
Comparison of Hemodynamic Response between Patients with Systolic Heart Failure Differing in Serum Aldosterone Concentrations during and after a 6-Minute Walk Test
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Assessment
2.3. 6-Minute Walk Test
2.4. Biochemical Analysis
2.5. Transthoracic Echocardiography
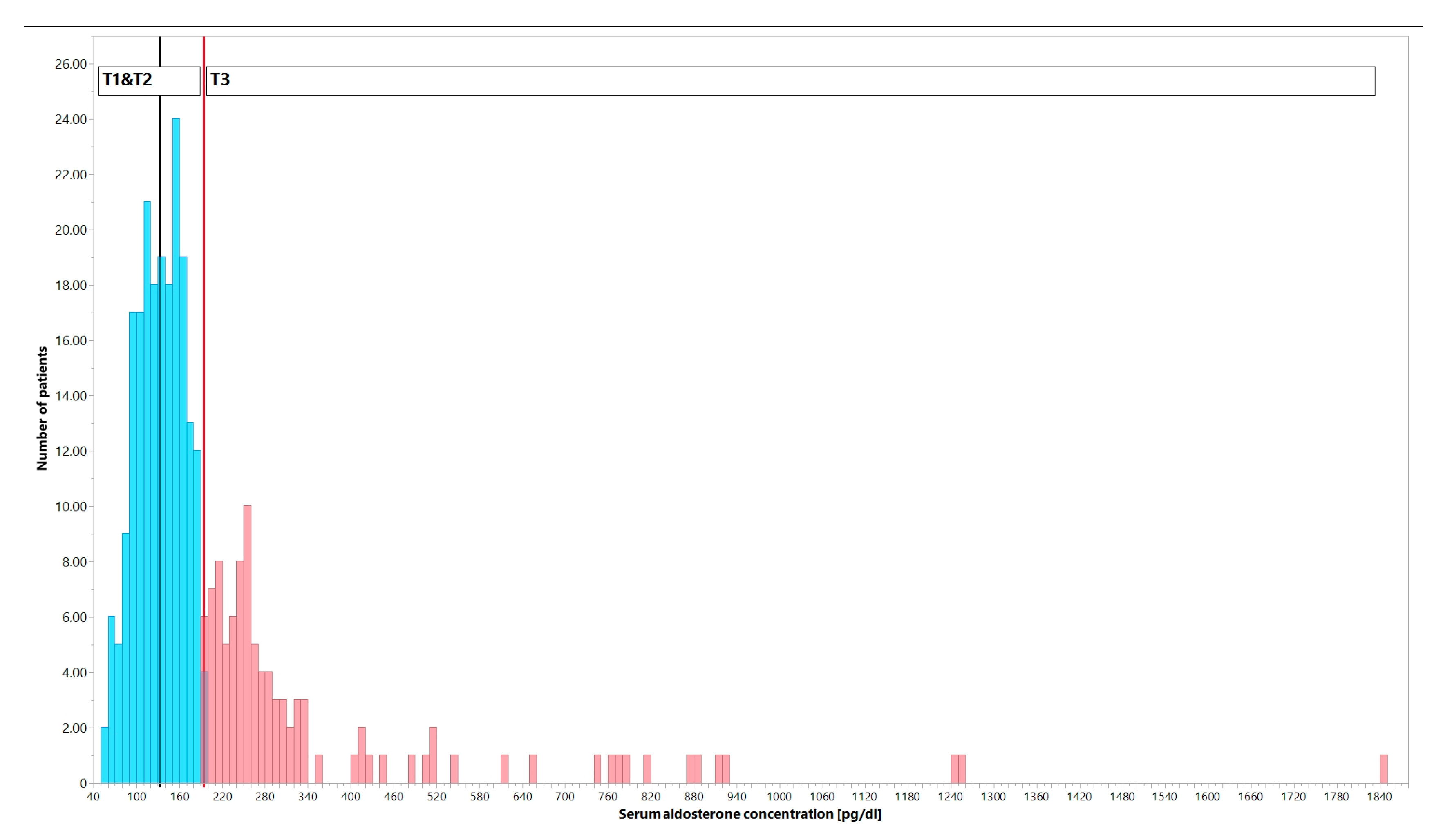
2.6. Dividing Patients into Low and High Serum Aldosterone Concentration Groups
2.7. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics between T1–T2 and T3 Patients
3.2. Comparison of Hemodynamic Profiles between T1–T2 and T3 Patients
4. Discussion
4.1. Clinical Implications and Prognostic Value of Low Blood Pressure in Patients with Stable HFrEF
4.2. Neurohormonal Adaptation in Patients with Stable HFrEF
4.3. Pharmacological Impact
4.4. Limitations
4.5. The Novelty of the Study and Potential Clinical Impact
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 6MWT | 6 min walk test |
| ACE | angiotensin-converting enzyme inhibitor |
| AF | atrial fibrillation |
| ARBs | angiotensin II receptor blocker |
| BMI | body mass index |
| BP | blood pressure |
| CVS | cardiovascular system |
| Crea | creatinine |
| CRT-D | cardiac resynchronization therapy defibrillator |
| DBP | diastolic blood pressure |
| E-wave velocity | peak early diastolic LV inflow |
| ECG | electrocardiography |
| eGFRC-G | estimated glomerular filtration rate by Cockcroft–Gault equation |
| HA | hypertension |
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
| HR | heart rate |
| ICD | implantable cardioverter-defibrillator |
| IVT | intra-ventricular septum thickness |
| K | potassium |
| LA | left atrium |
| LV | left ventricle |
| LVEDD | left ventricle end-diastolic diameter in the parasternal long-axis view |
| LVEF | left ventricular ejection fraction by the biplane Simpson method |
| LVESD | left ventricle end-systolic diameter in the parasternal long-axis view |
| LVPWT | left ventricle posterior (basal segment of the inferolateral) wall thickness |
| MBP | mean blood pressure |
| Na | sodium |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| NYHA | New York Heart Association I-IV |
| PP | pulse pressure |
| RAAS | renin-angiotensin-aldosterone system |
| resting SpO2 | resting stable oxygen saturation |
| RPE | Borg Rating of Perceived Exertion Scale |
| RV | right ventricle |
| SBP | systolic blood pressure |
| T1 | first tertile |
| T2 | second tertile |
| T3 | third tertile |
| TIA | transient ischemic attack |
References
- Durante, A.; Peretto, G.; Laricchia, A.; Ancona, F.; Spartera, M.; Mangieri, A.; Cianflone, D. Role of the Renin-Angiotensin-Aldosterone System in the Pathogenesis of Atherosclerosis. Curr. Pharm. Des. 2012, 18, 981–1004. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, R.D.; Mehta, R.M.; Tripathi, R.; Reed, G.L.; Gladysheva, I.P. Renin Activity in Heart Failure with Reduced Systolic Function—New Insights. Int. J. Mol. Sci. 2019, 20, 3182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacFadyen, R.J.; Barr, C.S.; Struthers, A.D. Aldosterone Blockade Reduces Vascular Collagen Turnover, Improves Heart Rate Variability and Reduces Early Morning Rise in Heart Rate in Heart Failure Patients. Cardiovasc. Res. 1997, 35, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heindl, S.; Holzschneider, J.; Hinz, A.; Sayk, F.; Fehm, H.L.; Dodt, C. Acute Effects of Aldosterone on the Autonomic Nervous System and the Baroreflex Function in Healthy Humans. J. Neuroendocrinol. 2006, 18, 115–121. [Google Scholar] [CrossRef]
- Kosmala, W.; Rojek, A.; Przewlocka-Kosmala, M.; Wright, L.; Mysiak, A.; Marwick, T.H. Effect of Aldosterone Antagonism on Exercise Tolerance in Heart Failure with Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2016, 68, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Giannitsi, S.; Bougiakli, M.; Bechlioulis, A.; Kotsia, A.; Michalis, L.K.; Naka, K.K. 6-Minute Walking Test: A Useful Tool in the Management of Heart Failure Patients. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719870084. [Google Scholar] [CrossRef] [Green Version]
- Hori, M.; Okamoto, H. Heart Rate as a Target of Treatment of Chronic Heart Failure. J. Cardiol. 2012, 60, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Spoletini, I.; Coats, A.J.S.; Piepoli, M.F.; Rosano, G.M.C. Heart Rate and Blood Pressure Monitoring in Heart Failure. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2019, 21 (Suppl. M), M13–M16. [Google Scholar] [CrossRef] [Green Version]
- Guzik, P.; Piskorski, J.; Wysocki, H.; Wykrętowicz, A. Prospective Observational Study on Predicting Adverse Clinical Outcomes in Patients with Implanted Defibrillating Devices—A Study Rationale, Design and Principal Methods. J. Med. Sci. 2014, 83, 84–88. [Google Scholar] [CrossRef]
- Sawicka-Gutaj, N.; Gruszczyński, D.; Guzik, P.; Mostowska, A.; Walkowiak, J. Publication Ethics of Human Studies in the Light of the Declaration of Helsinki—A Mini-Review. J. Med. Sci. 2022, 91, e700. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Popescu, B.A.; Andrade, M.J.; Badano, L.P.; Fox, K.F.; Flachskampf, F.A.; Lancellotti, P.; Varga, A.; Sicari, R.; Evangelista, A.; Nihoyannopoulos, P.; et al. European Association of Echocardiography Recommendations for Training, Competence, and Quality Improvement in Echocardiography. Eur. J. Echocardiogr. 2009, 10, 893–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wielemborek-Musial, K.; Szmigielska, K.; Leszczyńska, J.; Jegier, A. Blood Pressure Response to Submaximal Exercise Test in Adults. BioMed Res. Int. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Diniz, L.S.; Neves, V.R.; Starke, A.C.; Barbosa, M.P.T.; Britto, R.R.; Ribeiro, A.L.P. Safety of Early Performance of the Six-Minute Walk Test Following Acute Myocardial Infarction: A Cross-Sectional Study. Braz. J. Phys. Ther. 2017, 21, 167–174. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Stough, W.G.; Yancy, C.W.; Young, J.B.; Fonarow, G.C.; et al. Systolic Blood Pressure at Admission, Clinical Characteristics, and Outcomes in Patients Hospitalized With Acute Heart Failure. JAMA 2006, 296, 2217–2226. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.T.; Chen, J.; Cohen, D.J.; Tsao, L. The Association between Blood Pressure and Mortality in Patients with Heart Failure. Am. Heart J. 2006, 151, 76–83. [Google Scholar] [CrossRef]
- Ather, S.; Chan, W.; Chillar, A.; Aguilar, D.; Pritchett, A.M.; Ramasubbu, K.; Wehrens, X.H.T.; Deswal, A.; Bozkurt, B. Association of Systolic Blood Pressure with Mortality in Patients with Heart Failure with Reduced Ejection Fraction: A Complex Relationship. Am. Heart J. 2011, 161, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical Practice Update on Heart Failure 2019: Pharmacotherapy, Procedures, Devices and Patient Management. An Expert Consensus Meeting Report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Zannad, F.; Sopko, G.; Klein, L.; Piña, I.L.; Konstam, M.A.; Massie, B.M.; Roland, E.; Targum, S.; Collins, S.P.; et al. Acute Heart Failure Syndromes. Circulation 2005, 112, 3958–3968. [Google Scholar] [CrossRef]
- Borovac, J.A.; D’Amario, D.; Bozic, J.; Glavas, D. Sympathetic Nervous System Activation and Heart Failure: Current State of Evidence and the Pathophysiology in the Light of Novel Biomarkers. World J. Cardiol. 2020, 12, 373–408. [Google Scholar] [CrossRef] [PubMed]
- Triposkiadis, F.; Karayannis, G.; Giamouzis, G.; Skoularigis, J.; Louridas, G.; Butler, J. The Sympathetic Nervous System in Heart Failure Physiology, Pathophysiology, and Clinical Implications. J. Am. Coll. Cardiol. 2009, 54, 1747–1762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floras, J.S.; Ponikowski, P. The Sympathetic/Parasympathetic Imbalance in Heart Failure with Reduced Ejection Fraction. Eur. Heart J. 2015, 36, 1974–1982b. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepoli, M.F.; Coats, A.J.S. The “skeletal Muscle Hypothesis in Heart Failure” Revised. Eur. Heart J. 2013, 34, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Kulik, T.J. Pulmonary Hypertension Caused by Pulmonary Venous Hypertension. Pulm. Circ. 2014, 4, 581–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thrasher, T.N. Baroreceptor Regulation of Vasopressin and Renin Secretion: Low-Pressure versus High-Pressure Receptors. Front. Neuroendocrinol. 1994, 15, 157–196. [Google Scholar] [CrossRef]
- Olivetti, G.; Abbi, R.; Quaini, F.; Kajstura, J.; Cheng, W.; Nitahara, J.A.; Quaini, E.; Di Loreto, C.; Beltrami, C.A.; Krajewski, S.; et al. Apoptosis in the Failing Human Heart. N. Engl. J. Med. 1997, 336, 1131–1141. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Dimopoulos, K.; Concu, A.; Crisafulli, A. Cardiovascular and Ventilatory Control during Exercise in Chronic Heart Failure: Role of Muscle Reflexes. Int. J. Cardiol. 2008, 130, 3–10. [Google Scholar] [CrossRef]
- Keller-Ross, M.L.; Larson, M.; Johnson, B.D. Skeletal Muscle Fatigability in Heart Failure. Front. Physiol. 2019, 10, 129. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Francis, D.P.; Piepoli, M.F.; Davies, L.C.; Chua, T.P.; Davos, C.H.; Florea, V.; Banasiak, W.; Poole-Wilson, P.A.; Coats, A.J.; et al. Enhanced Ventilatory Response to Exercise in Patients with Chronic Heart Failure and Preserved Exercise Tolerance: Marker of Abnormal Cardiorespiratory Reflex Control and Predictor of Poor Prognosis. Circulation 2001, 103, 967–972. [Google Scholar] [CrossRef]
- Coats, A.J.; Adamopoulos, S.; Radaelli, A.; McCance, A.; Meyer, T.E.; Bernardi, L.; Solda, P.L.; Davey, P.; Ormerod, O.; Forfar, C. Controlled Trial of Physical Training in Chronic Heart Failure. Exercise Performance, Hemodynamics, Ventilation, and Autonomic Function. Circulation 1992, 85, 2119–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, Y.; Joho, S.; Harada, D.; Hirai, T.; Asanoi, H.; Inoue, H. Renal Insufficiency Coexisting with Heart Failure Is Related to Elevated Sympathetic Nerve Activity. Auton. Neurosci. Basic Clin. 2010, 155, 104–108. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| T1 and 2 n = 204 | T3 n = 102 | p-Value | |||
|---|---|---|---|---|---|
| Median | 25–75 P | Median | 25–75 P | ||
| Age, years | 63.24 | 57.94–68.58 | 65.73 | 57.15–73.96 | 0.1348 |
| BMI, kg/m2 | 28.31 | 25.43–31.0 | 27.94 | 24.51–31.37 | 0.6651 |
| NYHA class | 2.0 | 2.0–3.0 | 2.0 | 2.0–3.0 | 0.9373 |
| Weeks from ICD/CRT-D implantation | 17 | 5.0–30.0 | 19 | 9.0–34.00 | 0.2853 |
| Aldosterone, pg/mL | 133.5 | 106.00–158.50 | 263 | 229.00–337.00 | <0.0001 |
| Crea, mg/dL | 1.03 | 0.89–1.27 | 1.16 | 1.00–1.49 | 0.0001 |
| eGFRC-G, mL/min/1.73 m2 | 82.561 | 61.64–107.88 | 69.667 | 49.89–92.70 | 0.0016 |
| NT-proBNP, pg/mL | 811.9 | 374.40–2378.50 | 1145 | 485.30–2783.00 | 0.0425 |
| K, mmol/L | 4.52 | 4.27–4.78 | 4.495 | 4.30–4.87 | 0.9676 |
| Na, mmol/L | 141 | 139.00–143.00 | 140 | 138.00–142.00 | 0.0006 |
| LVEDD, mm | 60.6 | 55.0–66.95 | 63.2 | 57.30–71.20 | 0.0581 |
| LVESD, mm | 50.9 | 44.60–58.85 | 54.25 | 45.90–61.50 | 0.0583 |
| LA, mm | 43.15 | 39.30–47.60 | 45.85 | 39.70–50.30 | 0.0315 |
| RV, mm | 27.8 | 25.40–31.60 | 29.15 | 26.20–32.90 | 0.0385 |
| IVT, mm | 11.1 | 9.75–12.35 | 11.2 | 9.60–12.70 | 0.911 |
| LVPWT, mm | 11.6 | 10.20–13.20 | 11.25 | 9.60–13.20 | 0.3759 |
| E/A ratio | 0.78 | 0.60–1.55 | 1.018 | 0.60–2.23 | 0.1308 |
| E/e’ ratio | 8.13 | 5.85–11.20 | 8.53 | 5.62–11.84 | 0.7131 |
| E-wave velocity, cm/s | 62.5 | 49.50–92.00 | 67 | 47.75–96.25 | 0.4113 |
| LVEF, % | 30.93 | 23.39–37.44 | 30.93 | 21.33–36.72 | 0.4371 |
| Distance, m | 480 | 384.00–544.00 | 432 | 320.00–512.00 | 0.0303 |
| RPE | 12 | 10.00–15.00 | 12 | 10.00–15.00 | 0.7746 |
| Resting SpO2, % | 96 | 95.00–97.00 | 96 | 95.00–98.00 | 0.2715 |
| T1 and 2 | T3 | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Men | 177 | 86.8 | 86 | 84.3 | 0.5615 |
| Ischaemic aetiology | 103 | 50.5 | 37 | 36.3 | 0.0188 |
| Hypertension | 167 | 81.9 | 83 | 81.4 | 0.9169 |
| Diabetes mellitus type 2 | 71 | 34.8 | 35 | 34.3 | 0.9324 |
| Current smoker status | 32 | 15.7 | 13 | 12.7 | 0.0659 |
| Stroke/TIA | 20 | 9.8 | 10 | 9.8 | 1.0000 |
| Permanent AF | 42 | 20.6 | 24 | 23.5 | 0.6086 |
| NYHA III/IV | 70 | 34.3 | 36 | 35.3 | 0.8653 |
| Primary/Secondary | 38 | 18.6 | 13 | 12.7 | 0.1938 |
| CRT-D | 80 | 39.2 | 53 | 52.0 | 0.0343 |
| ACE or ARBs | 170 | 83.3 | 83 | 81.4 | 0.6697 |
| Beta-blocker | 176 | 86.3 | 85 | 83.3 | 0.4942 |
| Spironolactone | 123 | 60.3 | 78 | 76.5 | 0.0050 |
| Diuretic | 164 | 80.4 | 94 | 92.2 | 0.0077 |
| Statin | 163 | 79.9 | 81 | 79.4 | 0.9200 |
| Digoxin | 15 | 7.4 | 10 | 9.8 | 0.4613 |
| Nitrate | 23 | 11.3 | 7 | 6.9 | 0.2219 |
| Antiplatelet drug | 155 | 76.0 | 78 | 76.5 | 0.9246 |
| Amiodarone | 43 | 21.2 | 23 | 22.5 | 0.7685 |
| Insulin | 17 | 8.3 | 7 | 6.9 | 0.6525 |
| T1 and 2 | T3 | p-Value | |||
|---|---|---|---|---|---|
| Median | (25–75P) | Median | (25–75P) | ||
| SBPrest, mmHg | 136.00 | 121.00–148.00 | 127.00 | 115.00–143.00 | 0.005 |
| SBPend, mmHg | 144.00 | 126.00–160.00 | 139.00 | 121.00–152.00 | 0.0147 |
| SBPrecov-1′, mmHg | 141.00 | 125.00–156.00 | 130.00 | 117.00–146.25 | 0.0008 |
| SBPrecov-3′, mmHg | 137.00 | 124.50–154.00 | 133.00 | 112.75–143.25 | 0.0013 |
| DBPrest, mmHg | 84.50 | 77.00–92.00 | 81.00 | 71.00–89.00 | 0.0082 |
| DBPend, mmHg | 88.00 | 80.00–95.50 | 84.00 | 74.00–93.00 | 0.0235 |
| DBPrecov-1′, mmHg | 87.00 | 80.00–95.00 | 81.00 | 74.00–94.00 | 0.0012 |
| DBPrecov-3′, mmHg | 86.00 | 79.00–94.00 | 83.00 | 73.00–90.00 | 0.0017 |
| MBPrest, mmHg | 101.50 | 93.17–111.83 | 97.00 | 87.33–105.67 | 0.0036 |
| MBPend, mmHg | 106.50 | 97.33–117.00 | 102.00 | 91.67–111.67 | 0.0099 |
| MBPrecov-1′, mmHg | 105.00 | 95.50–114.50 | 97.17 | 89.00–109.00 | 0.0001 |
| MBPrecov-3′, mmHg | 104.33 | 95.17–113.67 | 96.50 | 87.00–106.33 | 0.0001 |
| PPrest, mmHg | 50.00 | 40.00–60.00 | 46.00 | 37.00–57.00 | 0.1324 |
| PPend, mmHg | 55.00 | 40.00–66.50 | 52.00 | 39.00–61.00 | 0.1687 |
| PPrecov-1′, mmHg | 51.50 | 41.00–63.00 | 47.00 | 36.00–60.00 | 0.0465 |
| PPrecov-3′, mmHg | 50.00 | 39.00–61.50 | 47.50 | 35.00–58.00 | 0.086 |
| HRrest, mmHg | 71.00 | 64.00–78.00 | 71.00 | 65.00–81.00 | 0.6297 |
| HRend, mmHg | 89.00 | 76.50–101.50 | 85.00 | 77.00–100.00 | 0.5114 |
| HRrecov-1′, mmHg | 76.00 | 69.00–87.50 | 76.00 | 68.00–88.50 | 0.9571 |
| HRrecov-3′, mmHg | 72.50 | 66.50–84.00 | 75.00 | 68.00–86.00 | 0.4278 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miętkiewska-Szwacka, K.; Krauze, T.; Barecka, K.; Różańska-Kirschke, A.; Przymuszała-Staszak, D.; Schneider, A.; Dziarmaga, M.; Tarchalski, J.L.; Nowak, A.; Bryl, M.; et al. Comparison of Hemodynamic Response between Patients with Systolic Heart Failure Differing in Serum Aldosterone Concentrations during and after a 6-Minute Walk Test. J. Clin. Med. 2023, 12, 1007. https://doi.org/10.3390/jcm12031007
Miętkiewska-Szwacka K, Krauze T, Barecka K, Różańska-Kirschke A, Przymuszała-Staszak D, Schneider A, Dziarmaga M, Tarchalski JL, Nowak A, Bryl M, et al. Comparison of Hemodynamic Response between Patients with Systolic Heart Failure Differing in Serum Aldosterone Concentrations during and after a 6-Minute Walk Test. Journal of Clinical Medicine. 2023; 12(3):1007. https://doi.org/10.3390/jcm12031007
Chicago/Turabian StyleMiętkiewska-Szwacka, Kamila, Tomasz Krauze, Katarzyna Barecka, Anna Różańska-Kirschke, Dagmara Przymuszała-Staszak, Agata Schneider, Miłosz Dziarmaga, Jacek Lech Tarchalski, Aneta Nowak, Mateusz Bryl, and et al. 2023. "Comparison of Hemodynamic Response between Patients with Systolic Heart Failure Differing in Serum Aldosterone Concentrations during and after a 6-Minute Walk Test" Journal of Clinical Medicine 12, no. 3: 1007. https://doi.org/10.3390/jcm12031007