Left Atrial Functional Remodeling in Patients with Chronic Heart Failure Treated with Sacubitril/Valsartan

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Echocardiography
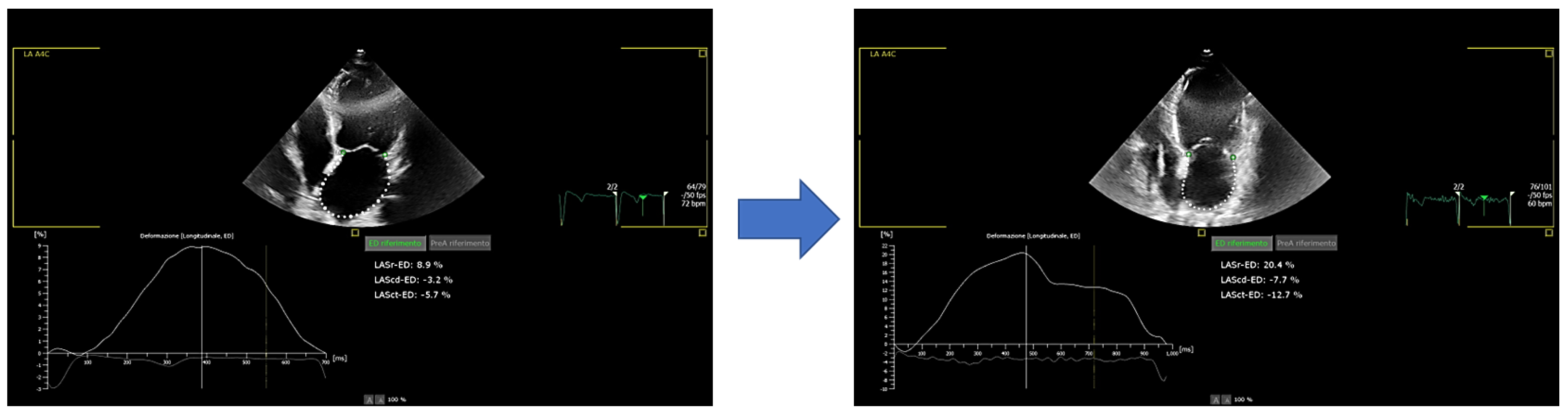
2.2. Speckle-Tracking Strain Analysis for Assessment Left Atrial Function
2.3. Statistical Analysis
3. Results
3.1. Conventional Echo Parameters
3.2. Two-Dimensional Speckle Tracking Echocardiography (2D-STE) Parameters
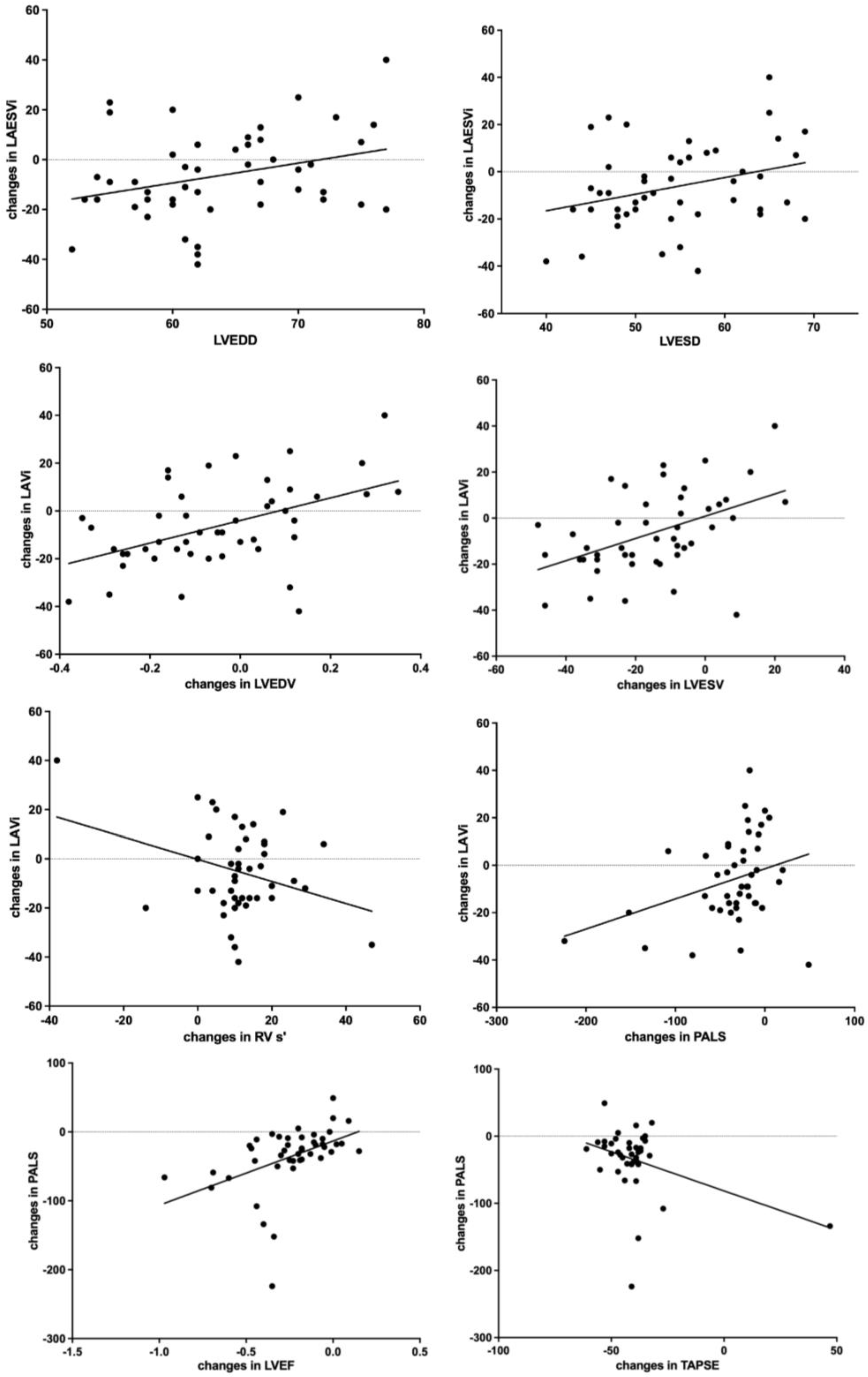
3.3. Correlations
- (i)
- (ii)
- (iii)
- (iv)
- changes in LVESV, (r = 0.46, p = 0.001);
- (v)
- (vi)
- changes in right ventricle tissue Doppler imaging s’ wave (RV TDI s’; r = −0.32, p = 0.04) (Figure 1);

3.4. LARR+ vs. LARR− Comparison
4. Discussion
- Significant improvement of LA dimensions and function already after just six months of therapy with S/V;
- Significant correlations between changes in LA volumes (LAVi) and LV dimensions (basal LVEDD, basal LVESD; changes in LVEDV, changes in LVESV), LA function (PALS) and RV function (changes in RV TDI S’);
- Changes in LA function (PALS) proportional to changes in LV (LVEF) and RV function (TAPSE);
- Larger PALS changes and larger LA baseline volumes in the LARR+ group compared with LARR- group;
- Changes at multivariable analysis in the LA dimension (LAVi) proportional to changes in LVEDV and PALS.
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, J.A.; Olson, E.N. Cardiac plasticity. N. Engl. J. Med. 2008, 358, 1370–1380. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Pitt, B.; Davis, C.E.; Hood, W.B.; Cohn, J.N. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N. Engl. J. Med. 1991, 325, 293–302. [Google Scholar] [PubMed]
- Cohn, J.N.; Tognoni, G.; Valsartan Heart Failure Trial, I. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N. Engl. J. Med. 2001, 345, 1667–1675. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Investigators P-H and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Martens, P.; Belien, H.; Dupont, M.; Vandervoort, P.; Mullens, W. The reverse remodeling response to sacubitril/valsartan therapy in heart failure with reduced ejection fraction. Cardiovasc. Ther. 2018, 36, e12435. [Google Scholar] [CrossRef] [Green Version]
- Almufleh, A.; Marbach, J.; Chih, S.; Stadnick, E.; Davies, R.; Liu, P.; Mielniczuk, L. Ejection fraction improvement and reverse remodeling achieved with Sacubitril/Valsartan in heart failure with reduced ejection fraction patients. Am. J. Cardiovasc. Dis. 2017, 7, 108–113. [Google Scholar]
- Gandjour, A.; Ostwald, D.A. Sacubitril/Valsartan (LCZ696): A Novel Treatment for Heart Failure and its Estimated Cost Effectiveness, Budget Impact, and Disease Burden Reduction in Germany. Pharmacoeconomics 2018, 36, 1285–1296. [Google Scholar] [CrossRef]
- Correale, M.; Monaco, I.; Ferraretti, A.; Tricarico, L.; Padovano, G.; Formica, E.S.; Tozzi, V.; Grazioli, D.; Di Biase, M.; Brunetti, N.D. Hospitalization cost reduction with sacubitril-valsartan implementation in a cohort of patients from the Daunia Heart Failure Registry. Int. J. Cardiol. Heart Vasc. 2019, 22, 102–104. [Google Scholar] [CrossRef]
- Sutanto, H.; Dobrev, D.; Heijman, J. Angiotensin Receptor-Neprilysin Inhibitor (ARNI) and Cardiac Arrhythmias. Int. J. Mol. Sci. 2021, 22, 8994. [Google Scholar] [CrossRef]
- Fernandes, A.D.F.; Fernandes, G.C.; Ternes, C.M.P.; Cardoso, R.; Chaparro, S.V.; Goldberger, J.J. Sacubitril/valsartan versus angiotensin inhibitors and arrhythmia endpoints in heart failure with reduced ejection fraction. Heart Rhythm 2021, 2, 724–732. [Google Scholar] [CrossRef]
- Casale, M.; Correale, M.; Laterra, G.; Vaccaro, V.; Morabito, C.; Crea, P.; Signorelli, S.S.; Katsiki, N.; Luzza, F.; de Gregorio, C.; et al. Effects of Sacubitril/Valsartan in Patients with High Arrhythmic Risk and an ICD: A Longitudinal Study. Clin. Drug Investig. 2021, 41, 169–176. [Google Scholar] [CrossRef]
- Rohde, L.E.; Chatterjee, N.A.; Vaduganathan, M.; Claggett, B.; Packer, M.; Desai, A.S.; Zile, M.; Rouleau, J.; Swedberg, K.; Lefkowitz, M.; et al. Sacubitril/Valsartan and Sudden Cardiac Death According to Implantable Cardioverter-Defibrillator Use and Heart Failure Cause: A PARADIGM-HF Analysis. Heart Fail. 2020, 8, 844–855. [Google Scholar] [CrossRef]
- Díez, J. Chronic heart failure as a state of reduced effectiveness of the natriuretic peptide system: Implications for therapy. Eur. J. Heart Fail. 2017, 19, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Abumayyaleh, M.; El-Battrawy, I.; Behnes, M.; Borggrefe, M.; Akin, I. Current evidence of sacubitril/valsartan in the treatment of heart failure with reduced ejection fraction. Future Cardiol. 2020, 16, 227–236. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Borggrefe, M.; Akin, I. The Risk for Sudden Cardiac Death and Effect of Treatment with Sacubitril/Valsartan in Heart Failure. Heart Fail. 2019, 7, 999. [Google Scholar] [CrossRef]
- Abumayyaleh, M.; El-Battrawy, I.; Kummer, M.; Pilsinger, C.; Sattler, K.; Kuschyk, J.; Aweimer, A.; Mügge, A.; Borggrefe, M.; Akin, I. Comparison of the prognosis and outcome of heart failure with reduced ejection fraction patients treated with sacubitril/valsartan according to age. Future Cardiol. 2021, 17, 1131–1142. [Google Scholar] [CrossRef]
- Ersboll, M.; Moller, J.E. Left Atrial Function in Heart Failure with Reduced Ejection Fraction. Circ. Cardiovasc. Imaging 2018, 11, e008427. [Google Scholar] [CrossRef]
- Zhu, N.; Chen, H.; Zhao, X.; Ye, F.; Jiang, W.; Wang, Y. Left atrial diameter in heart failure with left ventricular preserved, mid-range, and reduced ejection fraction. Medicine 2019, 98, e18146. [Google Scholar] [CrossRef]
- Donal, E.; Tan, K.; Leclercq, C.; Ollivier, R.; Derumeaux, G.; Bernard, M.; de Place, C.; Mabo, P.; Daubert, J.C. Left atrial reverse remodeling and cardiac resynchronization therapy for chronic heart failure patients in sinus rhythm. J. Am. Soc. Echocardiogr. 2009, 22, 1152–1158. [Google Scholar] [CrossRef]
- Thomas, L.; Abhayaratna, W.P. Left Atrial Reverse Remodeling: Mechanisms, Evaluation, and Clinical Significance. Cardiovasc. Imaging 2017, 10, 65–77. [Google Scholar]
- Gan, G.C.H.; Ferkh, A.; Boyd, A.; Thomas, L. Left atrial function: Evaluation by strain analysis. Cardiovasc. Diagn. Ther. 2018, 8, 29–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correale, M.; Totaro, A.; Greco, C.A.; Musaico, F.; De Rosa, F.; Ferraretti, A.; Ieva, R.; Di Biase, M.; Brunetti, N.D. Tissue Doppler time intervals predict the occurrence of rehospitalization in chronic heart failure: Data from the daunia heart failure registry. Echocardiography 2012, 29, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Correale, M.; Brunetti, N.D.; Totaro, A.; Montrone, D.; Russo, A.R.; Fanigliulo, A.M.; Ieva, R.; Di Biase, M. Statin therapy blunts inflammatory activation and improves prognosis and left ventricular performance assessed by Tissue Doppler Imaging in subjects with chronic ischemic heart failure: Results from the Daunia Heart Failure Registry. Clinics 2011, 66, 777–784. [Google Scholar] [PubMed]
- Correale, M.; Totaro, A.; Ferraretti, A.; Musaico, F.; Passero, T.; De Rosa, F.; Abruzzese, S.; Ieva, R.; Di Biase, M.; Brunetti, N.D. Additional Prognostic Value of EAS index in predicting the occurrence of rehospitalizations in chronic heart failure: Data from the Daunia Heart Failure Registry. Eur. J. Clin. Investig. 2015, 45, 1098–1105. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Castrichini, M.; Manca, P.; Nuzzi, V.; Barbati, G.; De Luca, A.; Korcova, R.; Stolfo, D.; Lenarda, A.D.; Merlo, M.; Sinagra, G. Sacubitril/Valsartan Induces Global Cardiac Reverse Remodeling in Long-Lasting Heart Failure with Reduced Ejection Fraction: Standard and Advanced Echocardiographic Evidences. J. Clin. Med. 2020, 9, 906. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Industry r and Reviewers: This document was reviewed by members of the ESDC. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar]
- Moon, M.G.; Hwang, I.C.; Lee, H.J.; Kim, S.H.; Yoon, Y.E.; Park, J.B.; Lee, S.P.; Kim, H.K.; Kim, Y.J.; Cho, G.Y. Reverse Remodeling Assessed by Left Atrial and Ventricular Strain Reflects Treatment Response to Sacubitril/Valsartan. Cardiovasc. Imaging 2022, 15, 1525–1541. [Google Scholar] [CrossRef]
- Sun, Y.; Song, S.; Zhang, Y.; Mo, W.; Zhang, X.; Wang, N.; Xia, Y.; Tse, G.; Liu, Y. Effect of angiotensin receptor neprilysin inhibitors on left atrial remodeling and prognosis in heart failure. ESC Heart Fail. 2022, 9, 667–675. [Google Scholar] [CrossRef]
- Ersboll, M.; Andersen, M.J.; Valeur, N.; Mogensen, U.M.; Waziri, H.; Moller, J.E.; Hassager, C.; Sogaard, P.; Kober, L. The prognostic value of left atrial peak reservoir strain in acute myocardial infarction is dependent on left ventricular longitudinal function and left atrial size. Circ. Cardiovasc. Imaging 2013, 6, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Carluccio, E.; Biagioli, P.; Mengoni, A.; Cerasa, M.F.; Lauciello, R.; Zuchi, C.; Bardelli, G.; Alunni, G.; Coiro, S.; Gronda, E.G.; et al. Left Atrial Reservoir Function and Outcome in Heart Failure with Reduced Ejection Fraction. Circ. Cardiovasc. Imaging 2018, 11, e007696. [Google Scholar] [CrossRef]
- Correale, M.; Mallardi, A.; Mazzeo, P.; Tricarico, L.; Diella, C.; Romano, V.; Ferraretti, A.; Leopizzi, A.; Merolla, G.; Di Biase, M.; et al. Sacubitril/valsartan improves right ventricular function in a real-life population of patients with chronic heart failure: The Daunia Heart Failure Registry. Int. J. Cardiol. Heart Vasc. 2020, 27, 100486. [Google Scholar] [CrossRef]
- Candan, O.; Ozdemir, N.; Aung, S.M.; Hatipoglu, S.; Karabay, C.Y.; Guler, A.; Gecmen, C.; Dogan, C.; Omaygenc, O.; Bakal, R.B. Atrial longitudinal strain parameters predict left atrial reverse remodeling after mitral valve surgery: A speckle tracking echocardiography study. Int. J. Cardiovasc. Imaging 2014, 30, 1049–1056. [Google Scholar] [CrossRef]
- Landolfo, M.; Piani, F.; Esposti, D.D.; Cosentino, E.; Bacchelli, S.; Dormi, A.; Borghi, C. Effects of sacubitril valsartan on clinical and echocardiographic parameters of outpatients with heart failure and reduced ejection fraction. Int. J. Cardiol. Heart Vasc. 2020, 31, 100656. [Google Scholar] [CrossRef]
- De Vecchis, R.; Paccone, A.; Di Maio, M. Favorable Effects of Sacubitril/Valsartan on the Peak Atrial Longitudinal Strain in Patients with Chronic Heart Failure and a History of One or More Episodes of Atrial Fibrillation: A Retrospective Cohort Study. J. Clin. Med. Res. 2020, 12, 100–107. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Baseline | Follow Up | ||
|---|---|---|---|
| Mean ± SD or % | Mean ± SD or % | p-Value | |
| Patients, # | 47 | 47 | |
| Male gender, % | 85 | ||
| Age, years | 66 ± 8 | ||
| BSA, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | |
| Hypertension, % | 85 | 85 | |
| Diabetes, % | 36 | 36 | |
| Dyslipidemia, % | 70 | 70 | |
| Ischaemic etiology, % | 43 | 43 | |
| Atrial Fibrillation, % | 51% | 51% | |
| ICD/CRT-D, %/% | 36/15 | 36/15 | |
| NYHA class I, % | 0 | 4 | 0.153 |
| NYHA class II, % | 64 | 79 | 0.107 |
| NYHA class III, % | 36 | 17 | 0.037 |
| NYHA class IV, % | 0 | 0 | |
| SBP, mmHg | 121 ± 17 | 116 ± 18 | 0.01 |
| DBP, mmHg | 71 ± 10 | 69 ± 10 | 0.163 |
| HR, bpm | 70 ± 13 | 69 ± 12 | 0.645 |
| NT-proBNP, mg/dL | 1086 ± 1116 | 399 ± 325 | <0.001 |
| Hb, g/dL | 13 ± 1 | 13 ± 1 | 0.634 |
| eGFR, mL/min/1.73 m2 | 71 ± 23 | 68 ± 24 | 0.103 |
| Potassium, mEq/L | 4.3 ± 0.2 | 4.5 ± 0.3 | 0.006 |
| ACE-i, % | 70 | 70 | |
| ARBs, % | 30 | 30 | |
| Ivabradine, % | 19 | 19 | |
| MRAs, % | 62 | 62 | |
| Beta-blockers, % | 98 | 98 |
| Baseline | Follow Up | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| LVEDDi, mm/m2 | 34.4 ± 5.0 | 33.7 ± 4.6 | 0.002 |
| LVESDi, mm/m2 | 29.4 ± 5.1 | 28.1 ± 5.1 | <0.001 |
| LVEDVi, mL/m2 | 105 ± 34 | 99 ± 38 | 0.07 |
| LVESVi, mL/m2 | 76 ± 28 | 65 ± 29 | <0.001 |
| LVEF, % | 28 ± 6 | 36 ± 7 | <0.001 |
| LA area, cm2 | 24.7 ± 5.4 | 23.8 ± 5.6 | 0.02 |
| LAVi, mL/m2 | 45 ± 15 | 42 ± 15 | 0.008 |
| E/e’ ratio | 16 ± 6 | 13 ± 6 | <0.001 |
| RAESA, cm2 | 20 ± 6 | 19 ± 6 | 0.219 |
| PAsP | 35 ± 9 | 31 ± 11 | 0.001 |
| RVEDD, mm | 38 ± 5 | 37 ± 5 | 0.026 |
| TAPSE, mm | 18 ± 3 | 20 ± 3 | <0.001 |
| RV TDI s’, cm/s | 11 ± 2 | 12 ± 2 | <0.001 |
| RV FAC, cm2 | 34 ± 6 | 39 ± 6 | <0.001 |
| Baseline | Follow Up | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| LAEF, % | 37 ± 11 | 46 ± 13 | <0.001 |
| PALS, % | 15 ± 7 | 19 ± 8 | <0.001 |
| LA Conduit, % | (−7.6) ± 4.1 | (−9.7) ± 5.2 | 0.007 |
| PACS, % | 8.7 ± 6 | 10.6 ± 6.5 | 0.051 |
| LARR+ (N = 17) | LARR− (N = 30) | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Male gender, % | 82 | 87 | 0.697 |
| Age, years | 66 ± 10 | 67 ± 7 | 0.722 |
| BSA, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 0.92 |
| Hypertension, % | 82 | 87 | 0.697 |
| Diabetes, % | 29 | 40 | 0.479 |
| Dyslipidemia, % | 65 | 73 | 0.545 |
| Ischaemic etiology, % | 35 | 47 | 0.46 |
| Atrial fibrillation, % | 35 | 67 | 0.108 |
| ICD/CRT-D, %/% | 29/12 | 40/17 | |
| NYHA I, % | 0 | 0 | |
| NYHA II, % | 59 | 67 | 0.583 |
| NYHA III, % | 41 | 33 | 0.583 |
| NYHA IV, % | 0 | 0 | |
| SBP, mmHg | 129 ± 21 | 117 ± 12 | 0.012 |
| DBP, mmHg | 74 ± 12 | 70 ± 9 | 0.226 |
| HR, bpm | 68 ± 11 | 71 ± 14 | 0.462 |
| NT-proBNP, mg/dL a | 800(850) | 800(1170) | 0.631 |
| LVEDVi, mL/m2 | 98 ± 27 | 109 ± 38 | 0.324 |
| LVESVi, mL/m2 | 69 ± 21 | 80 ± 31 | 0.223 |
| LVEF, % | 30 ± 6 | 27 ± 5 | 0.148 |
| LAVi, mL/m2 | 44 ± 17 | 46 ± 15 | 0.734 |
| LAEF, % | 40 ± 9 | 35 ± 11 | 0.143 |
| PALS, % | 14 ± 8 | 15 ± 7 | 0.872 |
| E/e’ ratio | 15 ± 7 | 16 ± 6 | 0.882 |
| RA ESA, cm2 | 19 ± 3 | 20 ± 7 | 0.511 |
| PAPs, mmHg | 33 ± 9 | 36 ± 9 | 0.381 |
| RVEDD, mm | 39 ± 5 | 37 ± 5 | 0.362 |
| TAPSE, mm | 19 ± 3 | 18 ± 3 | 0.125 |
| RV TDI s’, cm/s | 11 ± 2 | 10 ± 2 | 0.078 |
| RV FAC, cm2 | 37 ± 5 | 33 ± 6 | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correale, M.; Magnesa, M.; Mazzeo, P.; Fortunato, M.; Tricarico, L.; Leopizzi, A.; Mallardi, A.; Mennella, R.; Croella, F.; Iacoviello, M.; et al. Left Atrial Functional Remodeling in Patients with Chronic Heart Failure Treated with Sacubitril/Valsartan. J. Clin. Med. 2023, 12, 1086. https://doi.org/10.3390/jcm12031086
Correale M, Magnesa M, Mazzeo P, Fortunato M, Tricarico L, Leopizzi A, Mallardi A, Mennella R, Croella F, Iacoviello M, et al. Left Atrial Functional Remodeling in Patients with Chronic Heart Failure Treated with Sacubitril/Valsartan. Journal of Clinical Medicine. 2023; 12(3):1086. https://doi.org/10.3390/jcm12031086
Chicago/Turabian StyleCorreale, Michele, Michele Magnesa, Pietro Mazzeo, Martino Fortunato, Lucia Tricarico, Alessandra Leopizzi, Adriana Mallardi, Raffaele Mennella, Francesca Croella, Massimo Iacoviello, and et al. 2023. "Left Atrial Functional Remodeling in Patients with Chronic Heart Failure Treated with Sacubitril/Valsartan" Journal of Clinical Medicine 12, no. 3: 1086. https://doi.org/10.3390/jcm12031086