Use of Direct Acting Oral Anticoagulants in Elderly Patients with Atrial Fibrillation: A Multicenter, Cross-Sectional Study in Spain

 , , ,
, , ,  ,
on behalf of RE_BELD Spanish Investigator’s Group
,
on behalf of RE_BELD Spanish Investigator’s Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Subjects
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Population Baseline Characteristics
3.2. Patient Characteristics according to NOAC Treatment
3.3. Previous Thromboembolic and Bleeding Events
3.4. NOAC Prescription Patterns: Indications, Dose Appropriateness, and Treatment
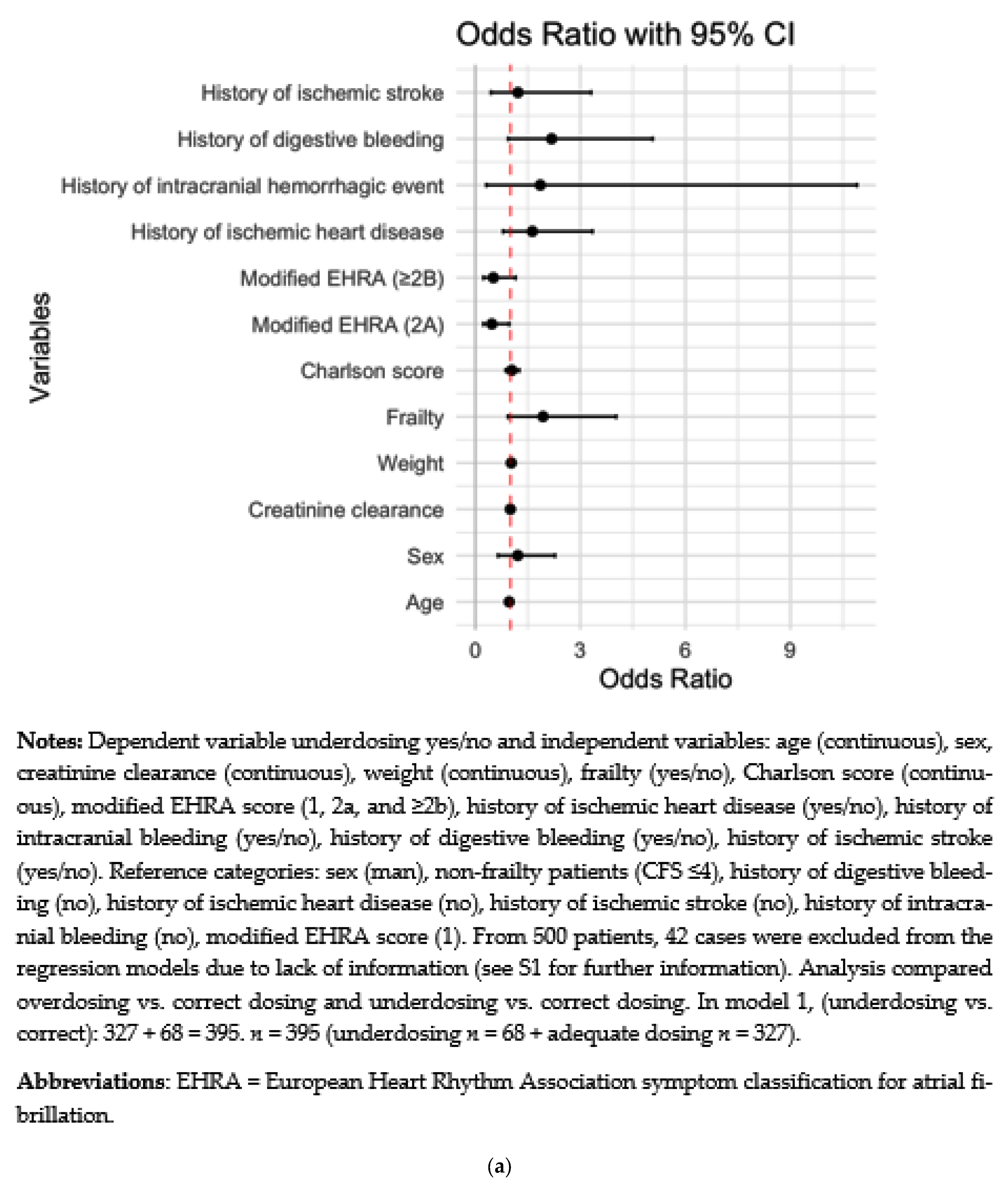
3.5. Factors Influencing under and Overdosing
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krijthe, B.P.; Kunst, A.; Benjamin, E.J.; Lip, G.Y.; Franco, O.H.; Hofman, A.; Witteman, J.C.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef]
- Pathak, R.K.; Middeldorp, M.E.; Lau, D.H.; Mehta, A.B.; Mahajan, R.; Twomey, D.; Alasady, M.; Hanley, L.; Antic, N.A.; McEvoy, R.D.; et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: The ARREST-AF cohort study. J. Am. Coll. Cardiol. 2014, 64, 2222–2231. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef]
- Chao, T.F.; Liu, C.J.; Chen, S.J.; Wang, K.L.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Wu, T.J.; et al. Atrial fibrillation and the risk of ischemic stroke: Does it still matter in patients with a CHA2DS2-VASc score of 0 or 1? Stroke 2012, 43, 2551–2555. [Google Scholar] [CrossRef]
- Petidier Torregrossa, R.; Abizanda Soler, P.; Noguerón García, A.; Gonzalo Lázaro, M.; Gutiérrez Rodríguez, J.; Gil Gregorio, P.; Martín-Sánchez, F.J.; Ruíz-Artacho, P.; Duems Noriega, Ó.; Veiga Fernández, F. Oral anticoagulation therapy in the elderly population with atrial fibrillation. A review article. Rev. Esp. Geriatr. Gerontol. 2018, 53, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, D.; Nunes-Ferreira, A.; Rodrigues, R.; Vicente, E.; Pinto, F.J.; Ferreira, J.J. Non-vitamin K antagonist oral anticoagulants in elderly patients with atrial fibrillation: A systematic review with meta-analysis and trial sequential analysis. Arch. Gerontol. Geriatr. 2019, 81, 209–214. [Google Scholar] [CrossRef]
- Lip, G.Y.; Clementy, N.; Pericart, L.; Banerjee, A.; Fauchier, L. Stroke and major bleeding risk in elderly patients aged ≥ 75 years with atrial fibrillation: The Loire Valley atrial fibrillation project. Stroke 2015, 46, 143–150. [Google Scholar] [CrossRef]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Grant, S.J.; Kothari, S.; Gimotty, P.A.; Gooneratne, N.S.; Cuker, A. Quality of direct oral anticoagulant prescribing in elderly patients with non-valvular atrial fibrillation: Results from a large urban health system. J. Thromb. Thrombolysis 2018, 46, 1–6. [Google Scholar] [CrossRef]
- Pattullo, C.S.; Barras, M.; Tai, B.; McKean, M.; Donovan, P. New oral anticoagulants: Appropriateness of prescribing in real-world setting. Intern. Med. J. 2016, 46, 812–818. [Google Scholar] [CrossRef]
- Barra, M.E.; Fanikos, J.; Connors, J.M.; Sylvester, K.W.; Piazza, G.; Goldhaber, S.Z. Evaluation of Dose-Reduced Direct Oral Anticoagulant Therapy. Am. J. Med. 2016, 129, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Stöllberger, C.; Brooks, R.; Finsterer, J.; Pachofszky, T. Use of Direct-Acting Oral Anticoagulants in Nonagenarians: A Call for More Data. Drugs Aging 2016, 33, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Raparelli, V.; Diemberger, I.; Boriani, G.; Dalla Vecchia, L.A.; Bellelli, G.; Marzetti, E.; Lip, G.Y.; Cesari, M. Frailty prevalence and impact on outcomes in patients with atrial fibrillation: A systematic review and meta-analysis of 1,187,000 patients. Ageing Res. Rev. 2022, 79, 101652. [Google Scholar] [CrossRef]
- Madhavan, M.; Holmes, D.N.; Piccini, J.P.; Ansell, J.E.; Fonarow, G.C.; Hylek, E.M.; Kowey, P.R.; Mahaffey, K.W.; Thomas, L.; Peterson, E.D.; et al. Association of frailty and cognitive impairment with benefits of oral anticoagulation in patients with atrial fibrillation. Am. Heart J. 2019, 211, 77–89. [Google Scholar] [CrossRef]
- Orlandi, M.; Dover, D.C.; Sandhu, R.K.; Hawkins, N.M.; Kaul, P.; McAlister, F.A. The Introduction of Direct Oral Anticoagulants Has Not Resolved Treatment Gaps for Frail Patients with Nonvalvular Atrial Fibrillation. Can. J. Cardiol. 2022, 38, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Romiti, G.F.; Vitolo, M.; Harrison, S.L.; Lane, D.A.; Fauchier, L.; Marin, F.; Näbauer, M.; Potpara, T.S.; Dan, G.-A.; et al. Epidemiology and impact of frailty in patients with atrial fibrillation in Europe. Age Ageing 2022, 51, afac192. [Google Scholar] [CrossRef] [PubMed]
- Díez-Villanueva, P.; Arizá-Solé, A.; Vidán, M.T.; Bonanad, C.; Formiga, F.; Sanchis, J.; Martín-Sánchez, F.J.; Ruiz Ros, V.; Sanmartín Fernández, M.; Bueno, H.; et al. Recommendations of the Geriatric Cardiology Section of the Spanish Society of Cardiology for the Assessment of Frailty in Elderly Patients with Heart Disease. Rev. Esp. Cardiol. 2019, 72, 63–71. [Google Scholar] [CrossRef]
- Tayaa, S.; Berrut, G.; de Decker, L.; Chevalet, P. Direct oral anticoagulants in non-valvular atrial fibrillation in elderly: For a treatment adapted to patient profile. Geriatr. Psychol. Neuropsychiatr. Vieil. 2018, 16, 229–240. [Google Scholar] [CrossRef]
- Martín-Asenjo, R.; Bueno, H.; Vidán, M.T. Anticoagulation in the elderly: Is it all about guidelines or there room for the art of medicine? Rev. Esp. Geriatr. Gerontol. 2018, 53, 314–316. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Cmaj 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef]
- Cohen, J. The statistical power of abnormal-social psychological research: A review. J. Abnorm. Soc. Psychol. 1962, 65, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- García Rodríguez, L.A.; Martín-Pérez, M.; Vora, P.; Roberts, L.; Balabanova, Y.; Brobert, G.; Fatoba, S.; Suzart-Woischnik, K.; Schaefer, B.; Ruigomez, A. Appropriateness of initial dose of non-vitamin K antagonist oral anticoagulants in patients with non-valvular atrial fibrillation in the UK. BMJ Open 2019, 9, e031341. [Google Scholar] [CrossRef] [PubMed]
- Sanghai, S.; Wong, C.; Wang, Z.; Clive, P.; Tran, W.; Waring, M.; Goldberg, R.; Hayward, R.; Saczynski, J.S.; McManus, D.D. Rates of Potentially Inappropriate Dosing of Direct-Acting Oral Anticoagulants and Associations with Geriatric Conditions Among Older Patients with Atrial Fibrillation: The SAGE-AF Study. J. Am. Heart Assoc. 2020, 9, e014108. [Google Scholar] [CrossRef] [PubMed]
- Raposeiras-Roubín, S.; Alonso Rodríguez, D.; Camacho Freire, S.J.; Abu-Assi, E.; Cobas-Paz, R.; Rodríguez Pascual, C.; García Comesaña, J.; González-Carrero López, A.; Cubelos Fernández, N.; López-Masjuán Ríos, Á.; et al. Vitamin K Antagonists and Direct Oral Anticoagulants in Nonagenarian Patients with Atrial Fibrillation. J. Am. Med. Dir. Assoc. 2020, 21, 367–373.e361. [Google Scholar] [CrossRef]
- Domínguez-Erquicia, P.; Raposeiras-Roubín, S.; Abbu-Assi, E.; Cespón-Fernández, M.; Alonso-Rodríguez, D.; Camacho-Freire, S.J.; Cubelos-Fernández, N.; López-Masjuán Ríos, Á.; Melendo-Viu, M.; Iñíguez-Romo, A. Predictors of Inappropriate Dosing of Direct Oral Anticoagulants in Nonagenarian Patients with Atrial Fibrillation. J. Am. Med. Dir. Assoc. 2021, 22, 2395–2397. [Google Scholar] [CrossRef]
- Spanish Health Authority Therapeutic Positioning Report. General Criteria and Recommendations for the Use of Direct Oral Anticoagulants (NOAC) in the Prevention of Stroke and Systemic Embolism in Patients with Non-Valvular Atrial Fibrillation; Spanish Agency of Medicines and Medical Products: Madrid, Spain, 2016. [Google Scholar]
- Durán-Bobín, O.; Elices-Teja, J.; González-Melchor, L.; Vázquez-Caamaño, M.; Fernández-Obanza, E.; González-Babarro, E.; Cabanas-Grandío, P.; Piñeiro-Portela, M.; Prada-Delgado, O.; Gutiérrez-Feijoo, M.; et al. Differences in the Clinical Profile and Management of Atrial Fibrillation According to Gender. Results of the REgistro GallEgo Intercéntrico de Fibrilación Auricular (REGUEIFA) Trial. J. Clin. Med. 2021, 10, 3846. [Google Scholar] [CrossRef]
- Oqab, Z.; Pournazari, P.; Sheldon, R.S. What is the Impact of Frailty on Prescription of Anticoagulation in Elderly Patients with Atrial Fibrillation? A Systematic Review and Meta-Analysis. J. Atr. Fibrillation 2018, 10, 1870. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, C.; Wu, J.; Clegg, A.; Nadarajah, R.; Rockwood, K.; Todd, O.; Gale, C.P. Impact of oral anticoagulation on the association between frailty and clinical outcomes in people with atrial fibrillation: Nationwide primary care records on treatment analysis. Europace 2022, 24, 1065–1075. [Google Scholar] [CrossRef]
- Santos, J.; António, N.; Rocha, M.; Fortuna, A. Impact of direct oral anticoagulant off-label doses on clinical outcomes of atrial fibrillation patients: A systematic review. Br. J. Clin. Pharmacol. 2020, 86, 533–547. [Google Scholar] [CrossRef] [PubMed]
- Okumura, K.; Akao, M.; Yoshida, T.; Kawata, M.; Okazaki, O.; Akashi, S.; Eshima, K.; Tanizawa, K.; Fukuzawa, M.; Hayashi, T.; et al. Low-Dose Edoxaban in Very Elderly Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1735–1745. [Google Scholar] [CrossRef]
- Lavoie, K.; Turgeon, M.H.; Brais, C.; Larochelle, J.; Blais, L.; Farand, P.; Letemplier, G.; Perreault, S.; Beauchesne, M.F. Inappropriate dosing of direct oral anticoagulants in patients with atrial fibrillation. J. Atr. Fibrillation 2016, 9, 1478. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, R.; Jamie Nielsen, B.; Langtved Pallisgaard, J.; Ji-Young Lee, C.; Torp-Pedersen, C. Adherence with oral anticoagulation in non-valvular atrial fibrillation: A comparison of vitamin K antagonists and non-vitamin K antagonists. Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 151–156. [Google Scholar] [CrossRef]
- Simons, L.A.; Ortiz, M.; Freedman, B.; Waterhouse, B.J.; Colquhoun, D. Medium- to long-term persistence with non-vitamin-K oral anticoagulants in patients with atrial fibrillation: Australian experience. Curr. Med. Res. Opin. 2017, 33, 1337–1341. [Google Scholar] [CrossRef]
- Olimpieri, P.P.; Di Lenarda, A.; Mammarella, F.; Gozzo, L.; Cirilli, A.; Cuomo, M.; Gulizia, M.M.; Colivicchi, F.; Murri, G.; Gabrielli, D.; et al. Non-vitamin K antagonist oral anticoagulation agents in patients with atrial fibrillation: Insights from Italian monitoring registries. Int. J. Cardiol. Heart Vasc. 2020, 26, 100465. [Google Scholar] [CrossRef] [PubMed]
- Villani, E.R.; Tummolo, A.M.; Palmer, K.; Gravina, E.M.; Vetrano, D.L.; Bernabei, R.; Onder, G.; Acampora, N. Frailty and atrial fibrillation: A systematic review. Eur. J. Intern. Med. 2018, 56, 33–38. [Google Scholar] [CrossRef]
- Wilkinson, C.; Todd, O.; Clegg, A.; Gale, C.P.; Hall, M. Management of atrial fibrillation for older people with frailty: A systematic review and meta-analysis. Age Ageing 2019, 48, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Bo, M.; Li Puma, F.; Badinella Martini, M.; Falcone, Y.; Iacovino, M.; Grisoglio, E.; Menditto, E.; Fonte, G.; Brunetti, E.; Isaia, G.C.; et al. Effects of oral anticoagulant therapy in older medical in-patients with atrial fibrillation: A prospective cohort observational study. Aging Clin. Exp. Res. 2017, 29, 491–497. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Cumming, R.G.; Hilmer, S.N. The Impact of Frailty on Mortality, Length of Stay and Re-hospitalisation in Older Patients with Atrial Fibrillation. Heart Lung Circ. 2016, 25, 551–557. [Google Scholar] [CrossRef]
- Perera, V.; Bajorek, B.V.; Matthews, S.; Hilmer, S.N. The impact of frailty on the utilisation of antithrombotic therapy in older patients with atrial fibrillation. Age Ageing 2009, 38, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yang, P.-S.; Sung, J.-H.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; et al. Effectiveness and Safety of Anticoagulation Therapy in Frail Patients with Atrial Fibrillation. Stroke 2022, 53, 1873–1882. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dabigatran (n = 192) | Rivaroxaban (n = 76) | Apixaban (n = 166) | Edoxaban (n = 66) | Total | SDD | |
|---|---|---|---|---|---|---|
| Age (years) | ||||||
| Mean (SD) | 80.83 (4.50) | 80.89 (4.64) | 82.29 (4.90) | 82.02 (4.80) | 81.48 (4.73) | 0.22552 |
| 75–79 years | 93 (48.4%) | 34 (44.7%) | 59 (35.5%) | 24 (36.4%) | 210 (42.0%) | 0.26925 |
| 80–84 years | 59 (30.7%) | 23 (30.3%) | 48 (28.9%) | 22 (33.3%) | 152 (30.4%) | |
| ≥85 years | 40 (20.8%) | 19 (25.0%) | 59 (35.5%) | 20 (30.3%) | 138 (27.6%) | |
| Sex | ||||||
| Female | 77 (40.1%) | 46 (60.5%) | 94 (56.6%) | 33 (50.0%) | 250 (50.0%) | −0.32575 |
| BMI (kg/m2) | ||||||
| Mean (SD) | 28.58 (4.06) | 28.13 (4.77) | 28.32 (4.71) | 27.46 (3.88) | 28.27 (4.42) | −0.10793 |
| Smoking habit | ||||||
| Smoker | 6 (3.3%) | 1 (1.3%) | 4 (2.5%) | 1 (1.5%) | 12 (2.5%) | 0.24214 |
| Alcohol consumption | ||||||
| Abuse | 0 | 0 | 1 (0.7%) | 1 (1.7%) | 2 (0.4%) | 0.16657 |
| Creatinine clearance | ||||||
| Mean (SD) | 63.50 (18.49) | 55.42 (17.59) | 54.45 (18.65) | 53.04 (18.40) | 57.37 (18.83) | −0.49546 |
| Creatinine clearance—range | ||||||
| <15 | 0 | 0 | 0 | 0 | 0 | 0.48605 |
| 15–29 | 0 | 3 (4.2%) | 10 (6.4%) | 7 (11.1%) | 20 (4.6%) | |
| 30–59 | 72 (51.1%) | 41 (57.7%) | 92 (59.0%) | 37 (58.7%) | 242 (56.1%) | |
| 60–89 | 55 (39.0%) | 25 (35.2%) | 46 (29.5%) | 18 (28.6%) | 144 (33.4%) | |
| ≥90 | 14 (9.9%) | 2 (2.8%) | 8 (5.1%) | 1 (1.6%) | 25 (5.8%) | |
| AST (UI/L) | ||||||
| Median (Q1–Q3) | 21.0 (18.0; 28.0) | 20.5 (17.0; 25.0) | 21.0 (16.0; 29.0) | 19.0 (14.0; 24.0) | 21.0 (17.0; 27.0) | −0.04836 |
| ALT (UI/L) | ||||||
| Median (Q1–Q3) | 19.0 (13.0; 25.0) | 16.0 (13.0; 21.0) | 16.0 (12.0; 25.0) | 14.5 (11.0; 21.0) | 16.5 (12.0; 24.0) | −0.1275 |
| Total bilirubin (mg/dl) | ||||||
| Median (Q1–Q3) | 0.7 (0.5; 1.0) | 0.7 (0.4; 0.9) | 0.6 (0.5; 0.8) | 0.6 (0.5; 1.0) | 0.7 (0.5; 0.9) | −0.15063 |
| Hemoglobin (g/dl) | ||||||
| Median (Q1–Q3) | 13.1 (12.0; 14.4) | 13.1 (12.3; 14.5) | 13.1 (11.8; 14.3) | 13.4 (12.3; 14.5) | 13.2 (12.1; 14.4) | −0.06259 |
| Platelet levels (×103/μL) | ||||||
| Median (Q1–Q3) | 197.5 (156.0; 234.0) | 209.9 (176.0; 254.0) | 200.0 (160.5; 246.9) | 179.5 (151.5; 223.0) | 198.0 (160.0; 241.0) | 0.11675 |
| Dabigatran (n = 192) | Rivaroxaban (n = 76) | Apixaban (n = 166) | Edoxaban (n = 66) | Total | SDD | |
|---|---|---|---|---|---|---|
| Comorbidities | ||||||
| Heart failure | ||||||
| n (%) | 63 (32.8%) | 22 (28.9%) | 70 (42.2%) | 29 (43.9%) | 184 (36.8%) | 0.13513 |
| Hypertension | ||||||
| n (%) | 146 (76.0%) | 63 (82.9%) | 144 (86.7%) | 59 (89.4%) | 412 (82.4%) | 0.26653 |
| Coronary artery disease | ||||||
| n (%) | 35 (18.3%) | 13 (17.1%) | 21 (12.9%) | 13 (19.7%) | 82 (16.5%) | −0.0779 |
| Myocardial infarction | ||||||
| n (%) | 16 (8.3%) | 11 (14.5%) | 18 (10.9%) | 11 (16.7%) | 56 (11.2%) | 0.15248 |
| Peripheral vascular disease | ||||||
| n (%) | 20 (10.4%) | 5 (6.7%) | 15 (9.0%) | 7 (10.6%) | 47 (9.4%) | −0.05506 |
| Cerebrovascular disease | ||||||
| n (%) | 39 (20.3%) | 13 (17.1%) | 33 (19.9%) | 9 (13.6%) | 94 (18.8%) | −0.06251 |
| Dementia | ||||||
| n (%) | 4 (2.1%) | 4 (5.3%) | 13 (7.8%) | 6 (9.1%) | 27 (5.4%) | 0.25452 |
| COPD | ||||||
| n (%) | 31 (16.1%) | 10 (13.2%) | 24 (14.5%) | 12 (18.2%) | 77 (15.4%) | −0.03206 |
| Diabetes mellitus | ||||||
| Uncomplicated, n (%) | 48 (25.0%) | 18 (23.7%) | 36 (21.7%) | 11 (16.7%) | 113 (22.6%) | 0.22544 |
| End-organ damage, n (%) | 9 (4.7%) | 7 (9.2%) | 17 (10.2%) | 8 (12.1%) | 41 (8.2%) | |
| Chronic kidney disease | ||||||
| n (%) | 26 (13.5%) | 12 (15.8%) | 36 (21.7%) | 18 (27.3%) | 92 (18.4%) | 0.20877 |
| Clinical risk Scores | ||||||
| Charlson Comorbidity index score | ||||||
| Mean (SD) | 5.3 (1.7) | 5.4 (1.6) | 6.0 (2.0) | 6.3 (2.4) | 5.7 (2.0) | 0.33904 |
| CHA2DS2-VASc score | ||||||
| Mean (SD) | 4.1 (1.3) | 4.4 (1.3) | 4.6 (1.4) | 4.3 (1.3) | 4.3 (1.4) | 0.3478 |
| HAS-BLED score | ||||||
| Mean (SD) | 2.0 (0.8) | 1.6 (0.8) | 2.0 (0.9) | 2.1 (0.9) | 2.0 (0.9) | −0.07326 |
| HAS-BLED (risk of bleeding) | ||||||
| Low risk (score 0), n (%) | 0 | 0 | 0 | 0 | 0 | |
| Intermediate risk (score 1–2), n (%) | 147 (76.6%) | 64 (84.2%) | 118 (71.1%) | 48 (72.7%) | 377 (75.4%) | |
| High risk (score ≥ 3), n (%) | 45 (23.4%) | 12 (15.8%) | 48 (28.9%) | 18 (27.3%) | 123 (24.6%) | |
| Frailty (CFS scoring > 4) | 33 (17.2%) | 21 (27.6%) | 50 (30.1%) | 14 (21.2%) | 118 (23.6%) |
| Prior Thromboembolic and Bleeding Events/Treatment at the Time of the Event | Total Events | Untreated | Antiplatelets | VKA | NOAC | VKA + Antiplatelet | NOAC + Antiplatelet |
|---|---|---|---|---|---|---|---|
| Thromboembolic events, n (%) | 190 (100.0%) | 98 (51.6%) | 42 (22.1%) | 26 (13.7%) | 17 (8.9%) | 4 (2.1%) | 3 (1.6%) |
| Bleeding events, n (%) | 123 (100.0%) | 14 (11.4%) | 7 (5.7%) | 38 (30.9%) | 61 (49.6%) | 0 (0.0%) | 3 (2.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díez-Villanueva, P.; Cosín-Sales, J.; Roldán-Schilling, V.; Barrios, V.; Riba-Artés, D.; Gavín-Sebastián, O., on behalf of RE_BELD Spanish Investigator’s Group. Use of Direct Acting Oral Anticoagulants in Elderly Patients with Atrial Fibrillation: A Multicenter, Cross-Sectional Study in Spain. J. Clin. Med. 2023, 12, 1224. https://doi.org/10.3390/jcm12031224
Díez-Villanueva P, Cosín-Sales J, Roldán-Schilling V, Barrios V, Riba-Artés D, Gavín-Sebastián O on behalf of RE_BELD Spanish Investigator’s Group. Use of Direct Acting Oral Anticoagulants in Elderly Patients with Atrial Fibrillation: A Multicenter, Cross-Sectional Study in Spain. Journal of Clinical Medicine. 2023; 12(3):1224. https://doi.org/10.3390/jcm12031224
Chicago/Turabian StyleDíez-Villanueva, Pablo, Juan Cosín-Sales, Vanesa Roldán-Schilling, Vivencio Barrios, Diana Riba-Artés, and Olga Gavín-Sebastián on behalf of RE_BELD Spanish Investigator’s Group. 2023. "Use of Direct Acting Oral Anticoagulants in Elderly Patients with Atrial Fibrillation: A Multicenter, Cross-Sectional Study in Spain" Journal of Clinical Medicine 12, no. 3: 1224. https://doi.org/10.3390/jcm12031224