Daytime Variation of Chloral Hydrate-Associated Sedation Outcomes: A Propensity-Matched Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Sedation Methods
2.2. Data Extraction
2.3. Outcomes
- (1)
- The sedation success rate after the second dose;
- (2)
- Final sedation failure rate (defined as the patient not being able to finish the procedure, either because of the inability of achieving a sufficient depth of sedation or waking during procedures);
- (3)
- The duration of sedation was defined from chloral hydrate administration to awakening; only patients who achieved an anticipated depth of sedation after the initial dose and completed the procedure were included in the analysis.
- (4)
- Complications (vomiting, agitation, bradycardia, delayed awakening, rash, cough, hyperthermia, hypoxia, desaturation, and mild upper airway obstruction).
- (5)
- Subgroup analysis was conducted according to males and females.
2.4. Statistical Analysis
3. Results
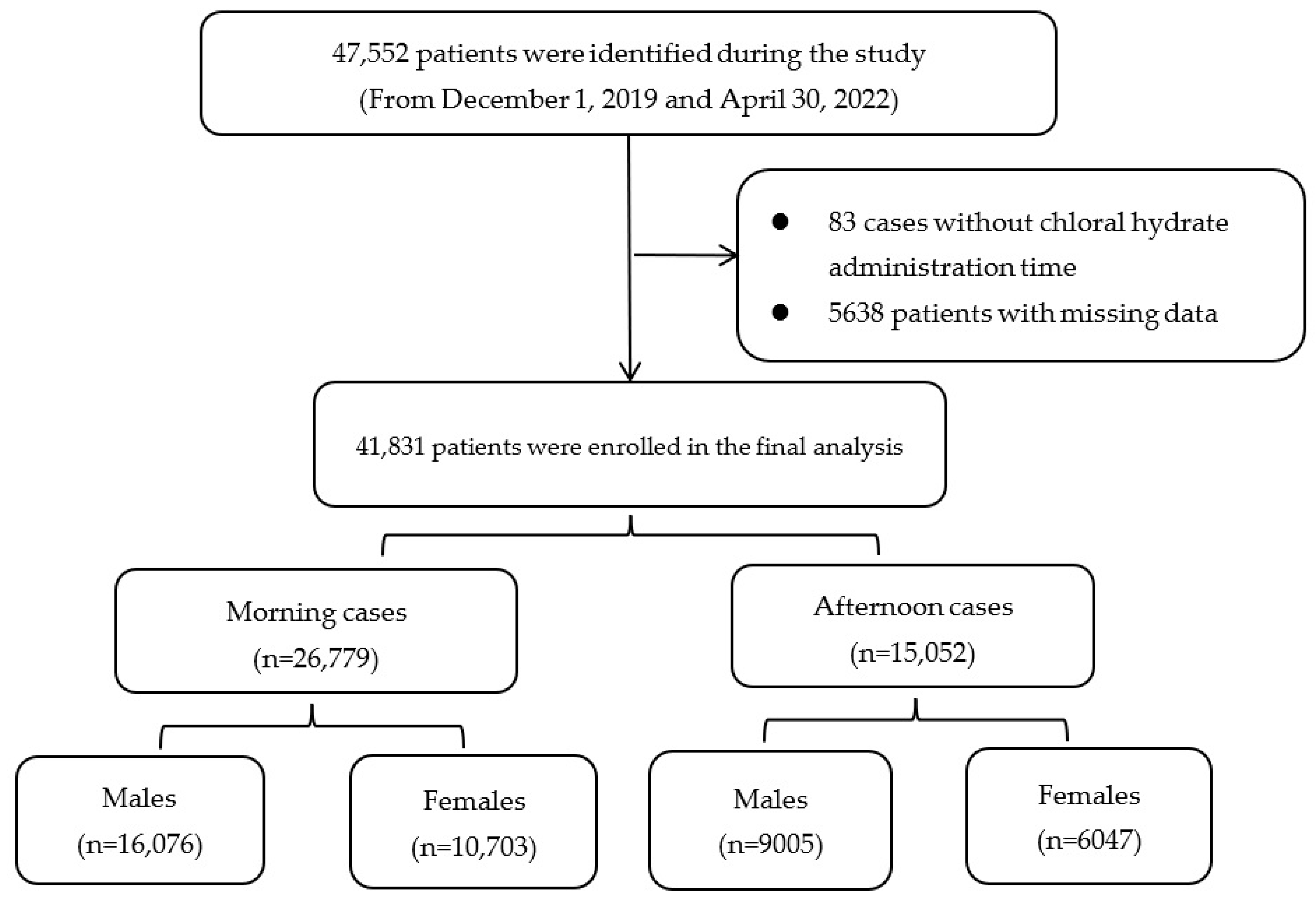
3.1. Patient Characteristics
3.2. Before Propensity Score-Matching
3.3. Primary and Secondary Outcomes before Matching
3.4. Cohorts Matched by Propensity Score
3.5. Sedation Success Rate after Matching
3.6. Sedation Duration and Complications after Matching
3.7. Subgroup Analysis Based on Gender
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pershad, J.; Palmisano, P.; Nichols, M. Chloral hydrate: The good and the bad. Pediatr. Emerg. Care 1999, 15, 432–435. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre (UK). Sedation in Children and Young People: Sedation for Diagnostic and Therapeutic Procedures in Children and Young People; Royal College of Physicians: London, UK, 2010. [Google Scholar]
- Cui, Y.; Guo, L.; Mu, Q.; Kang, L.; Chen, Q.; Wu, Q.; He, Y.; Tang, M. Analysis of Risk Factors for Chloral Hydrate Sedative Failure with Initial Dose in Pediatric Patients: A Retrospective Analysis. Paediatr. Drugs 2022, 24, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.; Simsek, E.; Gazeteci Tekin, H.; Aktan, G.; Gokben, S.; Tekgul, H. Melatonin Versus Chloral Hydrate for Sleep Electroencephalography Recording in Children: A Comparative Study Using Bispectral Index Monitoring Scores and Electroencephalographic Sleep Stages. J. Clin. Neurophysiol. 2021, 7, 625–630. [Google Scholar] [CrossRef]
- Moon, J.U.; Han, J.Y. Effectiveness of Chloral Hydrate on Brain MRI in Children with Developmental Delay/Intellectual Disability Comparing with Normal Intelligence: Single Tertiary Center Experience. Children 2021, 8, 1097. [Google Scholar] [CrossRef]
- Tsuji, T.; Sato, I.; Kamimura, Y.; Ota, H.; Takeda, C.; Sobue, K.; Kawakami, K. Trends and patterns in the practice of pediatric sedation for magnetic resonance imaging in Japan: A longitudinal descriptive study from 2012 to 2019. Paediatr. Anaesth. 2022, 32, 673–684. [Google Scholar] [CrossRef]
- Ballarín, J.S.; Guixes, J.S.; Botella, M.G.; Palacín, J.S. Use of a single dose of 70 mg/kg chloral hydrate as a hypnotic in nuclear magnetic resonance. A prospective study of 3132 cases. Uso de hidrato de cloral a dosis única de 70 mg/kg como hipnótico en resonancia magnética nuclear. Estudio prospectivo de 3.132 casos. Rev. Esp. Anestesiol. Reanim. 2021, 69, 355–359. [Google Scholar] [CrossRef]
- Luque, C.G.; Atkins-Labelle, C.; Pauwels, J.; Costello, R.; Kozak, F.K.; Chadha, N.K. Intranasal Dexmedetomidine increases the successful sedation of children with autism for out-patient auditory brainstem response hearing tests. Int. J. Pediatr. Otorhinolaryngol. 2021, 151, 110945. [Google Scholar] [CrossRef]
- Nordt, S.P.; Rangan, C.; Hardmaslani, M.; Clark, R.F.; Wendler, C.; Valente, M. Pediatric chloral hydrate poisonings and death following outpatient procedural sedation. J. Med. Toxicol. 2014, 10, 219–222. [Google Scholar] [CrossRef]
- Many, Y.A.; Berkenstadt, H.; Henkin, Y. The safety and efficacy of a nurse-led sedation service using Chloral Hydrate for auditory brainstem response testing. J. Pediatr. Nurs. 2022, 63, e143–e148. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.Y.; Kim, Y.J.; Park, Y.S.; Park, J.; Song, M.H.; Hahm, K.D.; Choi, I.C. Intramuscular dexmedetomidine and oral chloral hydrate for pediatric sedation for electroencephalography: A propensity score-matched analysis. Paediatr. Anaesth. 2020, 30, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Potts, A.L.; Cheeseman, J.F.; Warman, G.R. Circadian rhythms and their development in children: Implications for pharmacokinetics and pharmacodynamics in anesthesia. Paediatr. Anaesth. 2011, 21, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Szolnoki, J.; Polaner, D.M.; Eckle, T. Diurnal variations in recovery times after general anaesthesia in children. Br. J. Anaesth. 2018, 121, 776–786. [Google Scholar] [CrossRef] [PubMed]
- Dispersyn, G.; Pain, L.; Touitou, Y. Propofol anesthesia significantly alters plasma blood levels of melatonin in rats. Anesthesiology 2010, 112, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Santhi, N.; Lazar, A.S.; McCabe, P.J.; Lo, J.C.; Groeger, J.A.; Dijk, D.J. Sex differences in the circadian regulation of sleep and waking cognition in humans. Proc. Natl. Acad. Sci. USA 2016, 113, E2730–E2739. [Google Scholar] [CrossRef]
- Malviya, S.; Voepel-Lewis, T.; Tait, A.R.; Reynolds, P.I.; Gujar, S.K.; Gebarski, S.S.; Petter Eldevik, O. Pentobarbital vs chloral hydrate for sedation of children undergoing MRI: Efficacy and recovery characteristics. Paediatr. Anaesth. 2004, 14, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Yuen, V.M.; Li, B.L.; Cheuk, D.K.; Leung, M.K.M.; Hui, T.W.C.; Wong, I.C.; Lam, W.W.; Choi, S.W.; Irwin, M.G. A randomised controlled trial of oral chloral hydrate vs. intranasal dexmedetomidine before computerised tomography in children. Anaesthesia 2017, 72, 1191–1195. [Google Scholar] [CrossRef]
- Gumus, H.; Bayram, A.K.; Poyrazoglu, H.G.; Canpolat, D.G.; Per, H.; Canpolat, M.; Yildiz, K.; Kumandas, S. Comparison of Effects of Different Dexmedetomidine and Chloral Hydrate Doses Used in Sedation on Electroencephalography in Pediatric Patients. J. Child. Neurol. 2015, 30, 983–988. [Google Scholar] [CrossRef]
- Brainard, J.; Gobel, M.; Bartels, K.; Scott, B.; Koeppen, M.; Eckle, T. Circadian rhythms in anesthesia and critical care medicine: Potential importance of circadian disruptions. Semin. Cardiothorac. Vasc. Anesth. 2015, 19, 49–60. [Google Scholar] [CrossRef]
- Hermida, R.C.; Ayala, D.E.; Fernández, J.R.; Mojón, A.; Crespo, J.J.; Rios, M.T.; Smolensky, M.H. Bedtime Blood Pressure Chronotherapy Significantly Improves Hypertension Management. Heart Fail. Clin. 2017, 13, 759–773. [Google Scholar] [CrossRef]
- Cousins, J.N.; Leong, R.L.; Jamaluddin, S.A.; Ng, A.S.; Ong, J.L.; Chee, M.W. Splitting sleep between the night and a daytime nap reduces homeostatic sleep pressure and enhances long-term memory. Sci. Rep. 2021, 11, 5275. [Google Scholar] [CrossRef]
- Mason, G.M.; Kurdziel, L.B.F.; Spencer, R.M.C. The memory benefits of two naps per day during infancy: A pilot investigation. Infant Behav. Dev. 2021, 65, 101647. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 41,831) | Propensity Score Matched Pairs (n = 7816) | |||||
|---|---|---|---|---|---|---|
| Morning Cases (n = 26,779) | Afternoon Cases (n = 15,052) | p Values | Morning Cases (n = 3907) | Afternoon Cases (n = 3907) | p Values | |
| Male, n (%) | 16,076 (60.0) | 9005 (59.8) | 0.69 | 2246 (57.5) | 2327 (59.6) | 0.07 |
| Age, months, median (IQR) | 12.2 (4.0, 27.3) | 18.2 (6.0, 33.3) | <0.01 * | 18.2 (6.0, 29.3) | 18.2 (6.0, 29.3) | 1.00 |
| Weight, kg, median (IQR) | 9.5 (6.5, 12.5) | 10.5 (7.5, 13.5) | <0.01 * | 10.5 (8.0, 13.0) | 10.5 (8.0, 13.0) | 1.00 |
| Types of patient, outpatients, n (%) | 16,982 (63.4) | 9803 (65.1) | <0.01 * | 2942 (75.3) | 2942 (75.3) | 1.00 |
| Patients with sedation history, n (%) | 9039 (33.8) | 4577 (30.4) | <0.01 * | 1082 (27.7) | 1082 (27.7) | 1.00 |
| Sleep deprivation, yes, n (%) | 11,629 (43.4) | 6532 (43.4) | 0.96 | 1921 (49.2) | 1921 (49.2) | 1.00 |
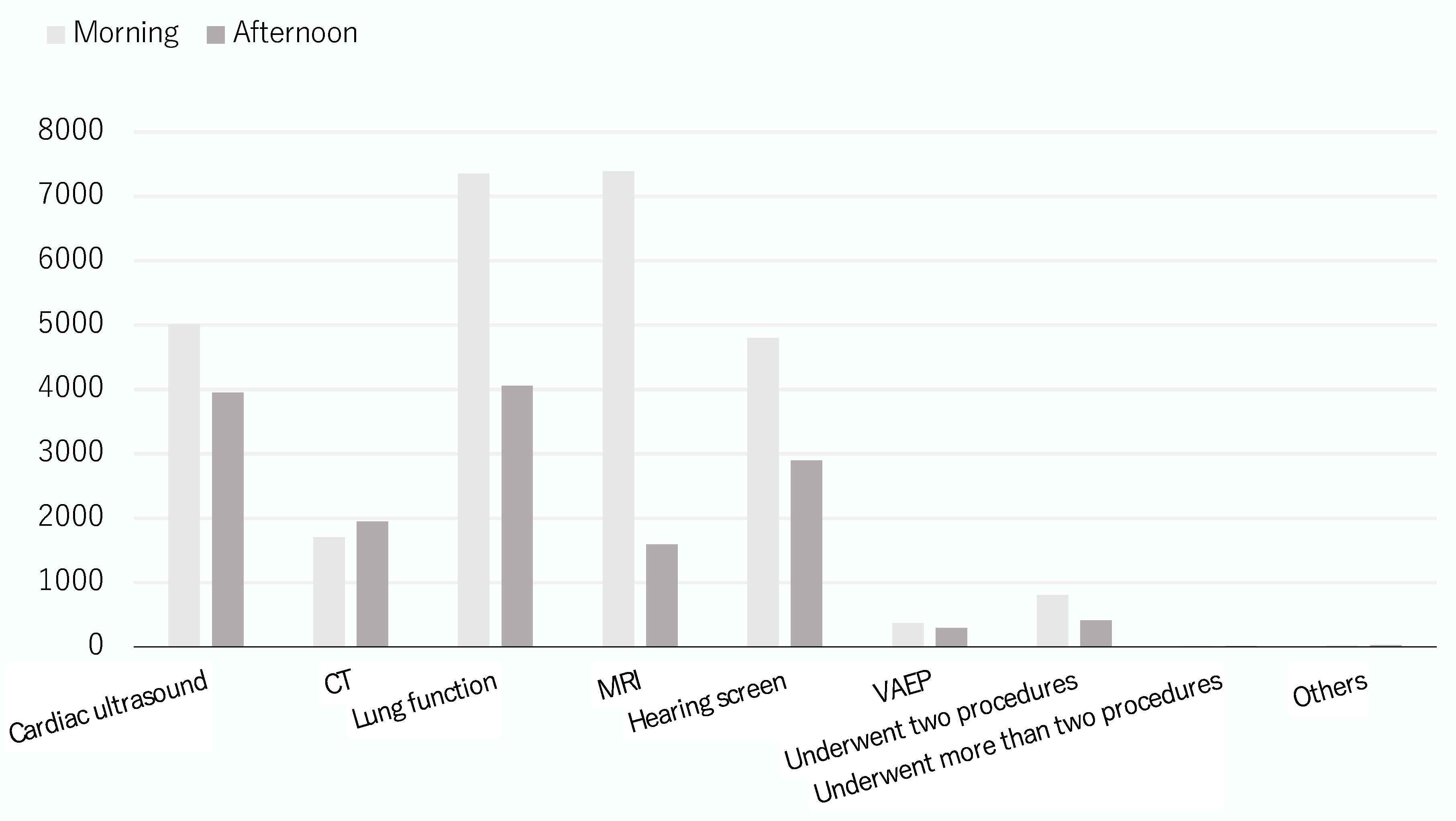
| Procedures, n (%) | <0.01 * | 1.00 | ||||
| Cardiac ultrasound | 5013 (18.8) | 3942 (26.2) | 1099 (28.1) | 1099 (28.1) | ||
| CT | 1687 (6.3) | 1932 (12.8) | 262 (6.7) | 262 (6.7) | ||
| Lung function | 7345 (27.4) | 4056 (26.9) | 1219 (31.2) | 1219 (31.2) | ||
| MRI | 6805 (25.4) | 1533 (10.2) | 395 (10.1) | 395 (10.1) | ||
| Hearing screen | 4796 (17.9) | 2895 (19.2) | 917 (23.5) | 917 (23.5) | ||
| VAEP | 343 (1.3) | 260 (1.7) | 6 (0.2) | 6 (0.2) | ||
| Others | 26 (0.1) | 27 (0.2) | 0 (0.0) | 0 (0.0) | ||
| Underwent two procedures | 750 (2.8) | 396 (2.6) | 9 (0.2) | 9 (0.2) | ||
| Underwent more than two procedures | 14 (0.1) | 11 (0.1) | 0 (0.0) | 0 (0.0) | ||
| All Patients (n = 41,831) | Propensity Score Matched Patients (n = 7814) | |||||
|---|---|---|---|---|---|---|
| Morning Cases (n = 26,779) | Afternoon Cases (n = 15,052) | p Values | Morning Cases (n = 3907) | Afternoon Cases (n = 3907) | p Values | |
| Primary outcome | ||||||
| Sedation success with initial dose, n (%) | 23,238 (86.8) | 13,069 (86.8) | 0.90 | 3364 (86.1) | 3435 (87.9) | 0.02 * |
| Initial dose of chloral hydrate, mg/kg, median (IQR); Mean ± SD | 50.0 (50.0, 50.0) 50.1 ± 2.2 | 50.0 (50.0, 50.0) 50.0 ± 2.0 | 0.25 | 50.0 (50.0, 50.0) 50.0 ± 1.5 | 50.0 (50.0, 50.0) 49.9 ± 1.4 | 0.01 * |
| Secondary outcomes | ||||||
| Sedation success rate with a rescue dose, n (%) | 1636 (6.1) | 711 (4.7) | <0.01 * | 238 (6.2) | 160 (4.4) | <0.01 * |
| Rescue sedatives, n (%) | <0.01 * | 0.53 | ||||
| Chloral hydrate | 1200 (4.5) | 478 (3.2) | 171 (4.4) | 110 (2.8) | ||
| Midazolam | 75 (0.3) | 42 (0.3) | 14 (0.4) | 10 (0.3) | ||
| Dexmedetomidine | 354 (1.3) | 185 (1.2) | 57 (1.5) | 38 (1.0) | ||
| Propofol | 7 (0.0) | 6 (0.0) | 1 (0.0) | 2 (0.1) | ||
| Final sedation success rate, n (%) | 24,874 (92.9) | 13,780 (91.5) | <0.01 * | 3601 (92.2) | 3594 (92.0) | 0.80 |
| Sedation duration, min, median (IQR) | 63.0 (50.0, 80.5) n = 20,961 | 59.0 (47.0, 75.0) n = 11,591 | <0.01 * | 65.0 (51.0, 81.0) n = 2950 | 60.0 (48.0, 75.0) n = 3069 | <0.01 |
| Complications, n (%) | ||||||
| Vomiting | 406 (1.5) | 154 (1.0) | <0.01 * | 60 (1.6) | 33 (0.9) | <0.01 * |
| Agitation | 8 (0.0) | 6 (0.0) | 0.79 | 1 (0.0) | 1 (0.0) | 1.00 |
| Cough | 1 (0.0) | 1 (0.0) | 1.00 | 0 (0.0) | 0 (0.0) | NA |
| Bradycardia | 1 (0.0) | 1 (0.0) | 1.00 | 0 (0.0) | 0 (0.0) | NA |
| Delayed awakening | 2 (0.0) | 1 (0.0) | 1.00 | 0 (0.0) | 0 (0.0) | NA |
| Hyperthermia | 0 (0.0) | 2 (0.0) | 0.25 | 0 (0.0) | 1 (0.0) | 1.00 |
| Rash | 2 (0.0) | 0 (0,0) | 0.75 | 1 (0.0) | 0 (0.0) | 1.00 |
| Desaturation | 15 (0.1) | 5 (0.0) | 0.43 | 1 (0.0) | 1 (0.0) | 1.00 |
| Male | ||||||
| Before Match (n = 25,081) | Propensity Score Matched Patients (n = 4910) | |||||
| Before 12 P.M. (n = 16,076) | After 12 P.M. (n = 9005) | p Values | Before 12 P.M. (n = 2455) | After 12 P.M. (n = 2455) | p Values | |
| Age, months, median (IQR) | 12.2 (4.4, 27.3) | 19.1 (6.1, 34.3) | <0.01 * | 19.2 (8.4, 30.3) | 19.2 (8.4, 30.3) | 1.00 |
| Types of patient, outpatients, n (%) | 10,302 (64.0) | 5932 (65.9) | <0.01 * | 1846 (75.2) | 1846 (75.2) | 1.00 |
| Sleep deprivation, yes, n (%) | 7036 (46.8) | 3941 (47.4) | 1.00 | 1211 (51.2) | 1211 (51.2) | 1.00 |
| Procedures, n (%) | <0.01 * | 1.00 | ||||
| Cardiac ultrasound | 2865 (17.8) | 2222 (24.7) | 628 (25.6) | 628 (25.6) | ||
| CT | 978 (6.1) | 1152 (12.8) | 158 (6.4) | 158 (6.4) | ||
| Lung function | 4582 (28.5) | 2556 (28.4) | 873 (35.6) | 873 (35.6) | ||
| MRI | 4147 (27.8) | 933 (10.4) | 257 (10.5) | 257 (10.5) | ||
| Hearing screen | 2753 (17.1) | 1725 (19.2) | 525 (21.4) | 525 (21.4) | ||
| VAEP | 216 (1.3) | 157 (1.7) | 6 (0.2) | 6 (0.2) | ||
| Others | 15 (0.1) | 11 (0.1) | 0 (0.0) | 0 (0.0) | ||
| Underwent two procedures | 511 (3.2) | 240 (2.7) | 8 (0.3) | 7 (0.3) | ||
| Underwent more than two procedures | 9 (0.1) | 9 (0.1) | 0 (0.0) | 0 (0.0) | ||
| Success with initial dose, n (%) | 14,022 (87.2) | 7820 (86.8) | 0.40 | 2094 (85.3) | 2153 (87.7) | 0.02 * |
| The initial dose of chloral hydrate, mg/kg, median (IQR) | 50.0 (50.0, 50.0) | 50.0 (50.0, 50.0) | 0.28 | 50.0 (50.0, 50.0) | 50.0 (50.0, 50.0) | 0.09 |
| Success with a rescue dose, n (%) | 947 (5.9) | 435 (4.8) | <0.01 * | 163 (6.6) | 111 (4.5) | <0.01 * |
| Rescue sedatives, n (%) | <0.01 * | 0.51 | ||||
| Chloral hydrate | 726 (4.5) | 303 (3.4) | 128 (5.2) | 81 (3.3) | ||
| Midazolam | 45 (0.3) | 27 (0.3) | 3 (0.1) | 4 (0.2) | ||
| Dexmedetomidine | 221 (1.4) | 127 (1.4) | 31 (1.3) | 26 (1.1) | ||
| Propofol | 5 (0.0) | 2 (0.0) | 1 (0.0) | 0 (0.0) | ||
| Final sedation failure, n (%) | 1107 (6.9) | 750 (8.3) | <0.01 * | 198 (8.1) | 191 (7.8) | 0.75 |
| Sedation duration, min, Median (IQR) | 65.0 (50.0, 84.0) (n = 12,635) | 60 (47.0, 76.0) (n = 6960) | <0.01 * | 64.0 (50.0, 80.0) (n = 1835) | 60.0 (47.0, 75.0) (n = 1934) | 0.07 |
| Female | ||||||
| Before Match (n = 16,750) | Propensity Score Matched Patients (n = 2804) | |||||
| Before 12 P.M. (n = 10,703) | After 12 P.M. (n = 6047) | p Values | Before 12 P.M. (n = 1402) | After 12 P.M. (n = 1402) | p Values | |
| Age, months, median (IQR) | 11.0 (4.0, 25.3) | 17.2 (6.0, 32.3) | <0.01 * | 17.2 (6.0, 28.3) | 17.2 (6.0, 28.3) | 1.00 |
| Types of patient, outpatients, n (%) | 6680 (62.4) | 3871 (64.0) | 0.04 * | 1037 (74.0) | 1037 (74.0) | 1.00 |
| Sleep deprivation, yes, n (%) | 4590 (45.9) | 2591 (46.6) | 0.98 | 693 (52.0) | 694 (49.5) | 1.00 |
| Sedation history, yes, n (%) | 3547 (33.1) | 1709 (28.3) | <0.01 * | 512 (36.5) | 425 (30.3) | 0.26 |
| Procedures, n (%) | <0.01 * | 1.00 | ||||
| Cardiac ultrasound | 2148 (20.1) | 1720 (28.4) | 466 (33.2) | 466 (33.2) | ||
| CT | 709 (6.6) | 780 (12.9) | 96 (6.8) | 96 (6.8) | ||
| Lung function | 2763 (25.8) | 1500 (24.8) | 377 (26.9) | 377 (26.9) | ||
| MRI | 2658 (24.8) | 600 (9.9) | 124 (8.8) | 124 (8.8) | ||
| Hearing screen | 2043 (19.1) | 1170 (19.3) | 335 (23.9) | 335 (23.9) | ||
| VAEP | 127 (1.2) | 103 (1.7) | 2 (0.1) | 2 (0.1) | ||
| Others | 11 (0.1) | 16 (0.3) | 0 (0.0) | 0 (0.0) | ||
| Underwent two procedures | 239 (2.2) | 156 (2.6) | 2 (0.1) | 2 (0.1) | ||
| Underwent more than two procedures | 5 (0.0) | 2 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Success with initial dose, n (%) | 9216 (86.1) | 5249 (86.8) | 0.22 | 1184 (84.5) | 1221 (87.1) | 0.05 |
| The initial dose of chloral hydrate, mg/kg, Median (IQR) | 50.0 (50.0, 50.0) | 50.0 (50.0, 50.0) | 0.61 | 50.0 (50.0, 50.0) | 50.0 (50.0, 50.0) | 0.08 |
| Success with a rescue dose, n (%) | 689 (6.4) | 276 (4.6) | <0.01 * | 76 (5.4) | 51 (3.6) | 0.03 * |
| Rescue sedatives, n (%) | 0.12 | 0.74 | ||||
| Chloral hydrate | 519 (4.8) | 195 (3.2) | 57 (4.1) | 38 (2.7) | ||
| Midazolam | 31 (0.3) | 15 (0.2) | 3 (0.2) | 1 (0.1) | ||
| Dexmedetomidine | 137 (1.3) | 62 (1.0) | 16 (1.1) | 11 (0.8) | ||
| Propofol | 2 (0.0) | 4 (0.1) | 0 (0.0) | 1 (0.1) | ||
| Final sedation failure, n (%) | 798 (7.3) | 522 (8.6) | <0.01 * | 142 (10.1) | 130 (9.3) | 0.48 |
| Sedation duration, min, median (IQR) | 65.0 (50.0, 82.0) (n = 8326) | 60.0 (47.0, 75.0) (n = 4361) | <0.01 * | 65.0 (51.0, 81.0) (n = 1032) | 62.0 (50.0,77.0) (n = 1078) | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Guo, L.; Xu, L.; Mu, Q.; Wu, Q.; Kang, L.; Chen, Q.; He, Y.; Liu, H. Daytime Variation of Chloral Hydrate-Associated Sedation Outcomes: A Propensity-Matched Cohort Study. J. Clin. Med. 2023, 12, 1245. https://doi.org/10.3390/jcm12031245
Cui Y, Guo L, Xu L, Mu Q, Wu Q, Kang L, Chen Q, He Y, Liu H. Daytime Variation of Chloral Hydrate-Associated Sedation Outcomes: A Propensity-Matched Cohort Study. Journal of Clinical Medicine. 2023; 12(3):1245. https://doi.org/10.3390/jcm12031245
Chicago/Turabian StyleCui, Yu, Langtao Guo, Li Xu, Qixia Mu, Qunying Wu, Lu Kang, Qin Chen, Yani He, and Hong Liu. 2023. "Daytime Variation of Chloral Hydrate-Associated Sedation Outcomes: A Propensity-Matched Cohort Study" Journal of Clinical Medicine 12, no. 3: 1245. https://doi.org/10.3390/jcm12031245