
An Exploratory Analysis on the 2D:4D Digit Ratio and Its Relationship with Social Responsiveness in Adults with Prader–Willi Syndrome
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sample
2.2. Procedure
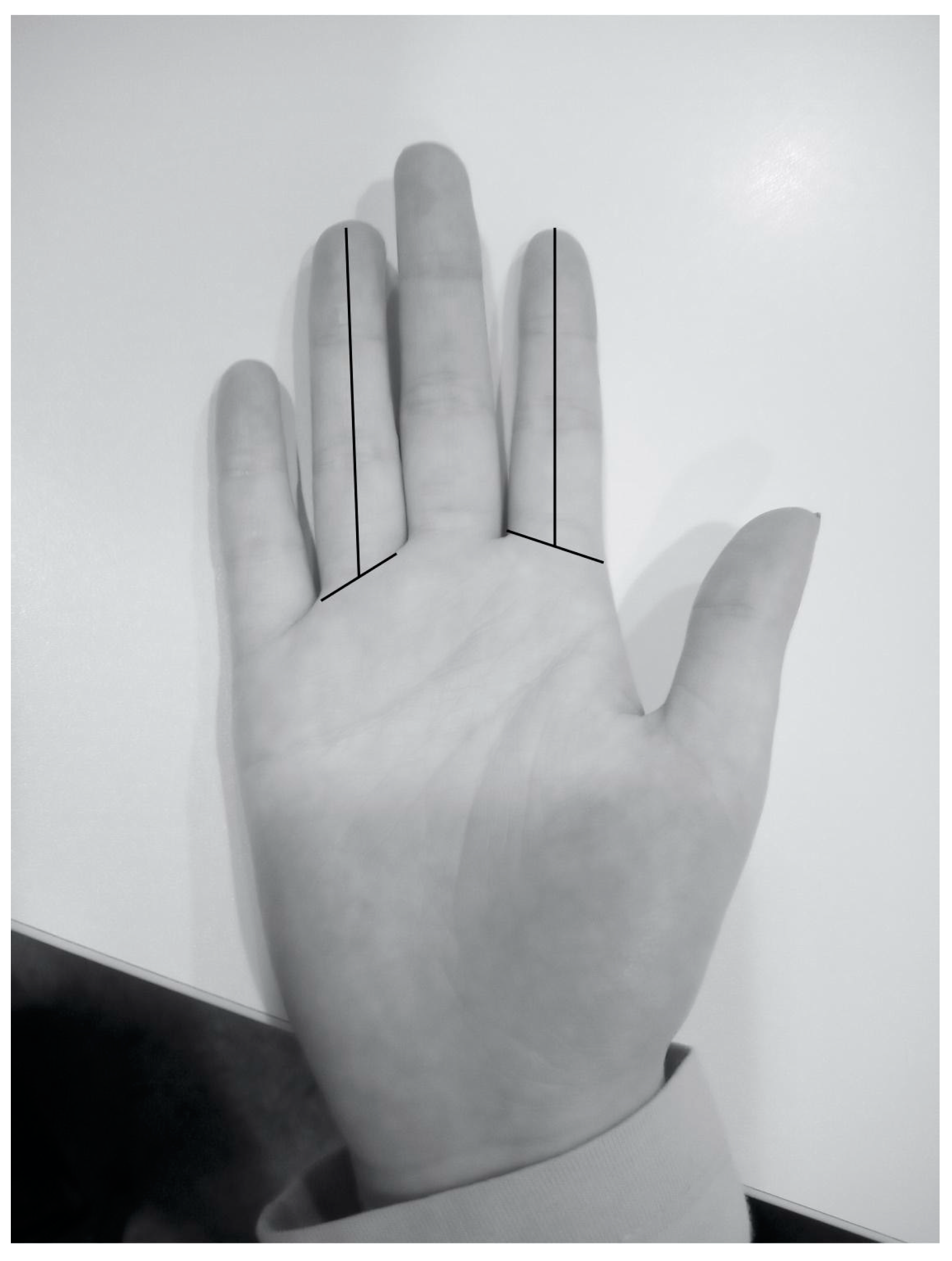
2.3. Assessment
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic, Hormonal, and Anthropometric Variables in Both Groups
3.2. Bivariate Correlation of Severity VAS, Estimated Intelligence Quotient (IQ), Behavior (SDQ), Functionality (SPS), and Social Responsiveness (SRS) in the PWS Sample
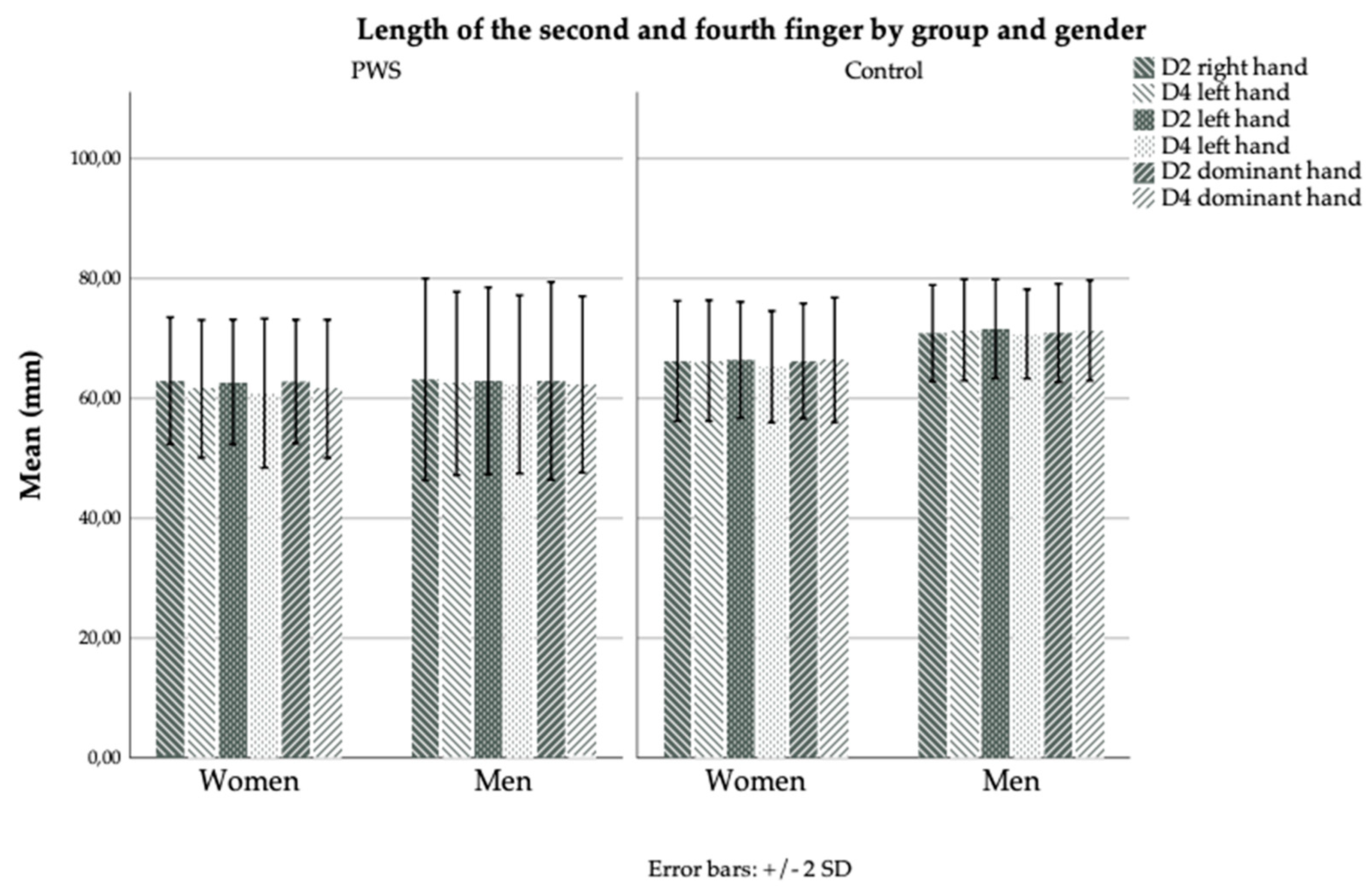
3.3. Sex Interactions in Both Samples
3.4. Relationship and SRS Sex Interactions of 2D:4D Digits on the Right Hand in the PWS Sample
3.5. Relationship and SRS Sex Interactions of 2D:4D Digit on the Left Hand in the PWS Sample
3.6. Relationship and SRS Sex Interactions of 2D:4D Digit on the Dominant Hand in the PWS Sample
3.7. Relationship between 2D or 4D Finger Lengths, 2D:4D Digit Ratios, and GH Administration during the Childhood and Adolescent Period
3.8. Relationship of GH Administration during the Childhood and Adolescent Period with Hormonal and SRS Factors
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendiola, A.J.P.; LaSalle, J.M. Epigenetics in Prader-Willi Syndrome. Front. Genet. 2021, 12, 624581. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.B.; Schwartz, S.; Miller, J.L.; Driscoll, D.J. Prader-Willi Syndrome. Genet. Med. 2012, 14, 10–26. [Google Scholar] [CrossRef] [PubMed]
- Salles, J.; Eddiry, S.; Lacassagne, E.; Laurier, V.; Molinas, C.; Bieth, É.; Franchitto, N.; Salles, J.P.; Tauber, M. Patients with PWS and Related Syndromes Display Differentially Methylated Regions Involved in Neurodevelopmental and Nutritional Trajectory. Clin. Epigenet. 2021, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A.; Germani, T.; Haqq, A.M.; Zwaigenbaum, L. Autism Spectrum Disorder in Prader-Willi Syndrome: A Systematic Review. Am. J. Med. Genet. A 2015, 167, 2936–2944. [Google Scholar] [CrossRef] [PubMed]
- Angulo, M.A.; Butler, M.G.; Cataletto, M.E. Prader-Willi Syndrome: A Review of Clinical, Genetic, and Endocrine Findings. J. Endocrinol. Invest. 2015, 38, 1249. [Google Scholar] [CrossRef] [PubMed]
- Dykens, E.M.; Roof, E. Behavior in Prader-Willi Syndrome: Relationship to Genetic Subtypes and Age. J. Child. Psychol. Psychiatry 2008, 49, 1001–1008. [Google Scholar] [CrossRef]
- Elena, G.; Bruna, C.; Benedetta, M.; Stefania, D.C.; Giuseppe, C. Prader-Willi Syndrome: Clinical Aspects. J. Obes. 2012, 2012, 13. [Google Scholar] [CrossRef]
- Guinovart, M.; Coronas, R.; Caixàs, A. Psychopathological Disorders in Prader–Willi Syndrome. Endocrinol. Diabetes Y Nutr. (Engl. Ed.) 2019, 66, 579–587. [Google Scholar] [CrossRef]
- Dimitropoulos, A.; Schultz, R.T. Autistic-like Symptomatology in Prader-Willi Syndrome: A Review of Recent Findings. Curr. Psychiatry Rep. 2007, 9, 159–164. [Google Scholar] [CrossRef]
- Dimitropoulos, A.; Ho, A.; Feldman, B. Social Responsiveness and Competence in Prader-Willi Syndrome: Direct Comparison to Autism Spectrum Disorder. J. Autism. Dev. Disord. 2012, 43, 103–113. [Google Scholar] [CrossRef]
- Milner, K.M.; Craig, E.E.; Thompson, R.J.; Veltman, M.W.M.; Simon Thomas, N.; Roberts, S.; Bellamy, M.; Curran, S.R.; Sporikou, C.M.J.; Bolton, P.F. Prader-Willi Syndrome: Intellectual Abilities and Behavioural Features by Genetic Subtype. J. Child. Psychol. Psychiatry 2005, 46, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Dykens, E.M.; Roof, E.; Hunt-Hawkins, H.; Dankner, N.; Lee, E.B.; Shivers, C.M.; Daniell, C.; Kim, S.J. Diagnoses and Characteristics of Autism Spectrum Disorders in Children with Prader-Willi Syndrome. J. Neurodev. Disord. 2017, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Veltman, M.W.M.; Craig, E.E.; Bolton, P.F. Autism Spectrum Disorders in Prader-Willi and Angelman Syndromes: A Systematic Review. Psychiatr. Genet. 2005, 15, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.K.; Godler, D.E.; Bui, M.; Hickerton, C.; Rogers, C.; Field, M.; Amor, D.J.; Bretherton, L. Exploring Autism Symptoms in an Australian Cohort of Patients with Prader-Willi and Angelman Syndromes. J. Neurodev. Disord. 2018, 10, 24. [Google Scholar] [CrossRef]
- Vorstman, J.A.S.; Staal, W.G.; van Daalen, E.; van Engeland, H.; Hochstenbach, P.F.R.; Franke, L. Identification of Novel Autism Candidate Regions through Analysis of Reported Cytogenetic Abnormalities Associated with Autism. Mol. Psychiatry 2005, 11, 18–28. [Google Scholar] [CrossRef]
- Fernández-Lafitte, M.; Cobo, J.; Coronas, R.; Parra, I.; Oliva, J.C.; Àlvarez, A.; Esteba-Castillo, S.; Giménez-Palop, O.; Palao, D.J.; Caixàs, A. Social Responsiveness and Psychosocial Functioning in Adults with Prader–Willi Syndrome. J. Clin. Med. 2022, 11, 1433. [Google Scholar] [CrossRef]
- Lutchmaya, S.; Baron-Cohen, S.; Raggatt, P.; Knickmeyer, R.; Manning, J.T. 2nd to 4th Digit Ratios, Fetal Testosterone and Estradiol. Early Hum. Dev. 2004, 77, 23–28. [Google Scholar] [CrossRef]
- Manning, J.T. Resolving the Role of Prenatal Sex Steroids in the Development of Digit Ratio. Proc. Natl. Acad. Sci. USA 2011, 108, 16143. [Google Scholar] [CrossRef]
- Manning, J.T.; Scutt, D.; Wilson, J.; Lewis-Jones, D.I. The Ratio of 2nd to 4th Digit Length: A Predictor of Sperm Numbers and Concentrations of Testosterone, Luteinizing Hormone and Oestrogen. Hum. Reprod. 1998, 13, 3000–3004. [Google Scholar] [CrossRef]
- Hönekopp, J.; Watson, S. Meta-Analysis of Digit Ratio 2D:4D Shows Greater Sex Difference in the Right Hand. Am. J. Hum. Biol. 2010, 22, 619–630. [Google Scholar] [CrossRef]
- Malas, M.A.; Dogan, S.; Hilal Evcil, E.; Desdicioglu, K. Fetal Development of the Hand, Digits and Digit Ratio (2D:4D). Early Hum. Dev. 2006, 82, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Ventura, T.; Gomes, M.C.; Pita, A.; Neto, M.T.; Taylor, A. Digit Ratio (2D:4D) in Newborns: Influences of Prenatal Testosterone and Maternal Environment. Early Hum. Dev. 2013, 89, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Knickmeyer, R.C.; Woolson, S.; Hamer, R.M.; Konneker, T.; Gilmore, J.H. 2D:4D Ratios in the First 2 Years of Life: Stability and Relation to Testosterone Exposure and Sensitivity. Horm. Behav. 2011, 60, 256. [Google Scholar] [CrossRef] [PubMed]
- Hönekopp, J. Digit Ratio 2D:4D in Relation to Autism Spectrum Disorders, Empathizing, and Systemizing: A Quantitative Review. Autism Res. 2012, 5, 221–230. [Google Scholar] [CrossRef]
- Manning, J.T.; Baron-Cohen, S.; Wheelwright, S.; Fink, B. Is Digit Ratio (2D:4D) Related to Systemizing and Empathizing? Evidence from Direct Finger Measurements Reported in the BBC Internet Survey. Pers. Individ. Differ. 2010, 48, 767–771. [Google Scholar] [CrossRef]
- Lombardo, M.V.; Auyeung, B.; Pramparo, T.; Quartier, A.; Courraud, J.; Holt, R.J.; Waldman, J.; Ruigrok, A.N.V.; Mooney, N.; Bethlehem, R.A.I.; et al. Sex-Specific Impact of Prenatal Androgens on Social Brain Default Mode Subsystems. Mol. Psychiatry 2020, 25, 2175–2188. [Google Scholar] [CrossRef]
- Butler, M.G. Prader-Willi Syndrome: Current Understanding of Cause and Diagnosis. Am. J. Med. Genet. 1990, 35, 319–332. [Google Scholar] [CrossRef]
- Hudgins, L.; Cassidy, S.B. Hand and Foot Length in Prader-Willi Syndrome. Am. J. Med. Genet. 1991, 41, 5–9. [Google Scholar] [CrossRef]
- Butler, M.G.; Meaney, F.J. An Anthropometric Study of 38 Individuals with Prader-Labhart-Willi Syndrome. Am. J. Med. Genet. 1987, 26, 445. [Google Scholar] [CrossRef]
- Moix Gil, E.; Giménez-Palop, O.; Caixàs, A. Treatment with Growth Hormone in the Prader-Willi Syndrome. Endocrinol. Diabetes Nutr. 2018, 65, 229–236. [Google Scholar] [CrossRef]
- Eiholzer, U.; Meinhardt, U.; Gallo, C.; Schlumpf, M.; Rousson, V.; l’Allemand, D. Association between Foot Growth and Musculoskeletal Loading in Children with Prader-Willi Syndrome before and during Growth Hormone Treatment. J. Pediatr. 2009, 154, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Festen, D.A.M.; de Lind Van Wijngaarden, R.; van Eekelen, M.; Otten, B.J.; Wit, J.M.; Duivenvoorden, H.J.; Hokken-Koelega, A.C.S. Randomized Controlled GH Trial: Effects on Anthropometry, Body Composition and Body Proportions in a Large Group of Children with Prader-Willi Syndrome. Clin. Endocrinol. (Oxf.) 2008, 69, 443–451. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association DSM-5. Manual Diagnóstico y Estadístico de Los Trastornos Mentales, 5th ed.; Editorial Médica Panamericana; American Psychiatric Association: Arlington, VA, USA, 2014; ISBN 978-84-9835-810-0. [Google Scholar]
- Fombonne, E.; Marcin, C.; Bruno, R.; Tinoco, C.M.; Marquez, C.D. Screening for Autism in Mexico. Autism Res. 2012, 5, 180–189. [Google Scholar] [CrossRef]
- Constantino, J.N.; Davis, S.A.; Todd, R.D.; Schindler, M.K.; Gross, M.M.; Brophy, S.L.; Metzger, L.M.; Shoushtari, C.S.; Splinter, R.; Reich, W. Validation of a Brief Quantitative Measure of Autistic Traits: Comparison of the Social Responsiveness Scale with the Autism Diagnostic Interview-Revised. J. Autism Dev. Disord. 2003, 33, 427–433. [Google Scholar] [CrossRef]
- Chan, W.; Smith, L.E.; Hong, J.; Greenberg, J.S.; Mailick, M.R. Validating the Social Responsiveness Scale for Adults with Autism. Autism Res. 2017, 10, 1663. [Google Scholar] [CrossRef]
- Bölte, S.; Poustka, F.; Constantino, J.N. Assessing Autistic Traits: Cross-Cultural Validation of the Social Responsiveness Scale (SRS). Autism Res. 2008, 1, 354–363. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child. Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Vostanis, P. Strengths and Difficulties Questionnaire: Research and Clinical Applications. Curr. Opin. Psychiatry 2006, 19, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Giannakopoulos, G.; Tzavara, C.; Dimitrakaki, C.; Kolaitis, G.; Rotsika, V.; Tountas, Y. The Factor Structure of the Strengths and Difficulties Questionnaire (SDQ) in Greek Adolescents. Ann. Gen. Psychiatry 2009, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- Fajardo Bullón, F.; León del Barco, B.; Felipe Castaño, E.; Ribeiro Dos Santos, E. Salud Mental En El Grupo de Edad 4-15 Años a Partir de Los Resultados de La Encuesta Nacional de Salud 2006. Rev. Esp. Salud Publica 2012, 86, 445–451. [Google Scholar]
- Glenn, S.; Cunningham, C.; Nananidou, A.; Prasher, V.; Glenholmes, P. Using the Strengths and Difficulties Questionnaire with Adults with Down Syndrome. Res. Dev. Disabil. 2013, 34, 3343–3351. [Google Scholar] [CrossRef] [PubMed]
- Brann, P.; Lethbridge, M.J.; Mildred, H. The Young Adult Strengths and Difficulties Questionnaire (SDQ) in Routine Clinical Practice. Psychiatry Res. 2018, 264, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Morosini, P.L.; Magliano, L.; Brambilla, L.; Ugolini, S.; Pioli, R. Development, Reliability and Acceptability of a New Version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to Assess Routine Social Funtioning. Acta Psychiatr. Scand. 2000, 101, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Portilla, M.P.; Saiz, P.A.; Bousoño, M.; Bascaran, M.T.; Guzmán-Quilo, C.; Bobes, J. Validation of the Spanish Personal and Social Performance Scale (PSP) in Outpatients with Stable and Unstable Schizophrenia. Rev. Psiquiatr. Y Salud Ment. (Engl. Ed.) 2011, 4, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Cobo, J.; Coronas, R.; Pousa, E.; Oliva, J.C.; Giménez-Palop, O.; Esteba-Castillo, S.; Novell, R.; Palao, D.J.; Caixàs, A. Multidimensional Evaluation of Awareness in Prader-Willi Syndrome. J. Clin. Med. 2021, 10, 2007. [Google Scholar] [CrossRef]
- Voracek, M.; Manning, J.T.; Dressler, S.G. Repeatability and Interobserver Error of Digit Ratio (2D:4D) Measurements Made by Experts. Am. J. Hum. Biol. 2007, 19, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Christian, C.B.; Shariff, A.F. Asymmetry and Empathy: Higher Asymmetry Is Associated with Lower Levels of Mentalizing. Early Hum. Dev. 2017, 111, 6–15. [Google Scholar] [CrossRef]
- Wu, L.; Yao, R.; Zhang, Y.; Wang, Y.; Li, T.; Chen, M.; Liu, W.; Han, H.; Bi, L.; Fu, L. The Association between Digit Ratio (2D:4D) and Overweight or Obesity among Chinese Children and Adolescents: A Cross-Sectional Study. Early Hum. Dev. 2019, 136, 14–20. [Google Scholar] [CrossRef]
- Pruszkowska-Przybylska, P.; Sitek, A.; Rosset, I.; Sobalska-Kwapis, M.; Słomka, M.; Strapagiel, D.; Żądzińska, E. Association of the 2D:4D Digit Ratio with Body Composition among the Polish Children Aged 6-13 Years. Early Hum. Dev. 2018, 124, 26–32. [Google Scholar] [CrossRef]
- Iljin, A.; Antoszewski, B.; Szewczyk, T.; Sitek, A. The 2D:4D Index Is Associated with the Development of Excess Body Weight in Adults, but Not with the Rate of Weight Loss Following Bariatric Surgery. Sci. Rep. 2022, 12, 8078. [Google Scholar] [CrossRef]
- Qian, W.; Huo, Z.; Lu, H.; Sheng, Y.; Geng, Z.; Ma, Z. Digit Ratio (2D:4D) in a Chinese Population with Schizophrenia. Early Hum. Dev. 2016, 98, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Paipa, N.; Stephan-Otto, C.; Cuevas-Esteban, J.; Núñez-Navarro, A.; Usall, J.; Brébion, G. Second-to-Fourth Digit Length Ratio Is Associated with Negative and Affective Symptoms in Schizophrenia Patients. Schizophr. Res. 2018, 199, 297–303. [Google Scholar] [CrossRef]
- Nieuwoudt, W.D.B.; Smit, I.M.; Niehaus, D.; Koen, L.; Jordaan, E. Digit Ratio as an Endophenotype in a Schizophrenia Population. S. Afr. J. Psychiatr. 2021, 27, 1587. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Rodolico, A.; Sturiale, S.; Carotenuto, B.; Natale, A.; Arillotta, D.; Siafis, S.; Signorelli, M.S.; Aguglia, E. Second-to-Fourth Digit Ratio (2D:4D) in Psychiatric Disorders: A Systematic Review of Case-Control Studies. Clin. Psychopharm. Neurosci. 2021, 19, 26–45. [Google Scholar] [CrossRef] [PubMed]
- Richards, G.; Aydin, E.; Tsompanidis, A.; Padaigaitė, E.; Austin, T.; Allison, C.; Holt, R.; Baron-Cohen, S. Digit Ratio (2D:4D) and Maternal Testosterone-to-Estradiol Ratio Measured in Early Pregnancy. Sci. Rep. 2022, 12, 13586. [Google Scholar] [CrossRef] [PubMed]
- Mian-Ling, Z.; Yun-Qi, C.; Chao-Chun, Z. Prader-Willi Syndrome: Molecular Mechanism and Epigenetic Therapy. Curr. Gene. Ther. 2020, 20, 36–43. [Google Scholar] [CrossRef]
- Richards, G.; Browne, W.V.; Constantinescu, M. Digit Ratio (2D:4D) and Amniotic Testosterone and Estradiol: An Attempted Replication of Lutchmaya et al. (2004). J. Dev. Orig. Health Dis. 2021, 12, 859–864. [Google Scholar] [CrossRef]
- Hara-Isono, K.; Matsubara, K.; Fuke, T.; Yamazawa, K.; Satou, K.; Murakami, N.; Saitoh, S.; Nakabayashi, K.; Hata, K.; Ogata, T.; et al. Genome-Wide Methylation Analysis in Silver–Russell Syndrome, Temple Syndrome, and Prader–Willi Syndrome. Clin. Epigenet. 2020, 12, 159. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PWS (n = 27) | Control (n = 36) | Statistics (X2 or U) | |
|---|---|---|---|
| Sex (male:female) | 12:15 | 12:24 | 0.808; 1; 0.262 |
| Age: m (SD); M (ITQ) | 28.5 (9.1) 24.3 (21.7–35.3) | 27.1 (8.9) 23.0 (22.0–27.5) | 458.0; 0.697 |
| IQ: m (SD); M (ITQ) | 66.5 (16.7) 63.5 (52.2–82.7) | - | - |
| Cytogenetic analysis | Type 1 deletion: 7 Type 2 deletion: 10 MUD: 6 Imprinting defects: 3 ABP2-BP4m: 1 | - | - |
| Height (m): m (SD); M (ITQ) | 1.57 (12.2) 1.56 (1.48–1.65) | 1.68 (0.1) 1.67 (1.60–1.77) | 188.0; <0.001 |
| Weight (kg): m (SD); M (ITQ) | 89.4 (22.0) 89.6 (70.5–105.5) | 64.4 (13.4) 62.0 (53.2–74.7) | 165.5; <0.001 |
| BMI (kg/m2): m (SD); M (ITQ) | 36.4 (9.0) 34.6 (30.9–41.3) | 22.5 (3.7) 21.6 (20.2–24.4) | 59.0; <0.001 |
| LH (IU/L) if receiving H-T: m (SD); M (ITQ), n = 17 | 4.41 (8.1) 1.87 (0.30–6.15) | - | - |
| LH (IU/L) if not receiving H-T: m (SD); M (ITQ), n = 10 | 4.15 (4.1) 2.44 (0.89–6.83) | - | - |
| FSH (IU/L) if receiving H-T: m (SD); M (ITQ), n = 17 | 2.84 (4.0) 0.52 (0.30–4.39) | - | - |
| FSH (IU/L): if not receiving H-T: m (SD); M (ITQ), n = 10 | 7.69 (7.5) 6.36 (2.92–9.43) | - | - |
| Testosterone, in males (ng/mL) if receiving H-T: m (SD); M (ITQ), n = 9 | 2.38 (1.9) 2.81 (0.44–3.52) | - | - |
| Testosterone, in males (ng/mL) if not receiving H-T: m (SD); M (ITQ), n = 8 | 2.18 (2.0) 1.35 (0.66–1.35) | - | - |
| Estradiol, in females (pg/mL): if receiving H-T: m (SD); M (ITQ), n = 8 | 37.25 (20.9) 32.5 (21.7–59.0) | - | - |
| Estradiol, in females (pg/mL): if not receiving H-T: m (SD); M (ITQ), n = 9 | 20.28 (13.3) 20.0 (9.0–23.0) | - | - |
| Laterality (right:left) | 18:9 | 31:5 | 3.375; 1; 0.063 |
| 2D (mm), R hand: m (SD); M (ITQ) | 63.0 (6.7) 62.0 (58.0–67.7) | 67.7 (5.1) 67.0 (64.0–71.7) | 277.0; 0.004 |
| 4D (mm), R hand: m (SD); M (ITQ) | 62.0 (6.5) 61.0 (56.0–67.0) | 68.0 (5.3) 68.0 (64.2–70.7) | 232.5; <0.001 |
| 2D:4D ratio, R hand: m (SD); M (ITQ) | 1.01 (0.04) 1.01 (1.00–1.05) | 0.99 (0.05) 1.00 (0.96–1.02) | 349.0; 0.054 |
| 2D (mm), L hand: m (SD); M (ITQ) | 62.8 (6.3) 63.0 (58.0–67.0) | 68.1 (5.1) 67.0 (64.0–72.0) | 246.5; <0.001 |
| 4D (mm), L hand: m (SD); M (ITQ) | 61.5 (6.6) 62.0 (55.0–67.0) | 67.1 (5.0) 67.5 (63.2–70.7) | 257.0; 0.001 |
| 2D:4D ratio, L hand: m (SD); M (ITQ) | 1.02 (0.05) 1.01 (0.98–1.05) | 1.01 (0.03) 1.01 (1.00–1.03) | 450.5; 0.621 |
| 2D (mm), D hand: m (SD); M (ITQ) | 62.8 (6.5) 62.0 (58.0–67.0) | 67.8 (5.0) 67.0 (64.0–72.0) | 269.5; 0.003 |
| 4D (mm), D hand: m (SD); M (ITQ) | 61.9 (6.3) 61.0 (56.0–67.0) | 68.0 (5.3) 68.0 (64.2–71.0) | 234.0; <0.001 |
| 2D:4D ratio, D hand: m (SD); M (ITQ) | 1.01 (0.04) 1.01 (0.98–1.05) | 0.99 (0.04) 1.00 (1.00–1.03) | 373.5; 0.117 |
| a. Characteristics of female participants for PWS and female healthy control groups. | |||
| PWS (n = 15) | Control (n = 24) | Statistics (X2 or U) | |
| Sex (male:female) | 0:15 | 0:24 | - |
| Age: m (SD); M (ITQ) | 24.9 (5.6) 22.9 (21.7–27.3) | 27.2 (8.9) 23.5 (22.0–28.0) | 158.0; 0.539 |
| IQ: m (SD); M (ITQ) | 71.2 (18.2) 70.0 (62.0–87.0) | - | - |
| Height (m): m (SD); M (ITQ) | 1.54 (0.1) 1.57 (1.47–1.62) | 1.63 (0.06) 1.62 (1.59–1.68) | 80.5; <0.001 |
| Weight (kg): m (SD); M (ITQ) | 86.1 (22.1) 82.0 (68.5–90.0) | 59.1 (11.6) 56.0 (49.6–62.7) | 44.0; <0.001 |
| BMI (kg/m2): m (SD); M (ITQ) | 35.9 (10.3) 33.4 (27.5–41.3) | 21.9 (4.0) 21.3 (18.8–23.8) | 18.0; <0.001 |
| Laterality (right:left) | 10:5 | 21:3 | 2.457; 1; 0.124 |
| 2D (mm), R hand: m (SD); M (ITQ) | 62.9 (5.2) 66.0 (59.0–67.0) | 66.2 (5.0) 65.5 (63.0–68.5) | 127.5; 0.128 |
| 4D (mm), R hand: m (SD); M (ITQ) | 61.6 (5.7) 63.0 (56.0–66.0) | 66.2 (5.0) 66.5 (62.2–69.7) | 102.0; 0.024 |
| 2D:4D ratio, R hand: m (SD); M (ITQ) | 1.02 (0.03) 1.01 (1.00–1.05) | 1.00 (0.05) 1.00 (0.97–1.02) | 120.0; 0.086 |
| 2D (mm), L hand: m (SD); M (ITQ) | 62.7 (5.2) 64.0 (58.0–67.0) | 66.4 (4.8) 66.0 (63.0–68.7) | 119.5; 0.080 |
| 4D (mm), L hand: m (SD); M (ITQ) | 60.8 (6.2) 62.0 (55.0–65.0) | 65.2 (4.6) 65.5 (62.0–68.0) | 108.5; 0.039 |
| 2D:4D ratio, L hand: m (SD); M (ITQ) | 1.03 (0.05) 1.03 (1.00–1.05) | 1.01 (0.04) 1.01 (1.00–1.03) | 140.5; 0.253 |
| 2D (mm), D hand: m (SD); M (ITQ) | 62.8 (5.1) 64.0 (59.0–67.0) | 66.5 (4.8) 65.5 (63.0–68.5) | 122.5; 0.095 |
| 4D (mm), D hand: m (SD); M (ITQ) | 61.6 (5.7) 63.0 (56.0–66.0) | 66.4 (5.1) 66.5 (62.5–69.7) | 102.0; 0.024 |
| 2D:4D ratio, D hand: m (SD); M (ITQ) | 1.02 (0.03) 1.01 (1.00–1.04) | 0.99 (0.04) 1.00 (0.97–1.03) | 123.5; 0.101 |
| b. Characteristics of male participants for PWS and male healthy control groups. | |||
| PWS (n = 12) | Control (n = 12) | Statistics (X2 or U) | |
| Sex (male:female) | 12:0 | 12:0 | - |
| Age: m (SD); M (ITQ) | 32.9 (10.7) 31.4 (21.9–42.0) | 27.0 (9.4) 23 (22.5–25.0) | 51.0; 0.242 |
| IQ: m (SD); M (ITQ) | 60.6 (13.2) 60.0 (49.5–70.5) | - | - |
| Height (m): m (SD); M (ITQ) | 1.60 (0.12) 1.57 (1.53–1.64) | 1.78 (0.72) 1.79 (1.72–1.83) | 15.0; 0.001 |
| Weight (kg): m (SD); M (ITQ) | 91.0 (19.6) 94.6 (80.8–100.9) | 75.0 (10.5) 72.0 (68.5–80.7) | 26.0; 0.008 |
| BMI (kg/m2): m (SD); M (ITQ) | 35.5 (7.4) 34.3 (31.4–41.2) | 23.5 (3.1) 23.0 (21.6–24.7) | 13.0; 0.001 |
| Laterality (right:left) | 8:4 | 10:2 | 0.889; 1; 0.320 |
| 2D (mm), R hand: m (SD); M (ITQ) | 63.1 (8.4) 61.0 (58.0–71.5) | 70.8 (4.0) 71.5 (67.0–75.1) | 32.0; 0.021 |
| 4D (mm), R hand: m (SD); M (ITQ) | 62.5 (7.6) 60.0 (56.5–68.7) | 71.4 (4.2) 70.5 (68.0–73.5) | 26.0; 0.008 |
| 2D:4D ratio, R hand: m (SD); M (ITQ) | 1.01 (0.04) 1.00 (0.97–1.05) | 0.99 (0.04) 0.99 (0.96–1.02) | 54.0; 0.297 |
| 2D (mm), L hand: m (SD); M (ITQ) | 62.9 (7.7) 60.5 (58.0–68.5) | 71.5 (4.1) 71.5 (67.5–72.2) | 25.0; 0.007 |
| 4D (mm), L hand: m (SD); M (ITQ) | 62.3 (7.4) 60.5 (54.7–69.0) | 70.7 (3.7) 70.0 (68.2–72.5) | 28.0; 0.011 |
| 2D:4D ratio, L hand: m (SD); M (ITQ) | 1.01 (0.05) 0.99 (0.96–1.06) | 1.01 (0.02) 1.00 (0.99–1.03) | 62.5; 0.583 |
| 2D (mm), D hand: m (SD); M (ITQ) | 62.9 (8.2) 61.0 (57.2–71.7) | 70.9 (4.1) 71.5 (67.0–74.7) | 31.5; 0.019 |
| 4D (mm), D hand: m (SD); M (ITQ) | 62.3 (7.3) 60.0 (55.0–68.7) | 71.3 (4.1) 70.5 (68.0–72.7) | 26.0; 0.008 |
| 2D:4D ratio, D hand: m (SD); M (ITQ) | 1.00 (0.05) 1.00 (0.94–1.05) | 0.99 (0.04) 0.98 (0.96–1.02) | 64.5; 0.664 |
| PWS 2D:4D Ratio, Right Hand | PWS 2D:4D Ratio, Left Hand | PWS 2D:4D Ratio, Dominant Hand | |
|---|---|---|---|
| Severity VAS (Rho; p) | 0.112; 0.577 | 0.188; 0.347 | −0.045; 0.825 |
| IQ (Rho; p) | 0.292; 0.212 | −0.016; 0.947 | 0.040; 0.867 |
| SRS Total (Rho; p) | 0.214; 0.293 | −0.142; 0.489 | −0.093; 0.653 |
| SRS Social Awareness (Rho; p) | 0.212; 0.300 | 0.066; 0.749 | 0.053; 0.798 |
| SRS Social Communication (Rho; p) | 0.207; 0.310 | −0.056; 0.785 | −0.051; 0.803 |
| SRS Social Cognition (Rho; p) | 0.270; 0.182 | −0.188; 0.359 | −0.037; 0.856 |
| SRS Social Motivation (Rho; p) | 0.035; 0.865 | −0.024; 0.906 | −0.076; 0.711 |
| SRS Restricted Interests and Repetitive Behavior (Rho; p) | 0.318; 0.113 | −0.228; 0.262 | −0.126; 0.538 |
| PWS 2D:4D Ratio, Right Hand | PWS 2D:4D Ratio, Left Hand | PWS 2D:4D Ratio, Dominant Hand | |
|---|---|---|---|
| SRS Total (Rho; p) | 0.044; 0.875 | −0.145; 0.606 | −0.355; 0.194 |
| SRS Social Awareness (Rho; p) | 0.051; 0.856 | −0.023; 0.934 | −0.249; 0.371 |
| SRS Social Communication (Rho; p) | −0.060; 0.832 | −0.170; 0.545 | −0.436; 0.104 |
| SRS Social Cognition (Rho; p) | 0.141; 0.617 | −0.363; 0.183 | −0.367; 0.179 |
| SRS Social Motivation (Rho; p) | −0.164; 0.560 | −0.067; 0.813 | −0.332; 0.227 |
| SRS Restricted Interests and Repetitive Behavior (Rho; p) | 0.134; 0.635 | −0.259; 0.352 | −0.412; 0.127 |
| PWS 2D:4D Ratio, Right Hand | PWS 2D:4D Ratio, Left Hand | PWS 2D:4D Ratio, Dominant Hand | |
|---|---|---|---|
| SRS Total (Rho; p) | 0.507; 0.112 | 0.128; 0.709 | 0.314; 0.346 |
| SRS Social Awareness (Rho; p) | 0.413; 0.207 | 0.293; 0.382 | 0.335; 0.314 |
| SRS Social Communication (Rho; p) | 0.494; 0.122 | 0.290; 0.386 | 0.433; 0.183 |
| SRS Social Cognition (Rho; p) | 0.270; 0.182 | 0.055; 0.872 | 0.330; 0.321 |
| SRS Social Motivation (Rho; p) | 0.272; 0.419 | 0.150; 0.659 | 0.260; 0.441 |
| SRS Restricted Interests and Repetitive Behaviour (Rho; p) | 0.728; 0.011 | 0.128; 0.709 | 0.226; 0.504 |
| PWS-GH (n = 14) | PWS-NoGH (n = 13) | Control (n = 36) | Statistics (U) | |
|---|---|---|---|---|
| 2D (mm), R hand: m (SD); M (ITQ) | 67.5 (5.1) 68.5 (65.5–71.5) | 58.2 (4.5) 58.0 (54.0–61.0) | 67.7 (5.1) 67.0 (64.0–71.7) | * 243.5; 0.854 ** 33.5; <0.001 *** 15.5; <0.001 |
| 4D (mm), R hand: m (SD); M (ITQ) | 65.6 (4.8) 66.0 (62.5–68.2) | 58.0 (5.9) 58.0 (53.5–60.0) | 68.0 (5.3) 68.0 (64.2–70.7) | * 181.5; 0.126 ** 51.0; <0.001 *** 27.5; 0.002 |
| 2D:4D ratio, R hand: m (SD); M (ITQ) | 1.02 (0.04) 1.03 (1.00–1.06) | 1.00 (0.04) 1.00 (0.97–1.04) | 0.99 (0.05) 1.00 (0.96–1.02) | * 140.0; 0.014 ** 209.0; 0.566 *** 60.0; 0.128 |
| 2D (mm), L hand: m (SD); M (ITQ) | 66.5 (4.0) 66.5 (63.7–67.5) | 58.7 (5.9) 58.0 (55.5–60.5) | 68.1 (5.1) 67.0 (64.0–72.0) | * 205.0; 0.308 ** 41.5; <0.001 *** 16.0; <0.001 |
| 4D (mm), L hand: m (SD); M (ITQ) | 65.2 (4.8) 64.5 (61.7–69.0) | 57.3 (6.1) 57.0 (53.0–60.5) | 67.1 (5.0) 67.5 (63.2–70.7) | * 199.5; 0.255 ** 57.5; <0.001 *** 28.5; 0.002 |
| 2D:4D ratio, L hand: m (SD); M (ITQ) | 1.02 (0.04) 1.02 (0.98–1.05) | 1.02 (0.06) 1.01 (0.96–1.07) | 1.01 (0.03) 1.01 (1.00–1.03) | * 221.5; 0.509 ** 229.0; 0.910 *** 86.5; 0.827 |
| 2D (mm), D hand: m (SD); M (ITQ) | 67.2 (4.7) 66.5 (63.5–66.5) | 58.1 (4.7) 58.0 (54.0–61.0) | 67.8 (5.0) 67.0 (64.0–72.0) | * 235.5; 0.720 ** 34.0; <0.001 *** 15.5; <0.001 |
| 4D (mm), D hand: m (SD); M (ITQ) | 65.5 (4.5) 65.5 (62.5–68.2) | 58.0 (5.9) 58.0 (53.5–60.0) | 68.0 (5.3) 68.0 (64.2–71.0) | * 182.5; 0.132 ** 51.5; <0.001 *** 26.5; 0.002 |
| 2D:4D ratio, D hand: m (SD); M (ITQ) | 1.02 (0.03) 1.03 (1.01–1.05) | 1.00 (0.05) 1.00 (0.95–1.04) | 0.99 (0.04) 1.00 (1.00–1.03) | * 142.0; 0.017 ** 231.5; 0.955 *** 64.5; 0.198 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gámez, S.; Cobo, J.; Fernández-Lafitte, M.; Coronas, R.; Parra, I.; Oliva, J.C.; Àlvarez, A.; Esteba-Castillo, S.; Giménez-Palop, O.; Corripio, R.; et al. An Exploratory Analysis on the 2D:4D Digit Ratio and Its Relationship with Social Responsiveness in Adults with Prader–Willi Syndrome. J. Clin. Med. 2023, 12, 1155. https://doi.org/10.3390/jcm12031155
Gámez S, Cobo J, Fernández-Lafitte M, Coronas R, Parra I, Oliva JC, Àlvarez A, Esteba-Castillo S, Giménez-Palop O, Corripio R, et al. An Exploratory Analysis on the 2D:4D Digit Ratio and Its Relationship with Social Responsiveness in Adults with Prader–Willi Syndrome. Journal of Clinical Medicine. 2023; 12(3):1155. https://doi.org/10.3390/jcm12031155
Chicago/Turabian StyleGámez, Sara, Jesus Cobo, Meritxell Fernández-Lafitte, Ramón Coronas, Isabel Parra, Joan Carles Oliva, Aida Àlvarez, Susanna Esteba-Castillo, Olga Giménez-Palop, Raquel Corripio, and et al. 2023. "An Exploratory Analysis on the 2D:4D Digit Ratio and Its Relationship with Social Responsiveness in Adults with Prader–Willi Syndrome" Journal of Clinical Medicine 12, no. 3: 1155. https://doi.org/10.3390/jcm12031155