
Real-World Use of Alirocumab: Experience from a Large Healthcare Provider

Abstract
:1. Introduction
2. Material and Methods
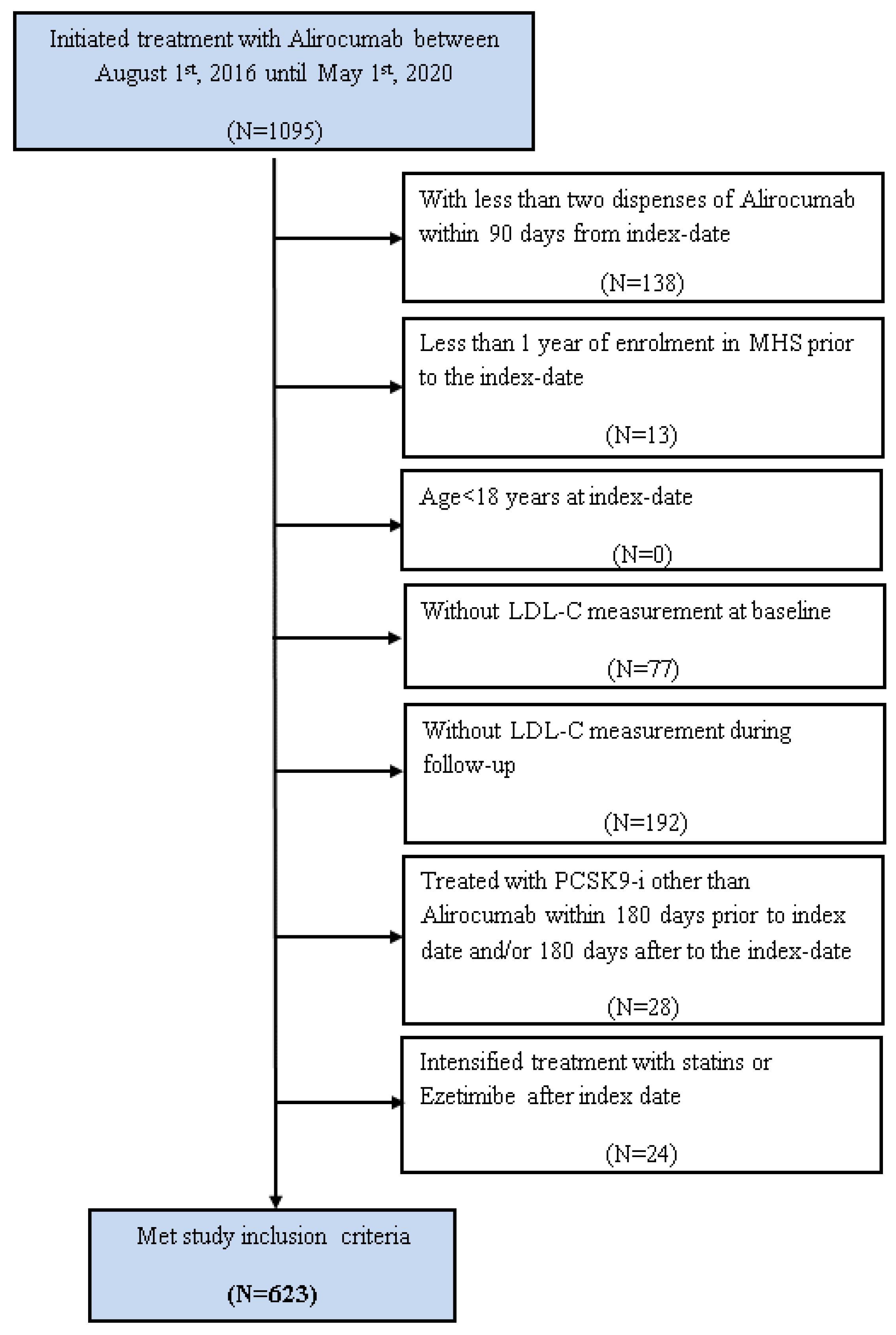
2.1. Study Population and Design
2.2. Study Variables
2.3. Statistical Analysis
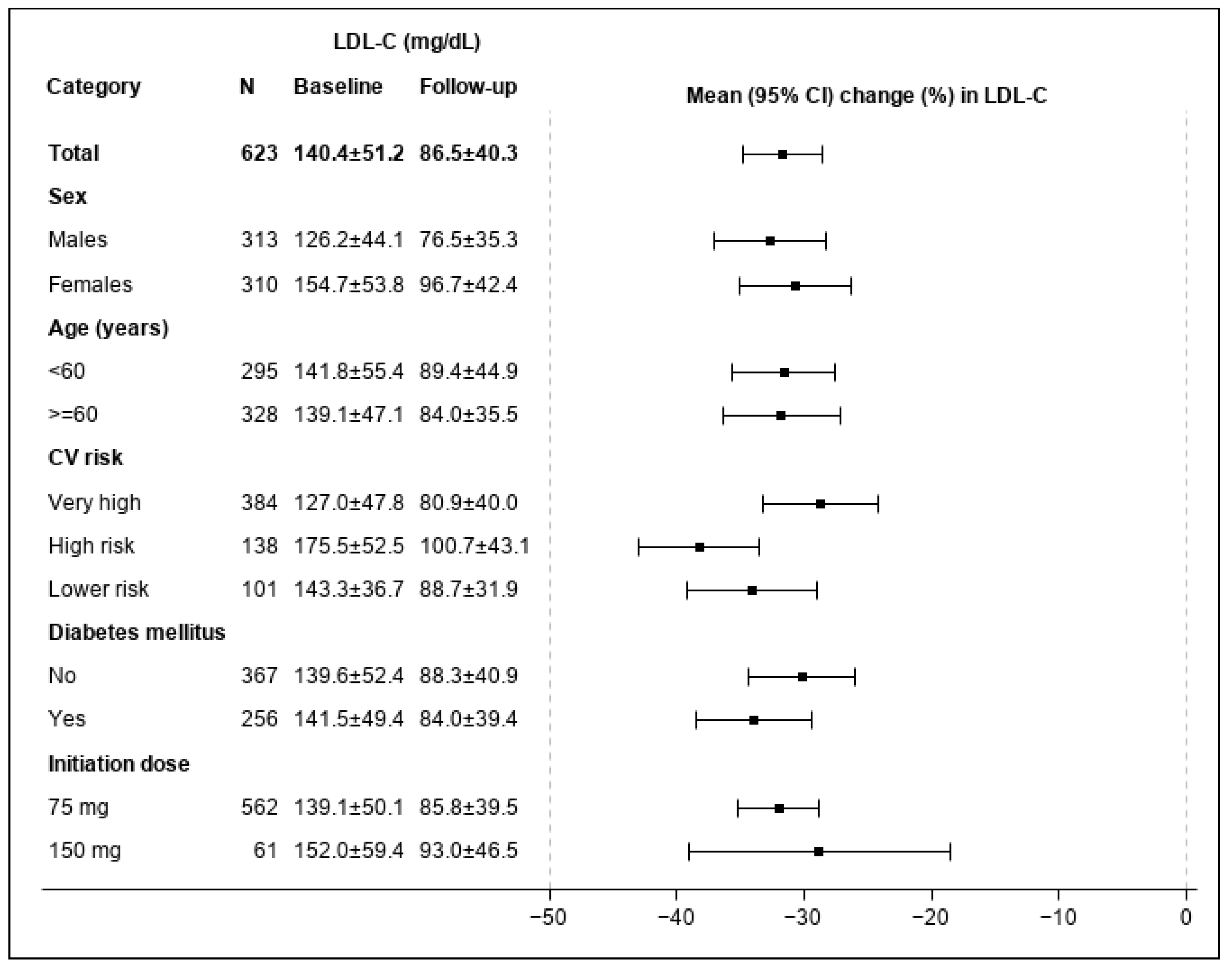
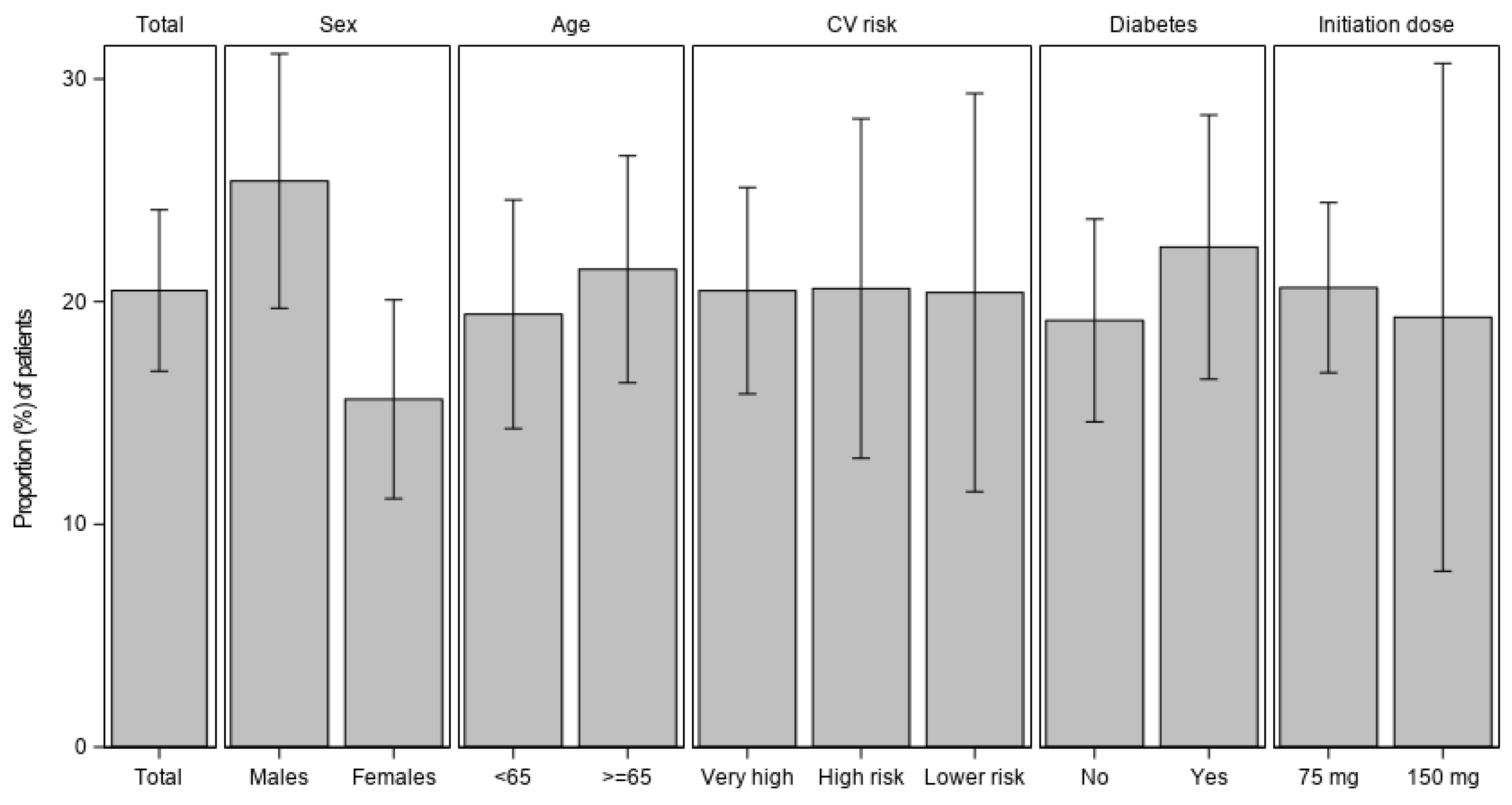
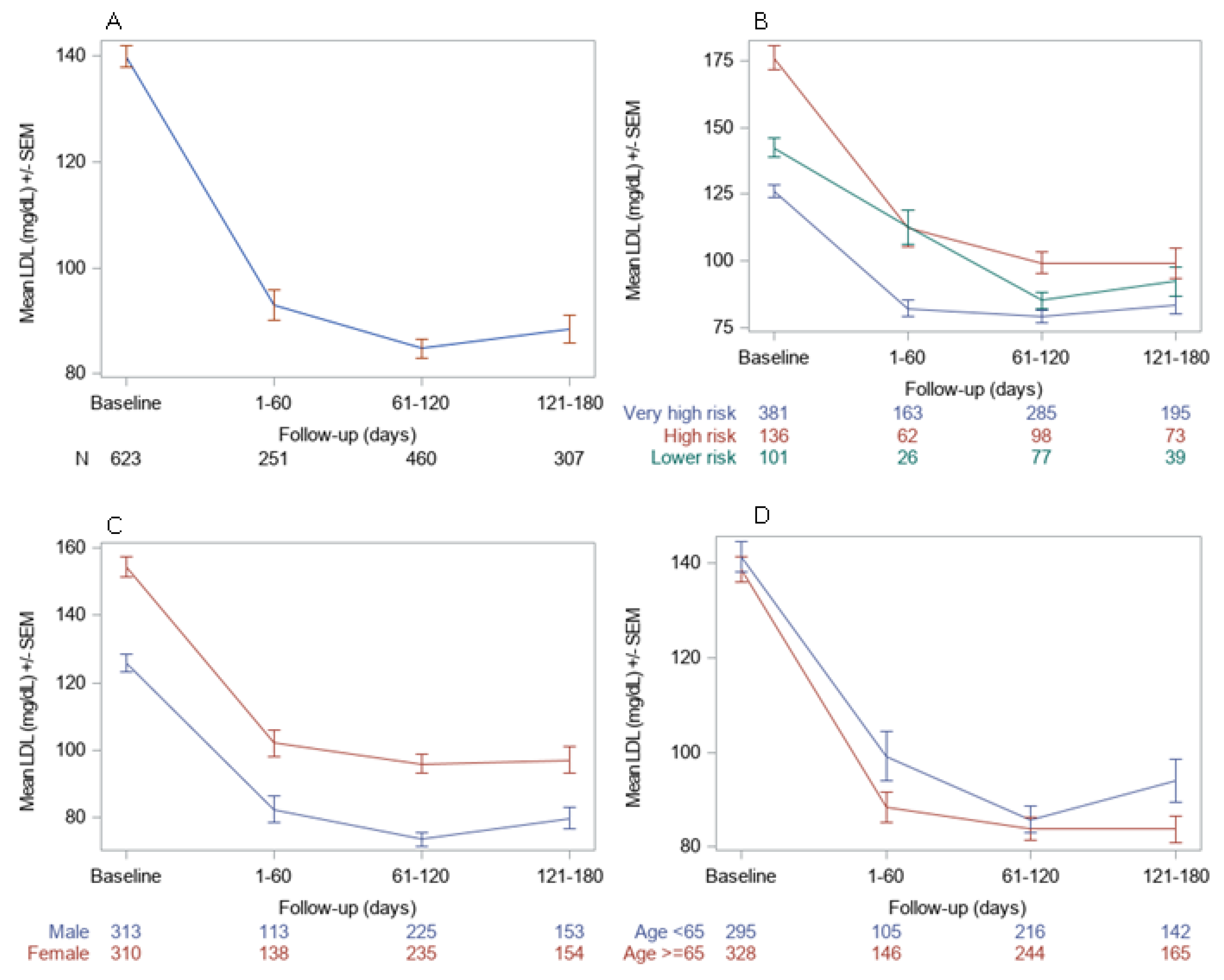
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wadhera, R.K.; Steen, D.L.; Khan, I.; Giugliano, R.P.; Foody, J.M. A review of low-density lipoprotein cholesterol, treatment strategies, and its impact on cardiovascular disease morbidity and mortality. J. Clin. Lipidol. 2016, 10, 472–489. [Google Scholar] [CrossRef] [Green Version]
- Catapano, A.L.; Reiner, Ž.; De Backer, G.; Graham, I.; Taskinen, M.-R.; Wiklund, O.; Agewall, S.; Alegria, E.; Chapman, M.J.; Durrington, P. ESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Atherosclerosis 2011, 217, 3–46. [Google Scholar] [CrossRef] [PubMed]
- Annemans, L.; Packard, C.J.; Briggs, A.; Ray, K.K. ’Highest risk-highest benefit’ strategy: A pragmatic, cost-effective approach to targeting use of PCSK9 inhibitor therapies. Eur. Heart J. 2018, 39, 2546–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, E.J.; Schiffman, F.J. Cecil Essentials of Medicine E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef]
- Sabatine, M.; Giugliano, R.; Wiviott, S.; Raal, F.; Blom, D.; Robinson, J.; Ballantyne, C.; Somaratne, R.; Legg, J.; Wasserman, S. Open-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER) Investigators. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1500–1509. [Google Scholar] [CrossRef] [Green Version]
- Preiss, D.; Tobert, J.A.; Hovingh, G.K.; Reith, C. Lipid-Modifying Agents, From Statins to PCSK9 Inhibitors. J. Am. Coll. Cardiol. 2020, 75, 1945–1955. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Landmesser, U.; Chapman, M.J.; Stock, J.K.; Amarenco, P.; Belch, J.J.F.; Borén, J.; Farnier, M.; Ference, B.A.; Gielen, S.; Graham, I.; et al. 2017 Update of ESC/EAS Task Force on practical clinical guidance for proprotein convertase subtilisin/kexin type 9 inhibition in patients with atherosclerotic cardiovascular disease or in familial hypercholesterolaemia. Eur. Heart J. 2018, 39, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [Green Version]
- Mulder, J.; Steward, K.; Galema-Boers, A.; Boersma, E.; Van Lennep, J.R. Efficacy & safety of PCSK9-inhibitors: A systematic review and meta-analysis of real-world data. Atherosclerosis 2022, 355, 15. [Google Scholar]
- Dicembrini, I.; Giannini, S.; Ragghianti, B.; Mannucci, E.; Monami, M. Effects of PCSK9 inhibitors on LDL cholesterol, cardiovascular morbidity and all-cause mortality: A systematic review and meta-analysis of randomized controlled trials. J. Endocrinol. Investig. 2019, 42, 1029–1039. [Google Scholar] [CrossRef]
- Shalev, V.; Chodick, G.; Goren, I.; Silber, H.; Kokia, E.; Heymann, A.D. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int. J. Cardiol. 2011, 152, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Zafrir, B.; Jubran, A. Lipid-lowering therapy with PCSK9-inhibitors in the real-world setting: Two-year experience of a regional lipid clinic. Cardiovasc. Ther. 2018, 36, e12439. [Google Scholar] [CrossRef]
- Stoekenbroek, R.M.; Hartgers, M.L.; Rutte, R.; de Wijer, D.D.; Stroes, E.S.G.; Hovingh, G.K. PCSK9 inhibitors in clinical practice: Delivering on the promise? Atherosclerosis 2018, 270, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, T.M.; Warden, B.A.; Minnier, J.; Miles, J.R.; Duell, P.B.; Purnell, J.Q.; Wojcik, C.; Fazio, S.; Shapiro, M.D. Application of PCSK9 Inhibitors in Practice. Circ. Res. 2019, 124, 32–37. [Google Scholar] [CrossRef]
- Bradley, C.K.; Shrader, P.; Sanchez, R.J.; Peterson, E.D.; Navar, A.M. The patient journey with proprotein convertase subtilisin/kexin type 9 inhibitors in community practice. J. Clin. Lipidol. 2019, 13, 725–734. [Google Scholar] [CrossRef] [Green Version]
- Zafrir, B.; Egbaria, A.; Stein, N.; Elis, A.; Saliba, W. PCSK9 inhibition in clinical practice: Treatment patterns and attainment of lipid goals in a large health maintenance organization. J. Clin. Lipidol. 2021, 15, 202–211.e2. [Google Scholar] [CrossRef]
- Diaz, R.; Li, Q.H.; Bhatt, D.L.; Bittner, V.A.; Baccara-Dinet, M.T.; Goodman, S.G.; Jukema, J.W.; Kimura, T.; Parkhomenko, A.; Pordy, R.; et al. Intensity of statin treatment after acute coronary syndrome, residual risk, and its modification by alirocumab: Insights from the ODYSSEY OUTCOMES trial. Eur. J. Prev. Cardiol. 2021, 28, 33–43. [Google Scholar] [CrossRef]
- Gaudet, D.; López-Sendón, J.L.; Averna, M.; Bigot, G.; Banach, M.; Letierce, A.; Loy, M.; Samuel, R.; Manvelian, G.; Batsu, I.; et al. Safety and efficacy of alirocumab in a real-life setting: The ODYSSEY APPRISE study. Eur. J. Prev. Cardiol. 2020, 28, 1864–1872. [Google Scholar] [CrossRef]
- Hines, D.M.; Rane, P.; Patel, J.; Harrison, D.J.; Wade, R.L. Treatment patterns and patient characteristics among early initiators of PCSK9 inhibitors. Vasc. Health Risk Manag. 2018, 14, 409–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Class | LDL-C (% Reduction) |
|---|---|
| PCSK-9 inhibitor | 38–72 |
| HMG-CoA inhibitors | 20–60 |
| Bile acid sequestrants | 15–30 |
| Bempedoic acid | 15–19 |
| Nicotinic acid | 10–25 |
| Cholesterol absorption inhibitors | 17 |
| Fibric acid | 6–20 |
| Parameter | Category | n (%) |
|---|---|---|
| Demographics | ||
| Males | 313 (50.2) | |
| Age (years) | <55 | 93 (14.9) |
| 55- < 65 | 202 (32.4) | |
| 65- < 75 | 254 (40.8) | |
| 75+ | 74 (11.9) | |
| Mean ± SD, n | 64.7 ± 9.1, 623 | |
| Smoking status | Current smoker | 55 (8.8) |
| Past smoker | 9 (1.4) | |
| Never Smoker | 276 (44.3) | |
| Unknown | 283 (45.4) | |
| BMI (kg/m2) | Mean ± SD, n | 28.9 ± 4.7, 493 |
| CV risk (2019 ESC/EAS guidelines) | Very high | 384 (61.6) |
| High | 138 (22.2) | |
| Lower risk | 101 (16.2) | |
| Co-morbidities | ||
| High-blood pressure registry | 389 (62.4) | |
| Cardiovascular disease * | 349 (56.0) | |
| Diabetes mellitus | 256 (41.1) | |
| Pure hypercholesterolemia | 92 (14.8) | |
| Congestive heart failure | 26 (4.2) | |
| Peripheral vascular disease | 55 (8.8) | |
| Retinopathy | 51 (8.2) | |
| Peripheral neuropathy | 40 (6.4) | |
| Cancer | 133 (21.3) | |
| Cholesterol lowering therapy | ||
| Statin | 409 (65.7) | |
| Ezetimibe | 432 (69.3) | |
| Laboratory/clinical measurements | Mean ± SD, n | |
| Total cholesterol (mg/dL) | 220.2 ± 58.1, 623 | |
| Low-Density Lipoprotein (mg/dL) | 136.0 ± 48.7, 562 | |
| High-Density Lipoprotein (mg/dL) | 50.0 ± 12.6, 623 | |
| non-HDL Cholesterol (mg/dL) | 170.5 ± 54.6, 623 | |
| e-GFR (mL/min/1.73 m2) | 82.4 ± 18.0, 590 | |
| Systolic blood pressure (mmHg) | 129.8 ± 14.2, 608 | |
| Diastolic blood pressure (mmHg) | 75.6 ± 9.1, 608 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elis, A.; Melzer Cohen, C.; Chodick, G. Real-World Use of Alirocumab: Experience from a Large Healthcare Provider. J. Clin. Med. 2023, 12, 1084. https://doi.org/10.3390/jcm12031084
Elis A, Melzer Cohen C, Chodick G. Real-World Use of Alirocumab: Experience from a Large Healthcare Provider. Journal of Clinical Medicine. 2023; 12(3):1084. https://doi.org/10.3390/jcm12031084
Chicago/Turabian StyleElis, Avishay, Cheli Melzer Cohen, and Gabriel Chodick. 2023. "Real-World Use of Alirocumab: Experience from a Large Healthcare Provider" Journal of Clinical Medicine 12, no. 3: 1084. https://doi.org/10.3390/jcm12031084