
Hemodynamic and Respiratory Changes following Prone Position in Acute Respiratory Distress Syndrome Patients: A Clinical Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Outcomes
2.3. Settings
2.4. Statistical Analysis
3. Results
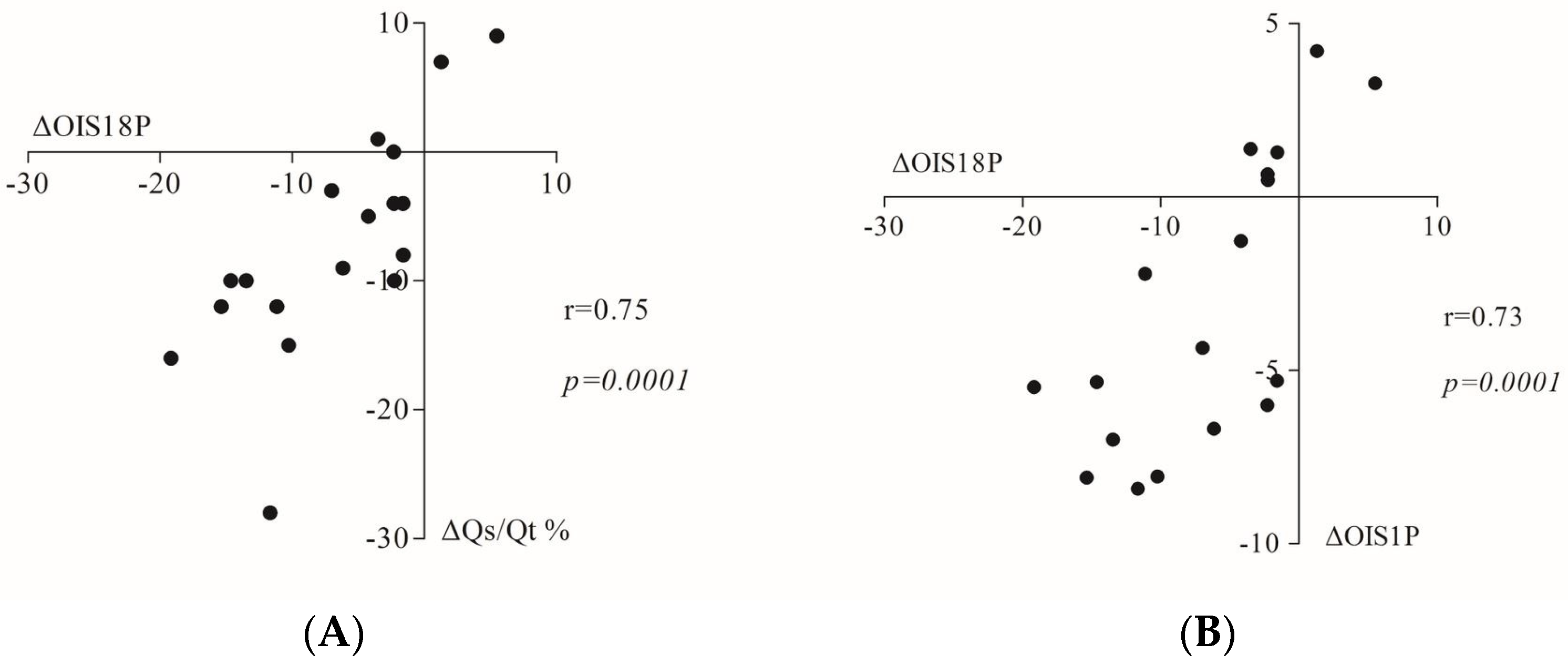
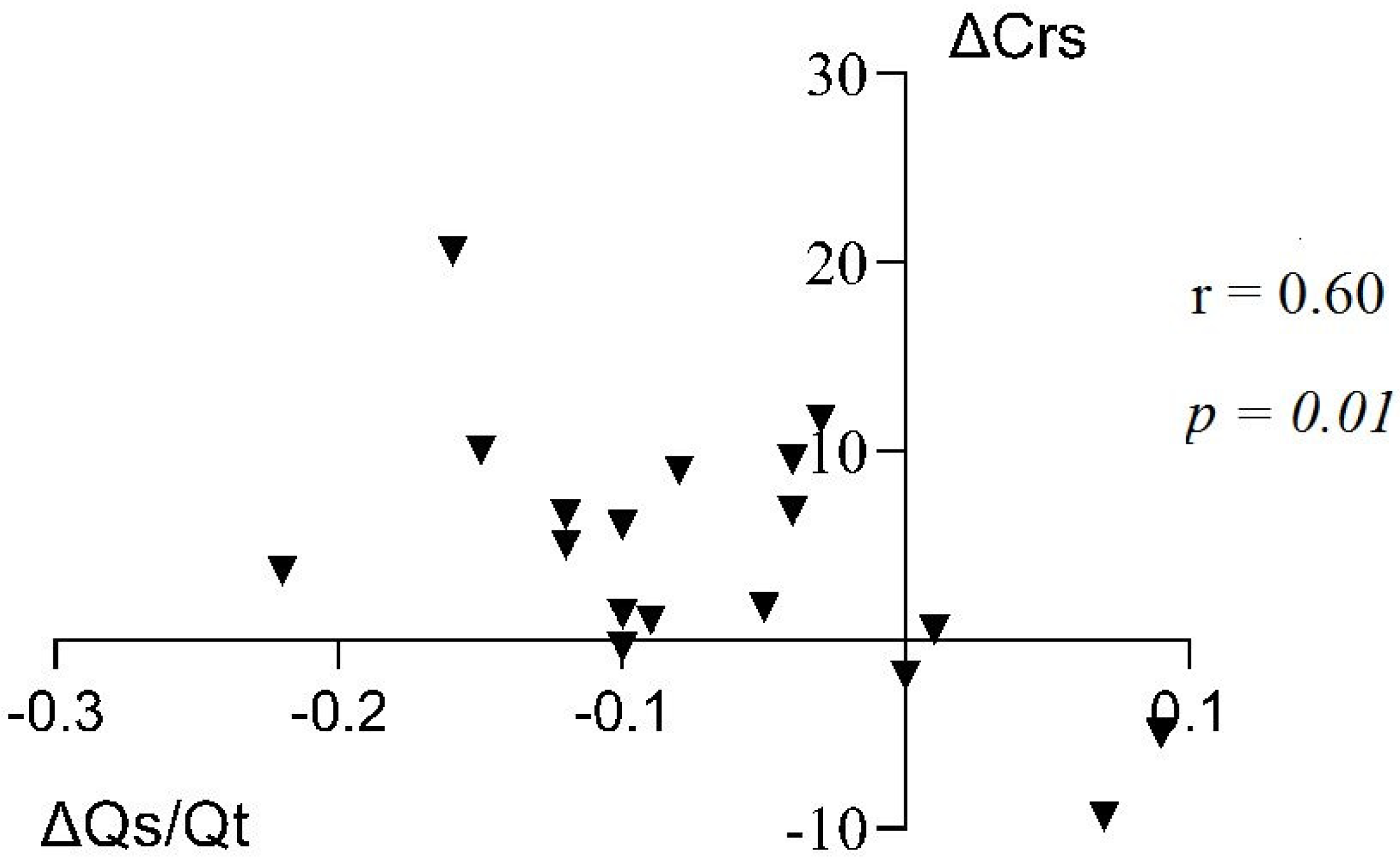
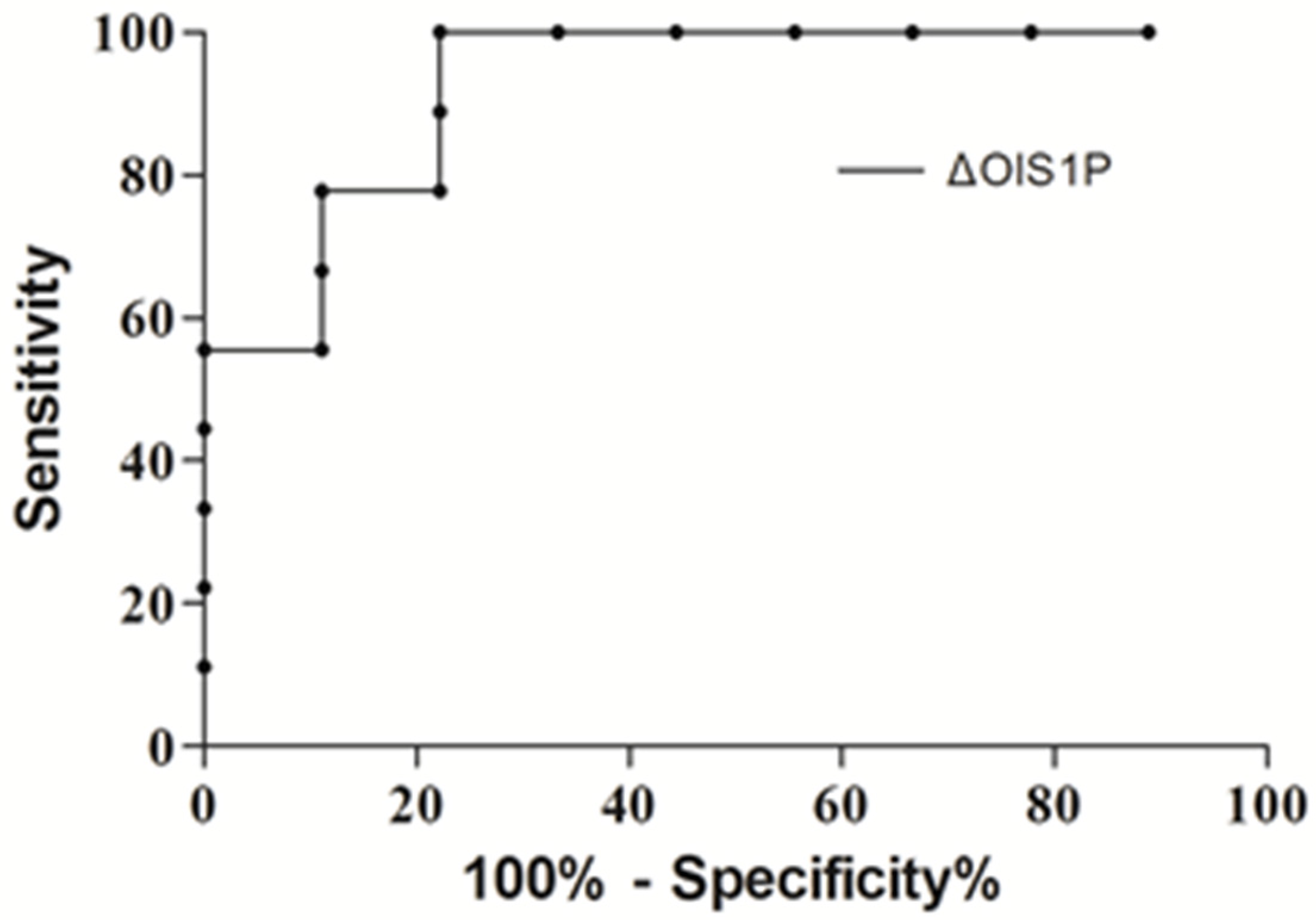
3.1. Oxygenation Changes and Their Determinants
3.2. Hemodynamic Changes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mure, M.; Martling, C.R.; Lindahl, S.G. Dramatic effect on oxygenation in patients with severe acute lung insufficiency treated in the prone position. Crit. Care Med. 1997, 25, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Douglas, W.W.; Rehder, K.; Beynen, F.M.; Sessler, A.D.; Marsh, H.M. Improved oxygenation in patients with acute respiratory failure: The prone position. Am. Rev. Respir. Dis. 1977, 115, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Sud, S.; Friedrich, J.O.; Taccone, P.; Polli, F.; Adhikari, N.K.J.; Latini, R. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Int. Care Med. 2010, 36, 585–599. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.C.; Beuret, P. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Richter, T.; Bellani, G.; Harris, R.S. Effect of prone position on regional shunt, aeration, and perfusion in experimental acute lung injury. Am. J. Respir. Crit. Care Med. 2005, 172, 480–487. [Google Scholar] [CrossRef] [Green Version]
- Albert, R.K.; Leasa, D.; Sanderson, M.; Robertson, H.T.; Hlastala, M.P. The prone position improves arterial oxygenation and reduces shunt in oleic-acid-induced acute lung injury. Am. Rev. Respir. Dis. 1987, 135, 628–633. [Google Scholar]
- Altemeier, W.A.; McKinney, S.; Krueger, M.; Glenny, R.W. Effect of posture on regional gas exchange in pigs. J. Appl. Physiol. 2004, 97, 2104–2111. [Google Scholar] [CrossRef] [Green Version]
- Jozwiak, M.; Teboul, J.-L.; Anguel, N.; Persichini, R.; Silva, S.; Chemla, D.; Richard, C.; Monnet, X. Beneficial hemodynamic effects of prone positioning in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2013, 188, 1428–1433. [Google Scholar] [CrossRef]
- Vieillard-Baron, A.; Charron, C.; Caille, V.; Belliard, G.; Page, B.; Jardin, F. Prone Positioning Unloads the Right Ventricle in Severe ARDS. Chest 2007, 132, 1440–1446. [Google Scholar] [CrossRef] [Green Version]
- Pelosi, P.; Tubiolo, D.; Mascheroni, D.; Vicardi, P.; Crotti, S.; Valenza, F.; Gattinoni, L. Effects of the prone position on respiratory mechanics and gas exchange during acute lung injury. Am. J. Respir. Crit. Care Med. 1998, 157, 387–393. [Google Scholar] [CrossRef] [Green Version]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Campo-rota, L.; Slutsky, A.S. The ARDS Definition Task Force Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Berggren, S.M. The oxygen deficit of arterial blood caused by nonventilating parts of the lung. Acta Physiol Scand. 1942, 4 (Suppl. S11), 1–92. [Google Scholar]
- Murray, J.F.; Matthay, M.A.; Luce, J.M.; Flick, M.R. An expanded definition of the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1988, 138, 720–723. [Google Scholar] [CrossRef]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung recruitment in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2006, 354, 1775–1786. [Google Scholar] [CrossRef]
- Wang, Y.; Zhong, M.; Dong, M.; Song, J.; Zheng, Y.-J.; Wu, W.; Tao, J.-L.; Zhu, L.; Zheng, X. Prone positioning improves ventilation– perfusion matching assessed by electrical impedance tomography in patients with ARDS: A prospective physiological study. Crit. Care 2022, 26, 154–164. [Google Scholar] [CrossRef]
- Fagerberg, A.; Stenqvist, O.; Åneman, A. Electrical impedance tomography applied to assess matching of pulmonary ventilation and perfusion in a porcine experimental model. Crit. Care 2009, 13, R34. [Google Scholar] [CrossRef] [Green Version]
- Blanch, L.; Mancebo, J.; Perez, M.; Martinez, M.; Mas, A.; Betbese, A.J.; Joseph, D.; Ballús, J.; Lucangelo, U.; Bak, E. Short-term effects of prone position in critically ill patients with acute respiratory distress syndrome. Int. Care Med. 1997, 23, 1033–1039. [Google Scholar] [CrossRef]
- Tawhai, M.H.; Nash, M.P.; Lin, C.-L.; Hoffman, E.A. Supine and prone differences in regional lung density and pleural pressure gradients in the human lung with constant shape. J. Appl. Physiol. 2009, 107, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Mure, M.; Domino, K.B.; Lindahl, S.G.E.; Hlastala, M.P.; Altemeier, W.A.; Glenny, R.W. Regional ventilation-perfusion distribution is more uniform in the prone position. J. Appl. Physiol. 2000, 88, 1076–1083. [Google Scholar] [CrossRef] [Green Version]
- Lamm, W.J.; Graham, M.M.; Albert, R.K. Mechanism by which the prone position improves oxygenation in acute lung injury. Am. J. Respir. Crit. Care Med. 1994, 150, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Dantzker, D.R.; Lynch, J.P.; Weg, J.G. Depression of cardiac output is a mechanism of shunt reduction in the therapy of acute respiratory failure. Chest 1980, 77, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Perrie, F.; Tuffet, S.; Maraffi, T.; Alcala, G.; Victor, M.; Haudebourg, A.-F.; De Prost, N.; Amato, M.; Carteaux, G.; Dessap, A.M. Effect of positive end-expiratory pressure and proning on ventilation and perfusion in COVID-19 acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2020, 202, 1713–1717. [Google Scholar] [CrossRef] [PubMed]
- Dell’Anna, A.M.; Carelli, S.; Cicetti, M.; Stella, C.; Bongiovanni, F.; Natalini, D.; Tanzarella, E.S.; De Santis, P.; Bocci, M.G.; De Pascale, G.; et al. Hemodynamic response to positive end-expiratory pressure and prone position in COVID-19 ARDS. Respir. Physiol. Neurobiol. 2022, 298, 103844. [Google Scholar] [CrossRef]
- Prisk, G.K.; Yamada, K.; Henderson, A.C. Pulmonary perfusion in the prone and supine postures in the normal human lung. J. Appl. Physiol. 2007, 103, 883–894. [Google Scholar] [CrossRef]
- Teboul, J.L.; Besbes, M.; Andrivet, P. A bedside index accessing the reliability of pulmonary occlusion pressure during mechanical ventilation with positive end-expiratory pressure. J. Crit. Care 1992, 7, 22–29. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age, Years | 62.8 ± 7.4 |
|---|---|
| Male gender, n (%) | 13 (72.2) |
| BSA, kg/m2 | 1.91 ± 0.26 |
| APACHE II score at admission | 17.3 ± 4.3 |
| SOFA score at inclusion | 9.34 ± 3.16 |
| PaO2/FiO2 ratio at inclusion, mmHg | 102.3 ± 29.4 |
| Oxygenation Index at inclusion | 20.6 ± 7.12 |
| Lung Injury Score at inclusion | 2.69 ± 0.54 |
| PEEP at inclusion, mbar | 9.8 ± 2.17 |
| Sepsis, n (%) | 16 (88.8%) |
| Septic shock, n (%) | 5 (27.77%) |
| Pneumonia, n (%) | 11 (61.1%) |
| Multiple Trauma n (%) | 2 (11.11%) |
| SRBAS | 1hProne | 18hProne | |
|---|---|---|---|
| NA drip, μg/kg/min | 0.26 ± 0.28 | 0.25 ± 0.24 | 0.24 ± 0.34 |
| Heart rate, bpm | 97.59 ± 18.49 | 99.1 ± 18.80 | 100.39 ± 15.93 |
| SAP, mmHg | 128 ± 17.5 | 129 ± 15.5 | 128.1 ± 16.4 |
| MAP, mmHg | 79.23 ± 9.64 | 80.7 ± 12.08 | 79.66 ± 8.25 |
| DAP, mmHg | 54.94 ± 8.31 | 58.5 ± 9.81 * | 57.88 ± 8.14 |
| MPAP, mmHg | 33.73 ± 7.49 | 34.58 ± 6.70 | 35.02 ± 1.63 |
| CVP, mmHg | 12.18 ± 4.57 | 12.76 ± 3.41 | 12.81 ± 4.66 |
| PAOP, mmHg | 14.18 ± 3.59 | 15.88 ± 3.42 * | 15.39 ± 4.57 |
| DPG, mmHg | 7.41 ± 4.87 | 7.77 ± 3.90 | 9.72 ± 3.99 |
| TPG, mmHg | 19.58 ± 5.13 | 18.77 ± 5.29 | 19.63 ± 3.92 |
| EDV, mL | 233.76 ± 51.19 | 235.35 ± 53.63 | 221.59 ± 56.77 |
| SV, mL/b | 87.12 ± 18.02 | 91.47 ± 21.98 | 89.39 ± 27.36 |
| EF % | 38.56 ± 5.85 | 38.44 ± 6.13 | 39.61 ± 5.98 |
| CO, L/min | 8.69 ± 2.53 | 8.84 ± 2.06 | 8.79 ± 2.73 |
| SVR, dyn × s/cm5 | 676.06 ± 243.39 | 668.19 ± 294.4 | 665.9 ± 298.71 |
| PVR, dyn × s/cm5 | 189.93 ± 48.55 | 182.34 ± 46.5 | 194.48 ± 55.98 |
| PEEP, mbar | 10.18 ± 1.84 | 10.06 ± 1.78 | 9.77 ± 1.80 |
| Pmean, mbar | 19.41 ± 2.29 | 19.41 ± 2.06 | 19.55 ± 0.75 |
| Tidal volume, mL | 473.24 ± 79.15 | 492.9 ± 81.85 | 512.22 ± 84.96 |
| Crs, mL/mbar | 25.3 ± 7.0 | 28.9 ± 7.0 | 29.9 ± 7.50 * |
| PO2/FiO2, mmHg | 110.3 ± 45.69 | 141.0 ± 70.95 * | 168.8 ± 63.98 * |
| OI | 20.2 ± 7.56 | 16.59 ± 6.81 | 13.11 ± 5.57 * |
| s/t | 0.30 ± 0.09 | 0.27 ± 0.08 | 0.23 ± 0.02 * |
| SaO2,% | 94.18 ± 0.03 | 94.5 ± 0.03 | 96.17 ± 0.00 * |
| CaO2, mL/dL | 14.56 ± 2.65 | 14.5 ± 3.01 | 14.61 ± 0.55 |
| PaO2, mmHg | 84.06 ± 16.79 | 102.94 ± 39.52 * | 106.32 ± 6.62 * |
| pH arterial | 7.31 ± 0.07 | 7.28 ± 0.1 | 7.33 ± 0.02 |
| PCO2, mmHg | 56.77 ± 11.78 | 59.65 ± 21 * | 52.56 ± 3.23 |
| DO2, mL/min | 1281 ± 408.18 | 1273 ± 410.29 | 1327 ± 512.91 |
| VO2, mL/min % | 303 ± 115.75 | 299 ± 115.95 | 324 ± 143.84 |
| P(v-a)CO2/C(a-v)O2 | 1.04 ± 0.91 | 1.5 ± 1.61 | 1.3 ± 0.78 |
| SvO2,% | 71.59 ± 0.05 | 73.1 ± 0.07 | 72.72 ± 0.05 |
| CvO2, mL/dL | 10.88 ± 2.21 | 11.01 ± 2.71 | 10.98 ± 1.96 |
| Correlation Coefficient * | p Value | |
|---|---|---|
| ARDS score at baseline | −0.73 | 0.009 |
| Δs/t from baseline to 1hProne | 0.55 | 0.018 |
| ΔPaCO2 from baseline to 1hProne | 0.47 | 0.045 |
| Δs/t from baseline to 18hProne | 0.75 | 0.000 |
| ΔCrs from baseline to 18hProne | −0.60 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baka, M.; Bagka, D.; Tsolaki, V.; Zakynthinos, G.E.; Diakaki, C.; Mantzarlis, K.; Makris, D. Hemodynamic and Respiratory Changes following Prone Position in Acute Respiratory Distress Syndrome Patients: A Clinical Study. J. Clin. Med. 2023, 12, 760. https://doi.org/10.3390/jcm12030760
Baka M, Bagka D, Tsolaki V, Zakynthinos GE, Diakaki C, Mantzarlis K, Makris D. Hemodynamic and Respiratory Changes following Prone Position in Acute Respiratory Distress Syndrome Patients: A Clinical Study. Journal of Clinical Medicine. 2023; 12(3):760. https://doi.org/10.3390/jcm12030760
Chicago/Turabian StyleBaka, Maria, Dimitra Bagka, Vasiliki Tsolaki, George E. Zakynthinos, Chrysi Diakaki, Konstantinos Mantzarlis, and Demosthenes Makris. 2023. "Hemodynamic and Respiratory Changes following Prone Position in Acute Respiratory Distress Syndrome Patients: A Clinical Study" Journal of Clinical Medicine 12, no. 3: 760. https://doi.org/10.3390/jcm12030760