443–1445. [Google Scholar] [CrossRef]
- Pickerodt, P.A.; Kuebler, W.M. Go West: Translational physiology for noninvasive measurement of pulmonary gas exchange in patients with hypoxemic lung disease. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2019, 316, L701–L702. [Google Scholar] [CrossRef]
- West, J.B.; Prisk, G.K. A new method for noninvasive measurement of pulmonary gas exchange using expired gas. Resp. Physiol. Neurobiol. 2018, 247, 112–115. [Google Scholar] [CrossRef]
- Prisk, G.K.; West, J.B. Deriving the arterial Po2 and oxygen deficit from expired gas and pulse oximetry. J. Appl. Physiol. 2019, 127, 1067–1074. [Google Scholar] [CrossRef]
- Prisk, G.K.; West, J.B. Non-invasive Measurement of Pulmonary Gas Exchange Efficiency: The Oxygen Deficit. Front. Physiol. 2021, 12, 757857. [Google Scholar] [CrossRef]
- West, J.B.; Wang, D.L.; Prisk, G.K.; Fine, J.M.; Bellinghausen, A.; Light, M.; Crouch, D.R. Noninvasive measurement of pulmonary gas exchange: Comparison with data from arterial blood gases. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2019, 316, L114–L118. [Google Scholar] [CrossRef]
- Howe, C.A.; MacLeod, D.B.; Wainman, L.; Oliver, S.J.; Ainslie, P.N. Validation of a Noninvasive Assessment of Pulmonary Gas Exchange During Exercise in Hypoxia. Chest 2020, 158, 1644–1650. [Google Scholar] [CrossRef]
- West, J.B.; Crouch, D.R.; Fine, J.M.; Makadia, D.; Wang, D.L.; Prisk, G.K. A New, Noninvasive Method of Measuring Impaired Pulmonary Gas Exchange in Lung Disease: An Outpatient Study. Chest 2018, 154, 363–369. [Google Scholar] [CrossRef]
- West, J.B.; Wang, D.L.; Prisk, G.K. Measurements of pulmonary gas exchange efficiency using expired gas and oximetry: Results in normal subjects. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2018, 314, L686–L689. [Google Scholar] [CrossRef]
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease(2022 Report). Available online: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf (accessed on 16 January 2023).
- Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 16 January 2023).
- Kent, B.D.; Mitchell, P.D.; McNicholas, W.T. Hypoxemia in patients with COPD: Cause, effects, and disease progression. Int. J. Chronic. Obs. Pulmon. Dis. 2011, 6, 199–208. [Google Scholar]
- Furian, M.; Mademilov, M.; Buergin, A.; Scheiwiller, P.M.; Mayer, L.; Schneider, S.; Emilov, B.; Lichtblau, M.; Bitos, K.; Muralt, L.; et al. Acetazolamide to Prevent Adverse Altitude Effects in COPD and Healthy Adults. Nejm. Évid. 2022, 1. [Google Scholar] [CrossRef]
- Nawrocki, J.; Furian, M.; Buergin, A.; Mayer, L.; Schneider, S.R.; Mademilov, M.; Bloch, M.; Sooronbaev, T.M.; Ulrich, S.; Bloch, K.E. Validation of a Portable Blood Gas Analyzer for Use in Challenging Field Conditions at High Altitude. Front. Physiol. 2021, 11, 600551. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Resp. Crit. Care 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Montenij, L.J.; Buhre, W.F.; Jansen, J.R.; Kruitwagen, C.L.; EE de, W. Methodology of method comparison studies evaluating the validity of cardiac output monitors: A stepwise approach and checklist. Bja. Br. J. Anaesth. 2016, 116, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcguire, W.C.; Crouch, D.R.; Pearce, A.; West, J.B.; Prisk, G.K.; Elliott, A.R.; Fine, J.M.; Malhotra, A. The Use of the Alveolar Gas Meter for Assessment of Gas Exchange Abnormalities in COVID-19. Am. J. Respir. Crit. Care. Med. 2021, 203, A4454. [Google Scholar]
- Amaza, I.; Kalra, H.; Eberlein, M.; Jethava, Y.; McDonell, J.; Wolfe, B.; Tomasson, M.H.; Bates, M.L. Case Studies in Physiology: Untangling the cause of hypoxemia in a patient with obesity with acute leukemia. J. Appl. Physiol. 2021, 131, 788–793. [Google Scholar] [CrossRef] [PubMed]
- West, J.B.; Liu, M.A.; Stark, P.C.; Prisk, G.K. Measuring the efficiency of pulmonary gas exchange using expired gas instead of arterial blood: Comparing the “ideal” Po2 of Riley with end-tidal Po2. Am. J. Physiol. Lung Cell. Mol. Physiol. 2020, 319, L289–L293. [Google Scholar] [CrossRef]
- Cao, M.; Stringer, W.W.; Corey, S.; Orogian, A.; Cao, R.; Calmelat, R.; Lin, F.; Casaburi, R.; Rossiter, H.B.; Porszasz, J. Transcutaneous PCO2 for Exercise Gas Exchange Efficiency in Chronic Obstructive Pulmonary Disease. Copd. J. Chronic. Obs. Pulm. Dis. 2020, 18, 16–25. [Google Scholar] [CrossRef]
- Furian, M.; Hartmann, S.E.; Latshang, T.D.; Flueck, D.; Murer, C.; Scheiwiller, P.M.; Osmonov, B.; Ulrich, S.; Kohler, M.; Poulin, M.J.; et al. Exercise Performance of Lowlanders with COPD at 2590 m: Data from a Randomized Trial. Respiration 2018, 95, 422–432. [Google Scholar] [CrossRef] [Green Version]
- Neder, J.A.; Kirby, M.; Santyr, G.; Pourafkari, M.; Smyth, R.; Phillips, D.B.; Crinion, S.; de-Torres, J.P.; O’Donnell, D.E. Ventilation/Perfusion Mismatch: A Novel Target for COPD Treatment. Chest 2022, 162, 1030–1047. [Google Scholar] [CrossRef]
- Liu, M.A.; Stark, P.C.; Prisk, G.K.; West, J.B. Oxygen deficit is a sensitive measure of mild gas exchange impairment at inspired O2 between 12.5% and 21%. Am. J. Physiol. Lung Cell. Mol. Physiol. 2020, 319, L91–L94. [Google Scholar] [CrossRef]
- Kuenzel, A.; Marshall, B.; Verges, S.; Anholm, J.D. Positional Changes in Arterial Oxygen Saturation and End-Tidal Carbon Dioxide at High Altitude: Medex 2015. High. Alt. Med. Biol. 2020, 21, 144–151. [Google Scholar] [CrossRef]
- Jamali, H.; Castillo, T.L.; Morgan, C.C.; Coult, J.; Muhammad, J.L.; Osobamiro, O.O.; Parsons, E.C.; Adamson, R. Racial Disparity in Oxygen Saturation Measurements by Pulse Oximetry: Evidence and Implications. Ann. Am. Thorac. Soc. 2022, 19, 1951–1964. [Google Scholar] [CrossRef]
- Lichtblau, M.; Latshang, T.D.; Furian, M.; Müller-Mottet, S.; Küest, S.; Tanner, F.; Grünig, E.; Bloch, K.E.; Ulrich, S. Right and Left Heart Function in Lowlanders with COPD at Altitude: Data from a Randomized Study. Respiration 2019, 97, 125–134. [Google Scholar] [CrossRef]
- Furian, M.; Flueck, D.; Latshang, T.D.; Scheiwiller, P.M.; Segitz, S.D.; Mueller-Mottet, S.; Murer, C.; Steiner, A.; Uirich, S.; Rothe, T.; et al. Exercise performance and symptoms in lowlanders with COPD ascending to moderate altitude: Randomized trial. Int. J. Chron. Obs. Pulmon. Dis. 2018, 13, 3529–3538. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COPD Participants (n = 131) | |
|---|---|
| Sex | |
| Men | 70 (53%) |
| Women | 61 (47%) |
| Age (years) | 60 (53–65) |
| Body mass index (kg·m−2) | 27.9 ± 4.0 |
| Baseline SpO2 (%) at 760 m | 95 ± 2 |
| FEV1 (% predicted value) | 60 ± 10 |
| GOLD grade a | |
| 2 | 112 (85%) |
| 3 | 19 (15%) |
| Smoking status b | |
| Active smoker | 20 (16%) |
| Ex-smoker | 42 (34%) |
| Never smoke | 62 (50%) |
| Smoking, pack-years | 18 (8–40) |
| mMRC dyspnea score | 1 (1–2) |
| CAT score | 5 (3–9) |
| Comorbidities | |
| Hypertension | 20 (15%) |
| Coronary artery disease | 0 (0%) |
| Diabetes | 4 (3%) |
| Others | 13 (10%) |
| Pulmonary medication | |
| Inhaled beta-adrenergics | 25 (19%) |
| Inhaled anticholinergics | 51 (39%) |
| Inhaled corticosteroids | 24 (18%) |
| Compared Variables | Mean Bias ± SD (mmHg) | 95% CI Mean Bias (mmHg) | LOA (mmHg) |
|---|---|---|---|
| cPaO2 vs. mPaO2 | 2.0 ± 4.6 | 1.2 to 2.8 | −7.1 to 11.1 |
| cPaO2 vs. mPaO2 corrected a | −2.3 ± 4.6 | −3.1 to −1.5 | −11.3 to 6.6 |
| O2 deficit vs. A-aDO2 | 6.2 ± 5.5 | 5.3 to 7.2 | −4.5 to 17.0 |
| O2 deficit vs. A-aDO2 corrected a | 10.6 ± 5.5 | 9.6 to 11.5 | −0.2 to 21.4 |
| Dependent Variable: cPaO2-mPaO2, mmHg | Full Model | Final Model | ||||
|---|---|---|---|---|---|---|
| β-Coefficient | SE | p Value | β-Coefficient | SE | p Value | |
| Intercept | −63.56 | 11.29 | <0.001 | −65.67 | 8.86 | <0.001 |
| Age, years | 0.01 | 0.05 | 0.83 | _ | _ | _ |
| Male sex (vs. female) | −0.92 | 0.79 | 0.25 | _ | _ | _ |
| Body mass index, kg/m2 | 0.11 | 0.10 | 0.28 | 0.18 | 0.09 | 0.046 |
| Baseline FEV1 (% predicted value) at 760 m | −2.66 | 3.78 | 0.48 | _ | _ | _ |
| SpO2, % | 0.72 | 0.12 | <0.001 | 0.70 | 0.10 | <0.001 |
| Time delay between end of AGM100 measurement and ABG puncture, sec | −0.001 | 0.002 | 0.54 | _ | _ | _ |
| PaCO2-PETCO2 difference, mmHg | 0.53 | 0.16 | 0.002 | 0.47 | 0.13 | <0.001 |
| Sensitivity | Specificity | PPV | NPV | LR+ | |
|---|---|---|---|---|---|
| PaO2 ≤ 55 mmHg | 0.75 | 0.80 | 0.94 | 0.43 | 3.77 |
| (0.66 to 0.83) | (0.59 to 0.93) | (0.87 to 0.98) | (0.29 to 0.59) | (1.71 to 8.33) | |
| PaO2 < 60 mmHg | 0.86 | 0.80 | 0.99 | 0.18 | 4.29 |
| (0.78 to 0.91) | (0.28 to 0.99) | (0.95 to 1.00) | (0.05 to 0.40) | (0.74 to 24.77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Champigneulle, B.; Reinhard, L.; Mademilov, M.; Marillier, M.; Ulrich, T.; Carta, A.F.; Scheiwiller, P.; Shabykeeva, S.B.; Sheraliev, U.U.; Abdraeva, A.K.; et al. Validation of Noninvasive Assessment of Pulmonary Gas Exchange in Patients with Chronic Obstructive Pulmonary Disease during Initial Exposure to High Altitude. J. Clin. Med. 2023, 12, 795. https://doi.org/10.3390/jcm12030795
Champigneulle B, Reinhard L, Mademilov M, Marillier M, Ulrich T, Carta AF, Scheiwiller P, Shabykeeva SB, Sheraliev UU, Abdraeva AK, et al. Validation of Noninvasive Assessment of Pulmonary Gas Exchange in Patients with Chronic Obstructive Pulmonary Disease during Initial Exposure to High Altitude. Journal of Clinical Medicine. 2023; 12(3):795. https://doi.org/10.3390/jcm12030795
Chicago/Turabian StyleChampigneulle, Benoit, Lukas Reinhard, Maamed Mademilov, Mathieu Marillier, Tanja Ulrich, Arcangelo F. Carta, Philipp Scheiwiller, Saltanat B. Shabykeeva, Ulan U. Sheraliev, Ainura K. Abdraeva, and et al. 2023. "Validation of Noninvasive Assessment of Pulmonary Gas Exchange in Patients with Chronic Obstructive Pulmonary Disease during Initial Exposure to High Altitude" Journal of Clinical Medicine 12, no. 3: 795. https://doi.org/10.3390/jcm12030795