
Comprehensive Management of Blood Pressure in Patients with Septic AKI


Abstract
:1. Introduction
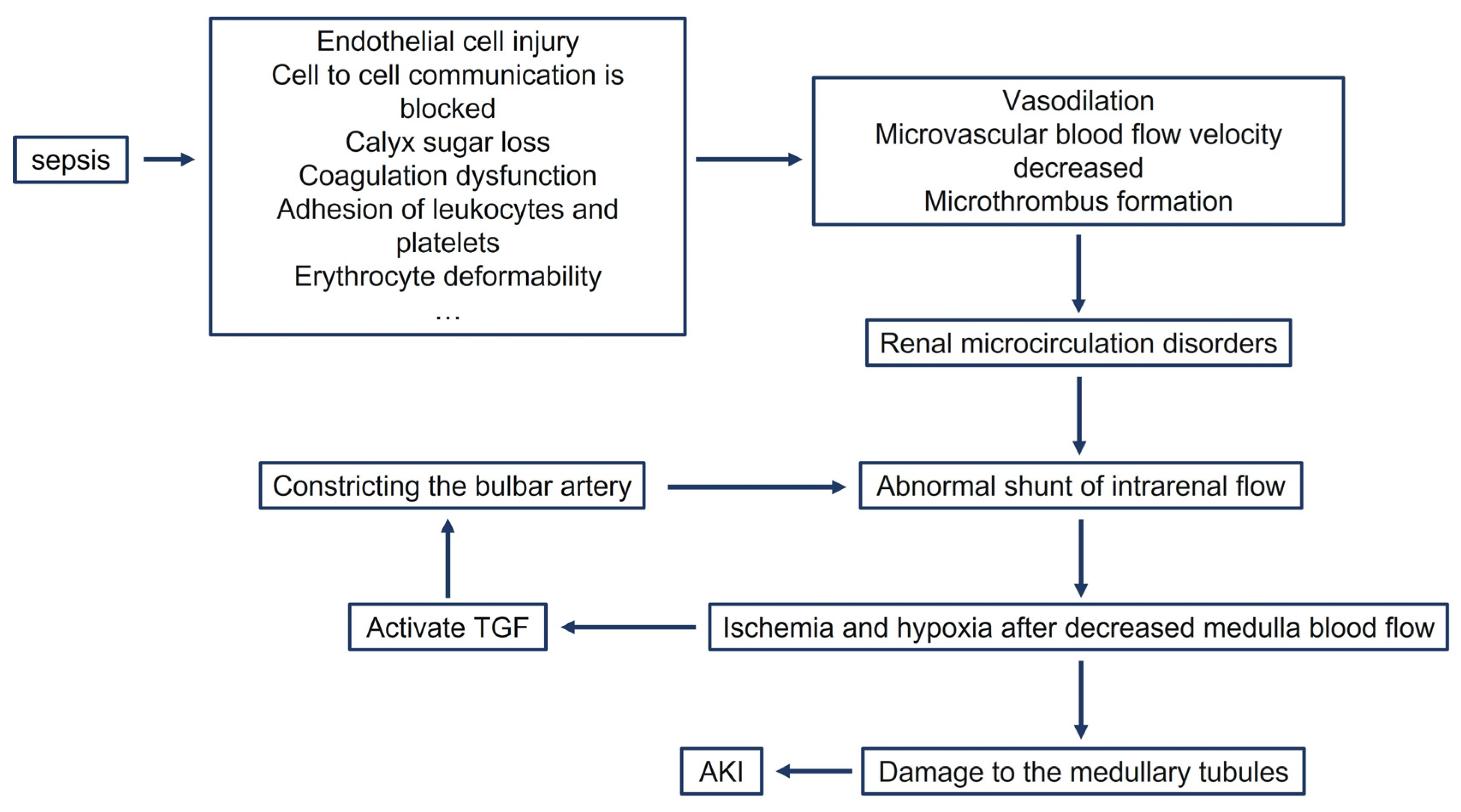
2. Microcirculatory Disorders
3. Fluid Management
4. Vasopressor

{kind=link}
| Drug Name | Receptor | Effects on Renal Function | Effect on Urine Output | Effects on the Medulla | Reference |
|---|---|---|---|---|---|
| Norepinephrine | α-adrenergic receptor | Improve | Increase | Exacerbate hypoxia | [53,54,55,56,57,58] |
| Dopamine | α receptor, β receptor, and peripheral dopamine receptor | Worsen | Unknown | Unknown | [60,61,80,81] |
| Vasopressin | AVPR1A | Improve | Increase | Unknown | [67,68,69,70,71,72] |
| Angiotensin II | Angiotensin II receptor | Improve | Increase | Does not exacerbate hypoxia | [74,77,78] |
5. Blood Pressure Target
| Nation | Time | Type of Study | Number of Cases | Indicator | Target | Reference |
|---|---|---|---|---|---|---|
| U.S. | January 2007 to January 2009 | Retrospective study | 233 | MAP | Prehospital MAP | [90] |
| France | October 2007 to April 2009 | Prospective study | 217 | MAP | 72–82 mmHg | [89] |
| U.S. | 2010 to 2016 | Retrospective study | 8782 | MAP | Much higher than 65 mmHg | [86] |
| Finland | September 2011 to February 2012 | Prospective study | 423 | MAP | Above 73 mmHg | [87] |
| China | January 2015 to December 2016 | Retrospective study | 63 | MAP | Above 77 mmHg | [88] |
| France | August 2016 to July 2017 | Prospective study | 26 (with a history of hypertension) | MAP | 80–85 mmHg | [92] |
| U.K. | July 2007 to June 2009 | Retrospective study | 790 | MPP | Above 60 mmHg | [95] |
6. Replacement Therapy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; George, C.; Bellomo, R. Early acute kidney injury and sepsis: A multicentre evaluation. Crit. Care 2008, 12, R47. [Google Scholar] [CrossRef] [Green Version]
- Bagshaw, S.M.; Uchino, S.; Bellomo, R.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; Gibney, N.; et al. Septic acute kidney injury in critically ill patients: Clinical characteristics and outcomes. Clin. J. Am. Soc. Nephrol. CJASN 2007, 2, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez, H.; Kellum, J.A. Sepsis-induced acute kidney injury. Curr. Opin. Crit. Care 2016, 22, 546–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Kellum, J.A.; Ronco, C.; Wald, R.; Martensson, J.; Maiden, M.; Bagshaw, S.M.; Glassford, N.J.; Lankadeva, Y.; Vaara, S.T.; et al. Acute kidney injury in sepsis. Intensive Care Med. 2017, 43, 816–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term risk of mortality and other adverse outcomes after acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2009, 53, 961–973. [Google Scholar] [CrossRef] [Green Version]
- Gomez, H.; Ince, C.; De Backer, D.; Pickkers, P.; Payen, D.; Hotchkiss, J.; Kellum, J.A. A unified theory of sepsis-induced acute kidney injury: Inflammation, microcirculatory dysfunction, bioenergetics, and the tubular cell adaptation to injury. Shock 2014, 41, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarbock, A.; Gomez, H.; Kellum, J.A. Sepsis-induced acute kidney injury revisited: Pathophysiology, prevention and future therapies. Curr. Opin. Crit. Care 2014, 20, 588–595. [Google Scholar] [CrossRef]
- Deng, J.; Tan, W.; Luo, Q.; Lin, L.; Zheng, L.; Yang, J. Long Non-coding RNA MEG3 Promotes Renal Tubular Epithelial Cell Pyroptosis by Regulating the miR-18a-3p/GSDMD Pathway in Lipopolysaccharide-Induced Acute Kidney Injury. Front. Physiol. 2021, 12, 663216. [Google Scholar] [CrossRef]
- Lerolle, N.; Nochy, D.; Guérot, E.; Bruneval, P.; Fagon, J.Y.; Diehl, J.L.; Hill, G. Histopathology of septic shock induced acute kidney injury: Apoptosis and leukocytic infiltration. Intensive Care Med. 2010, 36, 471–478. [Google Scholar] [CrossRef]
- Takasu, O.; Gaut, J.P.; Watanabe, E.; To, K.; Fagley, R.E.; Sato, B.; Jarman, S.; Efimov, I.R.; Janks, D.L.; Srivastava, A.; et al. Mechanisms of cardiac and renal dysfunction in patients dying of sepsis. Am. J. Respir. Crit. Care Med. 2013, 187, 509–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mårtensson, J.; Bellomo, R. Pathophysiology of Septic Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 36–46. [Google Scholar] [CrossRef]
- Bavishi, C.; Bangalore, S.; Messerli, F.H. Outcomes of Intensive Blood Pressure Lowering in Older Hypertensive Patients. J. Am. Coll. Cardiol. 2017, 69, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Tao, Y.H.; Yang, J.; Wang, S.W.; Zhou, J.J.; Yang, L.C. Risk Factors for Sepsis Associated-Acute Kidney Injury in Intensive Care Unit Patients. Sichuan Da Xue Xue Bao. Yi Xue Ban = J. Sichuan Univ. Med. Sci. Ed. 2020, 51, 708–713. [Google Scholar] [CrossRef]
- Iram, H.; Ali, M.; Kumar, V.; Ejaz, A.; Solangi, S.A.; Junejo, A.M.; Solangi, S.A.; Un Nisa, N. Frequency of Risk Factors and Outcome of Hospital-Acquired Acute Kidney Injury. Cureus 2020, 12, e12001. [Google Scholar] [CrossRef] [PubMed]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; de Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension With Acute Kidney Injury. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2015, 66, 602–612. [Google Scholar] [CrossRef] [Green Version]
- Bo, S.; Gruden, G.; Charbonnier, E.; Martorana, M.; Gambino, R.; Cassader, M.; Gentile, L.; Cavallo-Perin, P.; Durazzo, M. High-normal blood pressure and impaired renal function. A prospective study in a population-based cohort. Minerva Med. 2014, 105, 211–219. [Google Scholar]
- De Backer, D.; Ricottilli, F.; Ospina-Tascón, G.A. Septic shock: A microcirculation disease. Curr. Opin. Anaesthesiol. 2021, 34, 85–91. [Google Scholar] [CrossRef]
- Furst, B.; Bughrara, N.; Musuku, S.R. Macrocirculation and Microcirculation in Septic Shock. Anesth. Analg. 2021, 133, e37–e38. [Google Scholar] [CrossRef]
- De Backer, D.; Donadello, K.; Taccone, F.S.; Ospina-Tascon, G.; Salgado, D.; Vincent, J.L. Microcirculatory alterations: Potential mechanisms and implications for therapy. Ann. Intensive Care 2011, 1, 27. [Google Scholar] [CrossRef] [Green Version]
- Ertmer, C.; Rehberg, S. Pathophysiology of sepsis. Dtsch. Med. Wochenschr. 1946 2016, 141, 1067–1073. [Google Scholar] [CrossRef]
- Evans, R.G.; Gardiner, B.S.; Smith, D.W.; O’Connor, P.M. Intrarenal oxygenation: Unique challenges and the biophysical basis of homeostasis. Am. J. Physiol.-Ren. Physiol. 2008, 295, F1259–F1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallone, T.L.; Edwards, A.; Mattson, D.L. Renal medullary circulation. Compr. Physiol. 2012, 2, 97–140. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.G.; Ince, C.; Joles, J.A.; Smith, D.W.; May, C.N.; O’Connor, P.M.; Gardiner, B.S. Haemodynamic influences on kidney oxygenation: Clinical implications of integrative physiology. Clin. Exp. Pharm. Physiol. 2013, 40, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Regner, K.R.; Zuk, A.; Van Why, S.K.; Shames, B.D.; Ryan, R.P.; Falck, J.R.; Manthati, V.L.; McMullen, M.E.; Ledbetter, S.R.; Roman, R.J. Protective effect of 20-HETE analogues in experimental renal ischemia reperfusion injury. Kidney Int. 2009, 75, 511–517. [Google Scholar] [CrossRef] [Green Version]
- Fry, B.C.; Edwards, A.; Sgouralis, I.; Layton, A.T. Impact of renal medullary three-dimensional architecture on oxygen transport. Am. J. Physiol.-Ren. Physiol. 2014, 307, F263–F272. [Google Scholar] [CrossRef] [Green Version]
- Pannabecker, T.L.; Layton, A.T. Targeted delivery of solutes and oxygen in the renal medulla: Role of microvessel architecture. Am. J. Physiol.-Ren. Physiol. 2014, 307, F649–F655. [Google Scholar] [CrossRef] [Green Version]
- Devarajan, P. Update on mechanisms of ischemic acute kidney injury. J. Am. Soc. Nephrol. JASN 2006, 17, 1503–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regner, K.R.; Roman, R.J. Role of medullary blood flow in the pathogenesis of renal ischemia-reperfusion injury. Curr. Opin. Nephrol. Hypertens. 2012, 21, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.J.; Gardiner, B.S.; Evans, R.G.; Smith, D.W. A model of oxygen transport in the rat renal medulla. Am. J. Physiol.-Ren. Physiol. 2018, 315, F1787–F1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcoux, A.A.; Tremblay, L.E.; Slimani, S.; Fiola, M.J.; Mac-Way, F.; Haydock, L.; Garneau, A.P.; Isenring, P. Anatomophysiology of the Henle’s Loop: Emphasis on the Thick Ascending Limb. Compr. Physiol. 2021, 12, 3119–3139. [Google Scholar] [CrossRef] [PubMed]
- Cinel, I.; Kasapoglu, U.S.; Gul, F.; Dellinger, R.P. The initial resuscitation of septic shock. J. Crit. Care 2020, 57, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Kiers, H.D.; Griesdale, D.E.; Litchfield, A.; Reynolds, S.; Gibney, R.T.; Chittock, D.; Pickkers, P.; Sweet, D.D. Effect of early achievement of physiologic resuscitation goals in septic patients admitted from the ward on the kidneys. J. Crit. Care 2010, 25, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Chen, T.T.; Wu, M.Y.; Chan, M.C.; Shih, M.C.; Tu, Y.K. Resuscitation fluid types in sepsis, surgical, and trauma patients: A systematic review and sequential network meta-analyses. Crit. Care 2020, 24, 693. [Google Scholar] [CrossRef]
- Li, B.; Zhao, H.; Zhang, J.; Yan, Q.; Li, T.; Liu, L. Resuscitation Fluids in Septic Shock: A Network Meta-Analysis of Randomized Controlled Trials. Shock 2020, 53, 679–685. [Google Scholar] [CrossRef]
- Brunkhorst, F.M.; Engel, C.; Bloos, F.; Meier-Hellmann, A.; Ragaller, M.; Weiler, N.; Moerer, O.; Gruendling, M.; Oppert, M.; Grond, S.; et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N. Engl. J. Med. 2008, 358, 125–139. [Google Scholar] [CrossRef] [Green Version]
- Reinhart, K.; Perner, A.; Sprung, C.L.; Jaeschke, R.; Schortgen, F.; Johan Groeneveld, A.B.; Beale, R.; Hartog, C.S. Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients. Intensive Care Med. 2012, 38, 368–383. [Google Scholar] [CrossRef]
- Kampmeier, T.G.; Arnemann, P.H.; Hessler, M.; Bockbreder, K.; Wald, A.; Morelli, A.; Rehberg, S.W.; Ertmer, C. Effects of resuscitation with human albumin 5%, hydroxyethyl starch 130/0.4 6%, or crystalloid on kidney damage in an ovine model of septic shock. Br. J. Anaesth. 2018, 121, 581–587. [Google Scholar] [CrossRef] [Green Version]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yunos, N.M.; Bellomo, R.; Hegarty, C.; Story, D.; Ho, L.; Bailey, M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA 2012, 308, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Yunos, N.M.; Kim, I.B.; Bellomo, R.; Bailey, M.; Ho, L.; Story, D.; Gutteridge, G.A.; Hart, G.K. The biochemical effects of restricting chloride-rich fluids in intensive care. Crit. Care Med. 2011, 39, 2419–2424. [Google Scholar] [CrossRef]
- Zhang, L.; Chen, Z.; Diao, Y.; Yang, Y.; Fu, P. Associations of fluid overload with mortality and kidney recovery in patients with acute kidney injury: A systematic review and meta-analysis. J. Crit. Care 2015, 30, 860.e7–860.e13. [Google Scholar] [CrossRef] [PubMed]
- Selewski, D.T.; Goldstein, S.L. The role of fluid overload in the prediction of outcome in acute kidney injury. Pediatr. Nephrol. 2018, 33, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Montomoli, J.; Donati, A.; Ince, C. Acute Kidney Injury and Fluid Resuscitation in Septic Patients: Are We Protecting the Kidney? Nephron 2019, 143, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Gelman, S. Venous function and central venous pressure: A physiologic story. Anesthesiology 2008, 108, 735–748. [Google Scholar] [CrossRef] [Green Version]
- Reems, M.M.; Aumann, M. Central venous pressure: Principles, measurement, and interpretation. Compend. Contin. Educ. Vet. 2012, 34, E1. [Google Scholar] [PubMed]
- Chen, C.Y.; Zhou, Y.; Wang, P.; Qi, E.Y.; Gu, W.J. Elevated central venous pressure is associated with increased mortality and acute kidney injury in critically ill patients: A meta-analysis. Crit. Care 2020, 24, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, Y.; Wang, X.; Li, B.; Rello, J.; Kim, W.Y.; Wang, X.; Hu, Z. Impact of central venous pressure on the mortality of patients with sepsis-related acute kidney injury: A propensity score-matched analysis based on the MIMIC IV database. Ann. Transl. Med. 2022, 10, 199. [Google Scholar] [CrossRef]
- Nadeau-Fredette, A.C.; Bouchard, J. Fluid management and use of diuretics in acute kidney injury. Adv. Chronic Kidney Dis. 2013, 20, 45–55. [Google Scholar] [CrossRef]
- Malbrain, M.L.; Marik, P.E.; Witters, I.; Cordemans, C.; Kirkpatrick, A.W.; Roberts, D.J.; Van Regenmortel, N. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: A systematic review with suggestions for clinical practice. Anaesthesiol. Intensive Ther. 2014, 46, 361–380. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; Roberts, D.J.; De Waele, J.; Jaeschke, R.; Malbrain, M.L.; De Keulenaer, B.; Duchesne, J.; Bjorck, M.; Leppaniemi, A.; Ejike, J.C.; et al. Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013, 39, 1190–1206. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; Roberts, D.J.; Jaeschke, R.; De Waele, J.J.; De Keulenaer, B.L.; Duchesne, J.; Bjorck, M.; Leppäniemi, A.; Ejike, J.C.; Sugrue, M.; et al. Methodological background and strategy for the 2012-2013 updated consensus definitions and clinical practice guidelines from the abdominal compartment society. Anaesthesiol. Intensive Ther. 2015, 47, S63–S77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruslan, M.A.; Baharuddin, K.A.; Noor, N.M.; Yazid, M.B.; Noh, A.Y.M.; Rahman, A. Norepinephrine in Septic Shock: A Systematic Review and Meta-analysis. West. J. Emerg. Med. 2021, 22, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Hamzaoui, O.; Scheeren, T.W.L.; Teboul, J.L. Norepinephrine in septic shock: When and how much? Curr. Opin. Crit. Care 2017, 23, 342–347. [Google Scholar] [CrossRef]
- Bellomo, R.; Giantomasso, D.D. Noradrenaline and the kidney: Friends or foes? Crit. Care 2001, 5, 294–298. [Google Scholar] [CrossRef]
- Di Giantomasso, D.; May, C.N.; Bellomo, R. Norepinephrine and vital organ blood flow during experimental hyperdynamic sepsis. Intensive Care Med. 2003, 29, 1774–1781. [Google Scholar] [CrossRef]
- Lankadeva, Y.R.; Kosaka, J.; Evans, R.G.; Bailey, S.R.; Bellomo, R.; May, C.N. Intrarenal and urinary oxygenation during norepinephrine resuscitation in ovine septic acute kidney injury. Kidney Int. 2016, 90, 100–108. [Google Scholar] [CrossRef]
- Calzavacca, P.; Evans, R.G.; Bailey, M.; Bellomo, R.; May, C.N. Variable responses of regional renal oxygenation and perfusion to vasoactive agents in awake sheep. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2015, 309, R1226–R1233. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Wang, L.; Shi, H.; Gao, M. Comparison of clinical effect of dopamine and norepinephrine in the treatment of septic shock. Pak. J. Pharm. Sci. 2015, 28, 1461–1464. [Google Scholar]
- De Backer, D.; Scolletta, S. Clinical management of the cardiovascular failure in sepsis. Curr. Vasc. Pharmacol. 2013, 11, 222–242. [Google Scholar]
- Lauschke, A.; Teichgräber, U.K.; Frei, U.; Eckardt, K.U. ‘Low-dose’ dopamine worsens renal perfusion in patients with acute renal failure. Kidney Int. 2006, 69, 1669–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Backer, D.; Aldecoa, C.; Njimi, H.; Vincent, J.L. Dopamine versus norepinephrine in the treatment of septic shock: A meta-analysis. Crit. Care Med. 2012, 40, 725–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, A.M.; Shieh, H.H.; Bousso, A.; Góes, P.F.; de Cássia, F.O.F.I.; de Souza, D.C.; Paulo, R.L.; Chagas, F.; Gilio, A.E. Double-Blind Prospective Randomized Controlled Trial of Dopamine Versus Epinephrine as First-Line Vasoactive Drugs in Pediatric Septic Shock. Crit. Care Med. 2015, 43, 2292–2302. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Peter, O. Dopamine versus noradrenaline in septic shock. Australas. Med. J. 2011, 4, 571–574. [Google Scholar] [CrossRef]
- Kohn-Loncarica, G.; Fustiñana, A.; Santos, C.; Lantelli, G.P.; Rowensztein, H.; González-Dambrauskas, S. Clinical outcome of children with fluid-refractory septic shock treated with dopamine or epinephrine. A retrospective study at a pediatric emergency department in Argentina. Rev. Bras. Ter. Intensiv. 2020, 32, 551–556. [Google Scholar] [CrossRef]
- Belletti, A.; Benedetto, U.; Biondi-Zoccai, G.; Leggieri, C.; Silvani, P.; Angelini, G.D.; Zangrillo, A.; Landoni, G. The effect of vasoactive drugs on mortality in patients with severe sepsis and septic shock. A network meta-analysis of randomized trials. J. Crit. Care 2017, 37, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Russell, J.A. Bench-to-bedside review: Vasopressin in the management of septic shock. Crit. Care 2011, 15, 226. [Google Scholar] [CrossRef] [Green Version]
- Der-Nigoghossian, C.; Hammond, D.A.; Ammar, M.A. Narrative Review of Controversies Involving Vasopressin Use in Septic Shock and Practical Considerations. Ann. Pharmacother. 2020, 54, 706–714. [Google Scholar] [CrossRef]
- Di Giantomasso, D.; Morimatsu, H.; Bellomo, R.; May, C.N. Effect of low-dose vasopressin infusion on vital organ blood flow in the conscious normal and septic sheep. Anaesth. Intensive Care 2006, 34, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, N.; Iguchi, N.; Evans, R.G.; Hood, S.G.; Bellomo, R.; May, C.N.; Lankadeva, Y.R. Beneficial Effects of Vasopressin Compared With Norepinephrine on Renal Perfusion, Oxygenation, and Function in Experimental Septic Acute Kidney Injury. Crit. Care Med. 2020, 48, e951–e958. [Google Scholar] [CrossRef]
- Wang, J.; Shi, M.; Huang, L.; Li, Q.; Meng, S.; Xu, J.; Xue, M.; Xie, J.; Liu, S.; Huang, Y. Addition of terlipressin to norepinephrine in septic shock and effect of renal perfusion: A pilot study. Ren. Fail. 2022, 44, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wu, C.; Shen, Q.; Xu, H.; Fang, Y.; Mao, W. The effect of early vasopressin use on patients with septic shock: A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 48, 203–208. [Google Scholar] [CrossRef]
- Gordon, A.C.; Mason, A.J.; Thirunavukkarasu, N.; Perkins, G.D.; Cecconi, M.; Cepkova, M.; Pogson, D.G.; Aya, H.D.; Anjum, A.; Frazier, G.J.; et al. Effect of Early Vasopressin vs Norepinephrine on Kidney Failure in Patients With Septic Shock: The VANISH Randomized Clinical Trial. JAMA 2016, 316, 509–518. [Google Scholar] [CrossRef]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017, 377, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, A.; Kobori, H. Independent regulation of renin-angiotensin-aldosterone system in the kidney. Clin. Exp. Nephrol. 2018, 22, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Patzak, A.; Lai, E.; Persson, P.B.; Persson, A.E. Angiotensin II-nitric oxide interaction in glomerular arterioles. Clin. Exp. Pharm. Physiol. 2005, 32, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Lankadeva, Y.R.; Kosaka, J.; Evans, R.G.; Bellomo, R.; May, C.N. Urinary Oxygenation as a Surrogate Measure of Medullary Oxygenation during Angiotensin II Therapy in Septic Acute Kidney Injury. Crit. Care Med. 2018, 46, e41–e48. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Langenberg, C.; Bellomo, R.; May, C.N. Angiotensin II in experimental hyperdynamic sepsis. Crit. Care 2009, 13, R190. [Google Scholar] [CrossRef] [Green Version]
- Tumlin, J.A.; Murugan, R.; Deane, A.M.; Ostermann, M.; Busse, L.W.; Ham, K.R.; Kashani, K.; Szerlip, H.M.; Prowle, J.R.; Bihorac, A.; et al. Outcomes in Patients with Vasodilatory Shock and Renal Replacement Therapy Treated with Intravenous Angiotensin II. Crit. Care Med. 2018, 46, 949–957. [Google Scholar] [CrossRef]
- Wen, L.; Xu, L. The efficacy of dopamine versus epinephrine for pediatric or neonatal septic shock: A meta-analysis of randomized controlled studies. Ital. J. Pediatr. 2020, 46, 6. [Google Scholar] [CrossRef] [Green Version]
- Baske, K.; Saini, S.S.; Dutta, S.; Sundaram, V. Epinephrine versus dopamine in neonatal septic shock: A double-blind randomized controlled trial. Eur. J. Pediatr. 2018, 177, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Chawla, L.S.; Keener, C.; Singbartl, K.; Palevsky, P.M.; Pike, F.L.; Yealy, D.M.; Huang, D.T.; Angus, D.C. The Effects of Alternative Resuscitation Strategies on Acute Kidney Injury in Patients with Septic Shock. Am. J. Respir. Crit. Care Med. 2016, 193, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiden, M.J.; Otto, S.; Brealey, J.K.; Finnis, M.E.; Chapman, M.J.; Kuchel, T.R.; Nash, C.H.; Edwards, J.; Bellomo, R. Structure and Function of the Kidney in Septic Shock. A Prospective Controlled Experimental Study. Am. J. Respir. Crit. Care Med. 2016, 194, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Pinsky, M.R. Personalizing blood pressure management in septic shock. Ann. Intensive Care 2015, 5, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maheshwari, K.; Nathanson, B.H.; Munson, S.H.; Khangulov, V.; Stevens, M.; Badani, H.; Khanna, A.K.; Sessler, D.I. The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Intensive Care Med. 2018, 44, 857–867. [Google Scholar] [CrossRef] [Green Version]
- Poukkanen, M.; Wilkman, E.; Vaara, S.T.; Pettilä, V.; Kaukonen, K.M.; Korhonen, A.M.; Uusaro, A.; Hovilehto, S.; Inkinen, O.; Laru-Sompa, R.; et al. Hemodynamic variables and progression of acute kidney injury in critically ill patients with severe sepsis: Data from the prospective observational FINNAKI study. Crit. Care 2013, 17, R295. [Google Scholar] [CrossRef] [Green Version]
- Ko, C.H.; Lan, Y.W.; Chen, Y.C.; Cheng, T.T.; Yu, S.F.; Cidem, A.; Liu, Y.H.; Kuo, C.W.; Yen, C.C.; Chen, W.; et al. Effects of Mean Artery Pressure and Blood pH on Survival Rate of Patients with Acute Kidney Injury Combined with Acute Hypoxic Respiratory Failure: A Retrospective Study. Medicina 2021, 57, 1243. [Google Scholar] [CrossRef]
- Badin, J.; Boulain, T.; Ehrmann, S.; Skarzynski, M.; Bretagnol, A.; Buret, J.; Benzekri-Lefevre, D.; Mercier, E.; Runge, I.; Garot, D.; et al. Relation between mean arterial pressure and renal function in the early phase of shock: A prospective, explorative cohort study. Crit. Care 2011, 15, R135. [Google Scholar] [CrossRef] [Green Version]
- Moman, R.N.; Ostby, S.A.; Akhoundi, A.; Kashyap, R.; Kashani, K. Impact of individualized target mean arterial pressure for septic shock resuscitation on the incidence of acute kidney injury: A retrospective cohort study. Ann. Intensive Care 2018, 8, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewitte, A.; Labat, A.; Duvignaud, P.A.; Bouche, G.; Joannes-Boyau, O.; Ripoche, J.; Hilbert, G.; Gruson, D.; Rubin, S.; Ouattara, A.; et al. High mean arterial pressure target to improve sepsis-associated acute kidney injury in patients with prior hypertension: A feasibility study. Ann. Intensive Care 2021, 11, 139. [Google Scholar] [CrossRef] [PubMed]
- Asfar, P.; Meziani, F.; Hamel, J.F.; Grelon, F.; Megarbane, B.; Anguel, N.; Mira, J.P.; Dequin, P.F.; Gergaud, S.; Weiss, N.; et al. High versus low blood-pressure target in patients with septic shock. N. Engl. J. Med. 2014, 370, 1583–1593. [Google Scholar] [CrossRef]
- Panwar, R.; Lanyon, N.; Davies, A.R.; Bailey, M.; Pilcher, D.; Bellomo, R. Mean perfusion pressure deficit during the initial management of shock—An observational cohort study. J. Crit. Care 2013, 28, 816–824. [Google Scholar] [CrossRef]
- Ostermann, M.; Hall, A.; Crichton, S. Low mean perfusion pressure is a risk factor for progression of acute kidney injury in critically ill patients—A retrospective analysis. BMC Nephrol. 2017, 18, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, B.T.; Chan, M.J.; Glassford, N.J.; Mårtensson, J.; Bion, V.; Chai, S.Y.; Oughton, C.; Tsuji, I.Y.; Candal, C.L.; Bellomo, R. Mean arterial pressure and mean perfusion pressure deficit in septic acute kidney injury. J. Crit. Care 2015, 30, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Panwar, R.; Van Haren, F.; Cazzola, F.; Nourse, M.; Brinkerhoff, G.; Quail, A. Standard care versus individualized blood pressure targets among critically ill patients with shock: A multicenter feasibility and preliminary efficacy study. J. Crit. Care 2022, 70, 154052. [Google Scholar] [CrossRef]
- Romagnoli, S.; Ricci, Z.; Ronco, C. CRRT for sepsis-induced acute kidney injury. Curr. Opin. Crit. Care 2018, 24, 483–492. [Google Scholar] [CrossRef]
- Gibney, N.; Cerda, J.; Davenport, A.; Ramirez, J.; Singbartl, K.; Leblanc, M.; Ronco, C. Volume management by renal replacement therapy in acute kidney injury. Int. J. Artif. Organs 2008, 31, 145–155. [Google Scholar] [CrossRef]
- Legrand, M.; Darmon, M.; Joannidis, M.; Payen, D. Management of renal replacement therapy in ICU patients: An international survey. Intensive Care Med. 2013, 39, 101–108. [Google Scholar] [CrossRef]
- Summary of Recommendation Statements. Kidney Int. Suppl. 2012, 2, 8–12. [CrossRef] [PubMed] [Green Version]
- Schortgen, F.; Soubrier, N.; Delclaux, C.; Thuong, M.; Girou, E.; Brun-Buisson, C.; Lemaire, F.; Brochard, L. Hemodynamic tolerance of intermittent hemodialysis in critically ill patients: Usefulness of practice guidelines. Am. J. Respir. Crit. Care Med. 2000, 162, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Vodovar, D.; Mégarbane, B. Extracorporeal Kidney-Replacement Therapy for Acute Kidney Injury. N. Engl. J. Med. 2022, 386, 2250. [Google Scholar] [CrossRef] [PubMed]
- Fathima, N.; Kashif, T.; Janapala, R.N.; Jayaraj, J.S.; Qaseem, A. Single-best Choice Between Intermittent Versus Continuous Renal Replacement Therapy: A Review. Cureus 2019, 11, e5558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shawwa, K.; Kompotiatis, P.; Jentzer, J.C.; Wiley, B.M.; Williams, A.W.; Dillon, J.J.; Albright, R.C.; Kashani, K.B. Hypotension within one-hour from starting CRRT is associated with in-hospital mortality. J. Crit. Care 2019, 54, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Santiago, M.J.; López-Herce, J.; Urbano, J.; Solana, M.J.; del Castillo, J.; Sánchez, A.; Bellón, J.M. Continuous renal replacement therapy in children after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2013, 146, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Yun, D.; Kwon, S.; Jin, K.; Han, S.; Kim, D.K.; Oh, K.H.; Joo, K.W.; Kim, Y.S.; Kim, S.; et al. Target value of mean arterial pressure in patients undergoing continuous renal replacement therapy due to acute kidney injury. BMC Nephrol. 2021, 22, 20. [Google Scholar] [CrossRef]
- Wang, Y.; Gallagher, M.; Li, Q.; Lo, S.; Cass, A.; Finfer, S.; Myburgh, J.; Bouman, C.; Faulhaber-Walter, R.; Kellum, J.A.; et al. Renal replacement therapy intensity for acute kidney injury and recovery to dialysis independence: A systematic review and individual patient data meta-analysis. Nephrol. Dial. Transplant. 2018, 33, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef]
- Xing, Z.Q.; Liu, D.W.; Wang, X.T.; Long, Y.; Zhang, H.M.; Pan, P.; Su, L.X. Early initiation renal replacement therapy for fluid management to reduce central venous pressure is more conducive to renal function recovery in patients with acute kidney injury. Chin. Med. J. 2019, 132, 1328–1335. [Google Scholar] [CrossRef]
- Hellman, T.; Uusalo, P.; Järvisalo, M.J. Renal Replacement Techniques in Septic Shock. Int. J. Mol. Sci. 2021, 22, 10238. [Google Scholar] [CrossRef] [PubMed]
- Schwindenhammer, V.; Girardot, T.; Chaulier, K.; Grégoire, A.; Monard, C.; Huriaux, L.; Illinger, J.; Leray, V.; Uberti, T.; Crozon-Clauzel, J.; et al. oXiris® Use in Septic Shock: Experience of Two French Centres. Blood Purif. 2019, 47 (Suppl. S3), 29–35. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, D.P.; Caramori, J.T.; Martim, L.C.; Barretti, P.; Balbi, A.L. High volume peritoneal dialysis vs daily hemodialysis: A randomized, controlled trial in patients with acute kidney injury. Kidney Int. Suppl. 2008, 73, S87–S93. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, J.; Li, L.; Feng, Y.; Yang, J. Comprehensive Management of Blood Pressure in Patients with Septic AKI. J. Clin. Med. 2023, 12, 1018. https://doi.org/10.3390/jcm12031018
Deng J, Li L, Feng Y, Yang J. Comprehensive Management of Blood Pressure in Patients with Septic AKI. Journal of Clinical Medicine. 2023; 12(3):1018. https://doi.org/10.3390/jcm12031018
Chicago/Turabian StyleDeng, Junhui, Lina Li, Yuanjun Feng, and Jurong Yang. 2023. "Comprehensive Management of Blood Pressure in Patients with Septic AKI" Journal of Clinical Medicine 12, no. 3: 1018. https://doi.org/10.3390/jcm12031018