
Accelerometry in the Functional Assessment of Balance in People with Stroke: A Systematic Review



Abstract
:1. Introduction
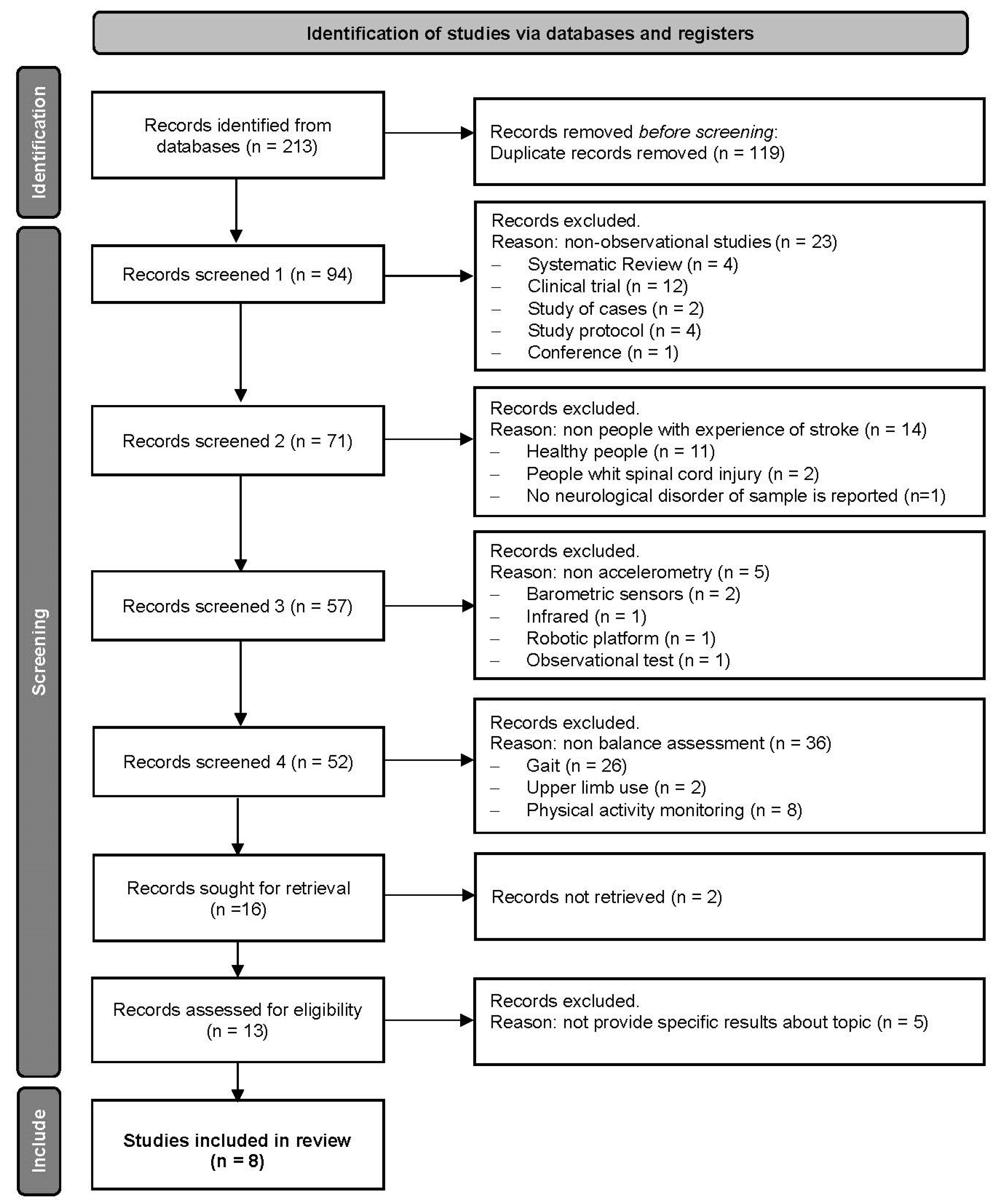
2. Methods
3. Results
3.1. Study Design
3.2. Participants
3.3. Balance Evaluation Methods
3.4. Outcome Variables
3.5. Signal Processing
3.6. Result of Studies
3.7. Risk of Bias Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 10MWT | 10-Meter Walk Test |
| AP | Antero-posterior |
| BBS | Berg Balance Scale |
| BI | Barthel Index |
| BVS | Virtual Health Library from Spain |
| CTSIB | Clinical Test of Sensory Interaction and Balance |
| FAC | Functional Ambulation Classification scale |
| FRT | Functional Reach Test |
| FST | Fukuda Stepping Test |
| ICC | Intraclass correlation coefficient |
| IMU | Inertial measurement units |
| MeSH | Medical Subject Headings |
| ML | Medio-lateral |
| PEDro | Physiotherapy Evidence Database |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| RMS | Root Mean Square |
| SLS | Sigl-Leg Stance Test |
| TUG | Timed Up and Go Test |
| WHO | World Health Organization |
| WOS | Web of Science |
References
- World Health Organization. Neurological Disorders: Public Health Challenges; World Health Organization: Geneva, Switzerland, 2006; ISBN 978-92-4-156336-9. [Google Scholar]
- Purroy, F.; Montalà, N. Epidemiology of Stroke in the Last Decade: A Systematic Review. Rev. Neurol. 2021, 73, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Krafft, P.R.; Bailey, E.L.; Lekic, T.; Rolland, W.B.; Altay, O.; Tang, J.; Wardlaw, J.M.; Zhang, J.H.; Sudlow, C.L.M. Etiology of Stroke and Choice of Models. Int. J. Stroke 2012, 7, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Chevidikunnan, M.F. Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study. Healthcare 2021, 9, 320. [Google Scholar] [CrossRef] [PubMed]
- Gorst, T.; Rogers, A.; Morrison, S.C.; Cramp, M.; Paton, J.; Freeman, J.; Marsden, J. The Prevalence, Distribution, and Functional Importance of Lower Limb Somatosensory Impairments in Chronic Stroke Survivors: A Cross Sectional Observational Study. Disabil. Rehabil. 2019, 41, 2443–2450. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor Recovery after Stroke: A Systematic Review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, P. Upper Limb Motor Impairment After Stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S.; Sarkar, B. Reliability, Validity, and Responsiveness of Three Scales for Measuring Balance in Patients with Chronic Stroke. BMC Neurol. 2018, 18, 141. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Lin, S.-F.; Yu, W.-H.; Lin, J.-H.; Chen, H.-L.; Hsieh, C.-L. Comparison of the Test-Retest Reliability of the Balance Computerized Adaptive Test and a Computerized Posturography Instrument in Patients with Stroke. Arch. Phys. Med. Rehabil. 2014, 95, 1477–1483. [Google Scholar] [CrossRef]
- Domènech-Vadillo, E.; Aguilera-Aguilera, G.; Sánchez-Blanco, C.; Batuecas-Caletrio, Á.; Guajardo, C.; Pérez, N.; Trinidad-Ruiz, G.; Gimeno, C.; Rama, J.; Rossi-Izquierdo, M.; et al. Normative Data for Static Balance Testing in Healthy Individuals Using Open Source Computerized Posturography. Eur. Arch. Otorhinolaryngol. 2019, 276, 41–48. [Google Scholar] [CrossRef]
- Visser, J.E.; Carpenter, M.G.; van der Kooij, H.; Bloem, B.R. The Clinical Utility of Posturography. Clin. Neurophysiol. 2008, 119, 2424–2436. [Google Scholar] [CrossRef]
- Wang, Q.; Markopoulos, P.; Yu, B.; Chen, W.; Timmermans, A. Interactive Wearable Systems for Upper Body Rehabilitation: A Systematic Review. J. NeuroEng. Rehab. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of Accelerometer Methods for Physical Activity Research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-H.; Sun, T.-L.; Jiang, B.C.; Choi, V.H. Using Wearable Accelerometers in a Community Service Context to Categorize Falling Behavior. Entropy 2016, 18, 257. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; García-Soidán, J.L.; Romo-Pérez, V. Analyzing the Use of Accelerometers as a Method of Early Diagnosis of Alterations in Balance in Elderly People: A Systematic Review. Sensors 2019, 19, 3883. [Google Scholar] [CrossRef] [PubMed]
- Johansson, D.; Malmgren, K.; Alt Murphy, M. Wearable Sensors for Clinical Applications in Epilepsy, Parkinson’s Disease, and Stroke: A Mixed-Methods Systematic Review. J. Neurol. 2018, 265, 1740–1752. [Google Scholar] [CrossRef] [PubMed]
- Similä, H.; Immonen, M.; Ermes, M. Accelerometry-Based Assessment and Detection of Early Signs of Balance Deficits. Comput. Biol. Med. 2017, 85, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Ciapponi, A. QUADAS-2: Instrumento para la evaluación de la calidad de estudios de precisión diagnóstica. Evid. Actual. Práctica Ambulatoria 2015, 18, 1. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Perez-Cruzado, D.; González-Sánchez, M.; Cuesta-Vargas, A.I. Parameterization and Reliability of Single-Leg Balance Test Assessed with Inertial Sensors in Stroke Survivors: A Cross-Sectional Study. Biomed. Eng. 2014, 13, 127. [Google Scholar] [CrossRef]
- Hou, Y.-R.; Chiu, Y.-L.; Chiang, S.-L.; Chen, H.-Y.; Sung, W.-H. Feasibility of a Smartphone-Based Balance Assessment System for Subjects with Chronic Stroke. Comput. Methods Programs Biomed. 2018, 161, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A.I. Reliability in the Parameterization of the Functional Reach Test in Elderly Stroke Patients: A Pilot Study. BioMed Res. Int. 2014, 2014, 637671. [Google Scholar] [CrossRef] [PubMed]
- Wüest, S.; Massé, F.; Aminian, K.; Gonzenbach, R.; de Bruin, E.D. Reliability and Validity of the Inertial Sensor-Based Timed “Up and Go” Test in Individuals Affected by Stroke. J. Rehabil. Res. Dev. 2016, 53, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.-R.; Chiu, Y.-L.; Chiang, S.-L.; Chen, H.-Y.; Sung, W.-H. Development of a Smartphone-Based Balance Assessment System for Subjects with Stroke. Sensors 2019, 20, 88. [Google Scholar] [CrossRef]
- Chung, J.; Kim, S.; Yang, Y. Correlation between Accelerometry and Clinical Balance Testing in Stroke. J. Phys. Ther. Sci. 2016, 28, 2260–2263. [Google Scholar] [CrossRef]
- Belluscio, V.; Bergamini, E.; Iosa, M.; Tramontano, M.; Morone, G.; Vannozzi, G. The iFST: An Instrumented Version of the Fukuda Stepping Test for Balance Assessment. Gait Posture 2018, 60, 203–208. [Google Scholar] [CrossRef]
- Na, E.; Hwang, H.; Woo, Y. Study of Acceleration of Center of Mass during Sit-to-Stand and Stand-to-Sit in Patients with Stroke. J. Phys. Ther. Sci. 2016, 28, 2457–2460. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.; Gough, C.; Gordon, S. Classification of Balance Assessment Technology: A Scoping Review of Systematic Reviews. Stud. Health Technol. Inform. 2020, 268, 45–59. [Google Scholar] [CrossRef]
- Bruyneel, A.-V.; Dubé, F. Best Quantitative Tools for Assessing Static and Dynamic Standing Balance after Stroke: A Systematic Review. Physiother. Can. 2021, 73, 329–340. [Google Scholar] [CrossRef]
- Clark, E.; Podschun, L.; Church, K.; Fleagle, A.; Hull, P.; Ohree, S.; Springfield, M.; Wood, S. Use of Accelerometers in Determining Risk of Falls in Individuals Post-Stroke: A Systematic Review. Clin. Rehabil. 2023, 37, 1467–1478. [Google Scholar] [CrossRef]
- Kim, T.J.; Seo, K.M.; Kim, D.-K.; Kang, S.H. The Relationship between Initial Trunk Performances and Functional Prognosis in Patients with Stroke. Ann. Rehabil. Med. 2015, 39, 66–73. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PUBMED | RESULTS |
| #1 “Accelerometry” [MeSH] | 11,296 |
| #2 “Accelerometry” [Title/Abstract] | 5351 |
| #3 “Acelerom *” [Title/Abstract] | 20,923 |
| #4 #1 OR #2 OR #3 | 25,657 |
| #5 “Stroke” [MeSH] | 158,593 |
| #6 “Stroke” [Title/Abstract] | 282,951 |
| #7 #5 OR #6 | 322,672 |
| #8 “Outcome and Process Assessment, Health Care” [MeSH] | 1,311,980 |
| #9 “Assessment” | 1,602,783 |
| #10 #8 OR #9 | 2,648,945 |
| #11 “Postural Balance” [MeSH] | 26,759 |
| #12 “Balance” [Title/Abstract] | 254,645 |
| #13 #11 OR #12 | 266,277 |
| #14 #4 AND #7 AND #10 AND #13 | 28 |
| #15 Limit #14 TO: published in the last 10 years | 21 |
| Total PUBMED results | 21 |
| SCOPUS | RESULTS |
| #1 “Accelerom *” [Title-Abstract-Keywords] | 70,031 |
| #2 “Stroke” [Title-Abstract-Keywords] | 482,261 |
| #3 “Balance” [Title-Abstract-Keywords] | 876,153 |
| #4 #1 AND #2 AND #3 | 75 |
| #5 Limit #4 TO: published in the last 10 years | 60 |
| Total SCOPUS results | 60 |
| WEB OF SCIENCE | RESULTS |
| #1 “Accelerom *” [Topic] | 52,046 |
| #2 “Stroke” [Topic] | 405,619 |
| #3 “Balance” [Topic] | 620,526 |
| #4 #1 AND #2 AND #3 | 90 |
| #5 Refined #4 By: Publication Years: 2022 or 2021 or 2020 or 2019 or 2018 or 2017 or 2016 or 2015 or 2014 or 2013 | 69 |
| Total WOS results | 69 |
| COCHRANE LIBRARY | RESULTS |
| #1 “Accelerometry” [MeSH descriptor] | 1075 |
| #2 “Accelerom *” | 1 |
| #3 #1 OR #2 | 1076 |
| #4 “Stroke” [MeSH descriptor] | 11,217 |
| #5 “Stroke” | 75,606 |
| #6 #4 OR #5 | 75,901 |
| #7 “Postural Balance” [MeSH descriptor] | 3120 |
| #8 “Balance” | 30,553 |
| #9 #7 OR #8 | 30,555 |
| #10 #3 AND #6 AND #9 | 3 |
| #11 Limit #10 TO: published in the last 10 years | 3 |
| Total, COCHRANE LIBRARY results | 3 |
| PEDro | RESULTS |
| #1 Accelerom * Stroke Balance | 2 |
| Total PEDro results | 2 |
| BVS Spain | RESULTS |
| Stroke AND Accelerom * AND Balance | 58 |
| Total, BVS results | 58 |
| Author and Year | Population (Women/Men) | Accelerometer Type | Accelerometer Location | Variable Measured | Psychometric Properties of the Accelerometer Analyzed | Results |
|---|---|---|---|---|---|---|
| Hou et al. (2019) [25] | 19 | Accelerometer of the ASUS Zenfone 3 smartphone | S2 vertebra | Displacement of the center of gravity in the base of support | Reliability and validity of a proprietary scale and comparison BBS | In the reliability test, in which healthy subjects participated, the intraclass correlation coefficient (ICC) of the accelerometer was 0.904 within-day and 0.764 between-days, indicating excellent reliability. In the validity test, in the accelerometer data, no statistically significant differences were observed between healthy subjects and subjects with stroke in the six tests (p = 0.007–0.65). The criterion validity test did not show significant correlations between the accelerometer and the BBS, obtaining p-values between 0.053 and 0.723. |
| Hou et al. (2018) [22] | 23 (9/14) | Accelerometer of the HTC 10 smartphone | S2 vertebra | Changes in acceleration of the center of gravity at the base of support | Validity of a proprietary scale | Significant differences were found between stroke subjects and healthy subjects in four test postures, with p-values between 0.000 and 0.048. |
| Belluscio et al. (2018) [27] | 18 (12/6) | Opal (IMU) (APDM Inc., Portland, OR, USA) | Occipital, sternum, L4–L5 vertebrae and both external malleoli | Linear accelerations (ML, AP and rotation) during the FST | Validity during the FST | No significant differences were found in the magnitude of body rotation and AP/ML displacement between stroke patients classified 3–4 in the FAC and healthy people, showing that the FST parameters are not capable of distinguishing between healthy and pathological subjects. |
| Na et al. (2016) [28] | 60 (30/30) | Tri-axial accelerometer (G-Walk; BTS Bioengineering S.p.A., Italy) | L5 vertebra | Phase duration (s), AP, ML and VP acceleration range (m/s2), | Validity during the sit-to-stand and stand-to-sit transition of TUG | significant differences (p < 0.05) between patients with stroke and healthy subjects were found in the phase duration and the AP, ML, and VT acceleration ranges sit-to-stand. And in duration m (p < 0.05) and ML acceleration range (p < 0.001) stand-to-sit and phase. |
| Wüest et al. (2016) [24] | 39 (19/20) | Physilog (GaitUp, Lausanne, Switzerland) | Both wrists, both legs, thoracic spine, both feet and L3 vertebra | Total time, sit-to-gait transfer, gait characteristics, turn, turn-to-sit transfer | Reliability and validity during the sit-to-stand and stand-to-sit transition of TUG | In the reliability test, of the 14 TUG metrics analyzed, 12 variables showed excellent test–retest reliability (ICC = 0.855–0.994). Regarding validity and taking time into consideration, there was a statistically significant difference between the two groups (p = 0.002). Of the 13 parameters analyzed, 8 showed a significant difference between groups (p = 0.000–0.02). In addition, 11 of the 14 parameters analyzed showed a low standard error of measurement and low minimum detectable difference. |
| Chung et al. (2016) [26] | 27 (6/21) | Trigno™ Wireless Electromyography System (Delsys Inc., Boston, MA, USA) | Postural sway | Validity during the CTSIB and a comparison with BBS | A significant correlation (p < 0.05) was found between the left–right and forward–backward accelerometry measures of the CTSIB with the BBS scores. Moreover, it showed a significant correlation between the acceleration of condition 3 of the CTSIB and the total score of the BBS (correlates p < 0.05). | |
| Pérez-Cruzado et al. (2014) [21] | 4 | InertiaCube3TM (InterSense Inc., Bedford, MA, USA) | T7–T8 and L5–S1 vertebrae | Variables of movement and speed of the trunk in rotation, flexion/extension and inclination | Reliability during the SLS | The ICC showed values over 0.847 for all the variables, both interobserver and intraobserver in both devices. Therefore, reliability showed excellent values for displacement and speed. Furthermore, significant differences in location were only found in 2 of the 68 variables measured, so the location of the sensors for the SLS between the upper trunk and the lower back would not be relevant. |
| Merchán-Baeza et al. (2014) [23] | 4 | InertiaCube3TM (InterSense Inc., Bedford, MA, USA) | L5–S1 and T7 vertebrae | Variables of trunk displacement and time | Reliability during the FRT | The within-subject reliability values observed in the use of inertial sensors were all above 0.820 (ICC = 0.829–0.891). The observed between-subject ICC values ranged from 0.821 to 0.883. Therefore, the intra- and intersubject reliability could be categorized as excellent. On the other hand, the intersubject and intrasubject reliability of the FRT was 0.987 (0.983–0.992) and 0.983 (0.979–0.989), respectively, being excellent in both cases. The levels of reliability observed could be categorized as excellent based on the results for intraobserver reliability (ICC = 0.829–0.878) and interobserver reliability (ICC = 0.821–0.883). In addition, it showed differences between the data provided by the sensors in the lower back with respect to the rest of the trunk when performing the FRT. |
| Authors | Bias Probability | Concerns Regarding Applicability of Results | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Times | Patient Selection | Index Test | Reference Standard | |
| Pérez-Cruzado et al. [21] | High | Unclear | High | Low | Low | Low | High |
| Hou et al. [22] | High | Unclear | High | Low | Low | Unclear | High |
| Merchán-Baeza et al. [23] | High | Unclear | High | Low | Low | Low | High |
| Wüest et al. [24] | High | Unclear | High | Low | Low | Low | High |
| Hou et al. [25] | High | Unclear | Low | Low | Low | High | Low |
| Chung et al. [26] | High | Unclear | Unclear | Unclear | Low | Low | Low |
| Belluscio et al. [27] | High | Unclear | High | Low | Low | High | High |
| Na et al. [28] | High | Unclear | Low | Low | Low | Low | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-López, J.F.; Cano-de-la-Cuerda, R.; Ortiz-Gutiérrez, R.M. Accelerometry in the Functional Assessment of Balance in People with Stroke: A Systematic Review. J. Clin. Med. 2023, 12, 7701. https://doi.org/10.3390/jcm12247701
Pérez-López JF, Cano-de-la-Cuerda R, Ortiz-Gutiérrez RM. Accelerometry in the Functional Assessment of Balance in People with Stroke: A Systematic Review. Journal of Clinical Medicine. 2023; 12(24):7701. https://doi.org/10.3390/jcm12247701
Chicago/Turabian StylePérez-López, Juan Francisco, Roberto Cano-de-la-Cuerda, and Rosa María Ortiz-Gutiérrez. 2023. "Accelerometry in the Functional Assessment of Balance in People with Stroke: A Systematic Review" Journal of Clinical Medicine 12, no. 24: 7701. https://doi.org/10.3390/jcm12247701