
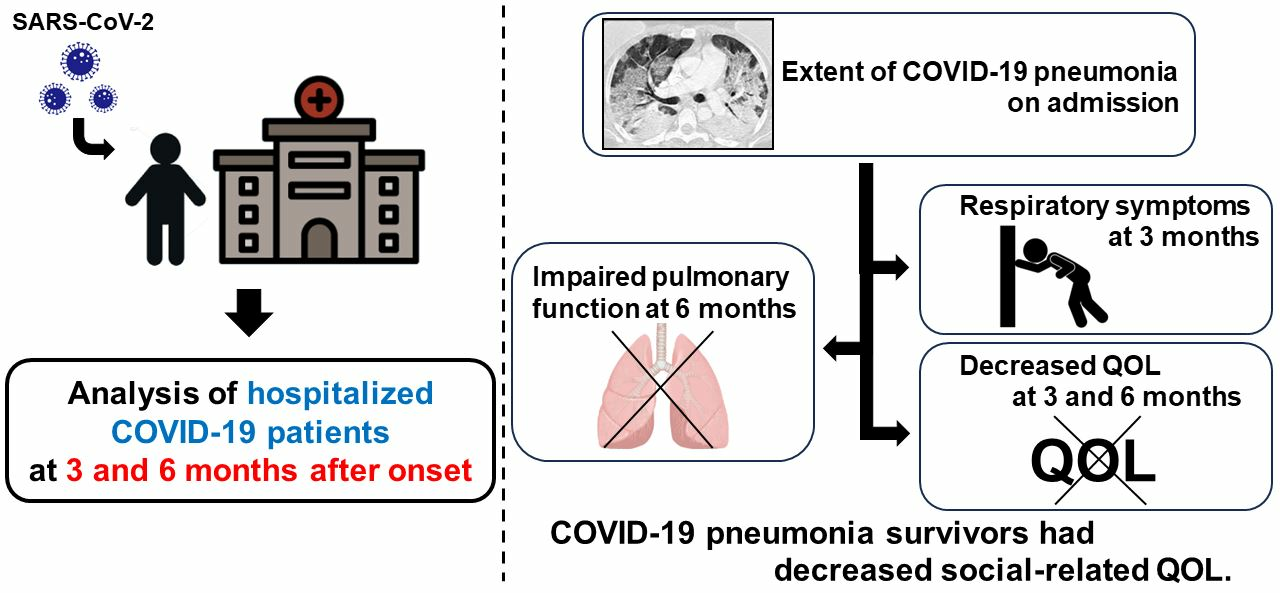
Impairment of Social-Related Quality of Life in COVID-19 Pneumonia Survivors: A Prospective Longitudinal Study

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
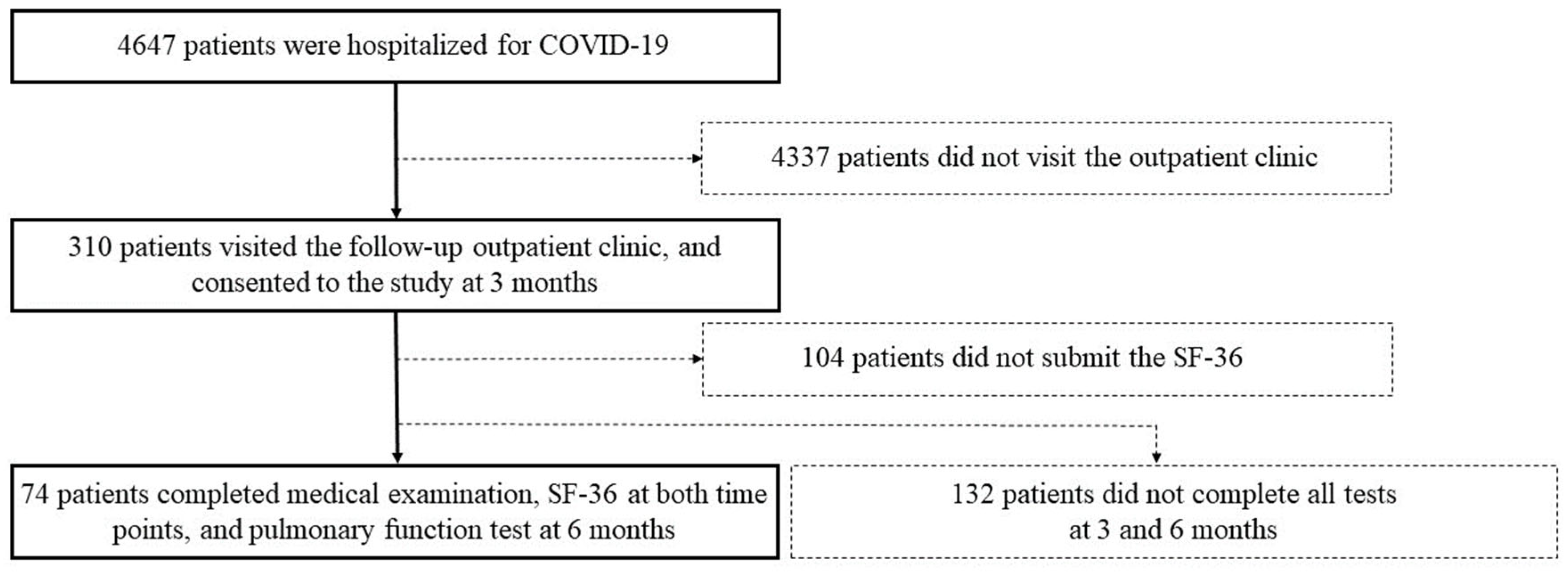
2.1. Study Design and Participants
2.2. Procedures
3. Measures
3.1. SF-36 Questionnaire
3.2. Chest CT Evaluation
3.3. Pulmonary Function Tests
4. Data Analysis
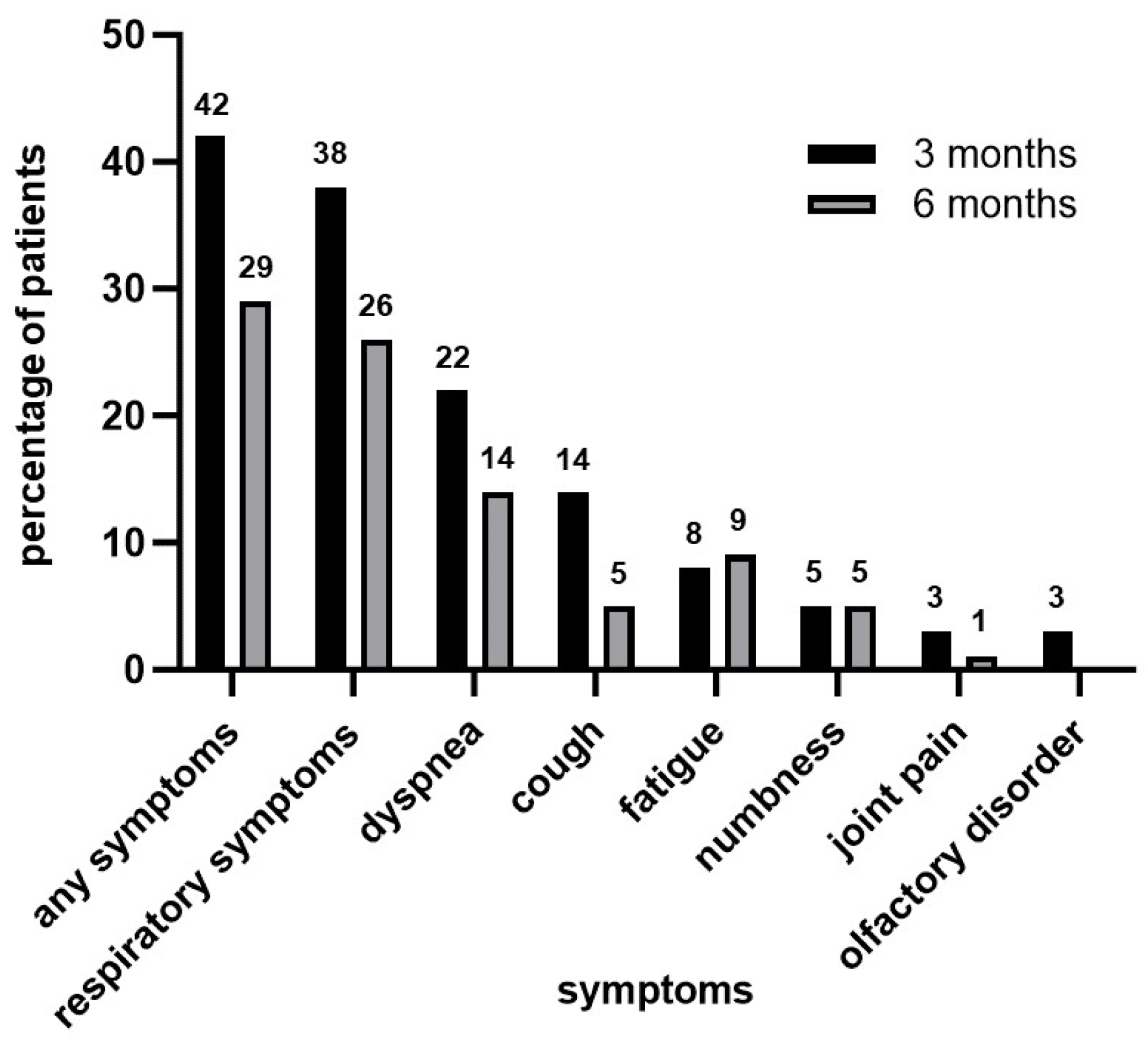
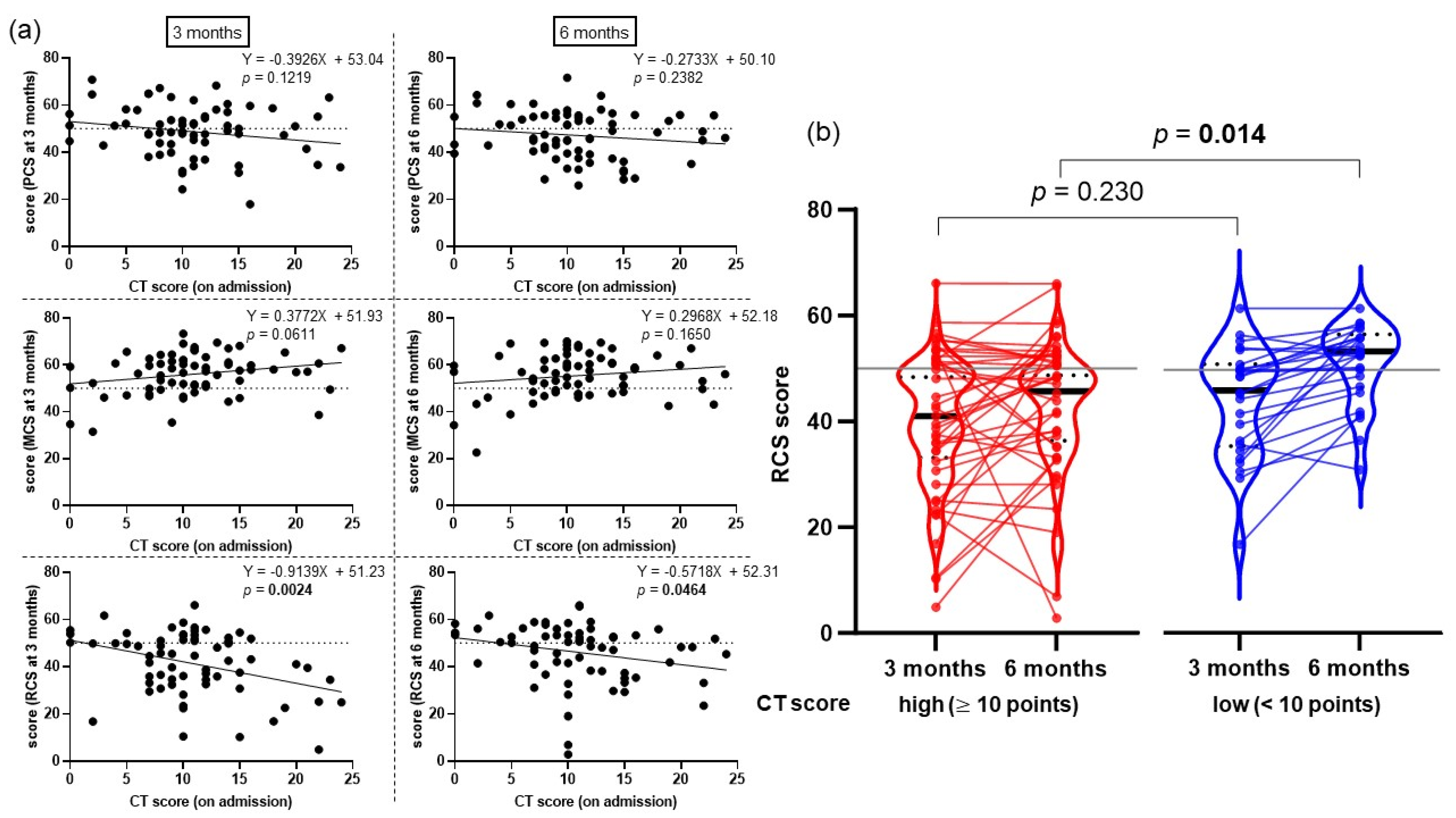
5. Results
6. Discussion
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 20 October 2023).
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Wang, C.; Liu, B.; Zhang, S.; Huang, N.; Zhao, T.; Lu, Q.B.; Cui, F. Differences in incidence and fatality of COVID-19 by SARS-CoV-2 Omicron variant versus Delta variant in relation to vaccine coverage: A world-wide review. J. Med. Virol. 2022, 95, 1. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 20 October 2023).
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated with Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef]
- Tarraso, J.; Safont, B.; Carbonell-Asins, J.A.; Fernandez-Fabrellas, E.; Sancho-Chust, J.N.; Naval, E.; Amat, B.; Herrera, S.; Ros, J.A.; Soler-Cataluna, J.J.; et al. Lung function and radiological findings 1 year after COVID-19: A prospective follow-up. Respir. Res. 2022, 23, 242. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Health-Related Quality of Life (HRQOL) Concepts. Available online: https://www.cdc.gov/hrqol/concept.htm (accessed on 20 October 2023).
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Poudel, A.N.; Zhu, S.; Cooper, N.; Roderick, P.; Alwan, N.; Terrant, C.; Ziauddeen, N.; Yao, G.L. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS ONE 2021, 16, e0259164. [Google Scholar] [CrossRef]
- O’Brien, K.; Townsend, L.; Dowds, J.; Bennan, C.; Nadarajan, P.; Kent, B.; Murphy, N.; Sheill, G.; Martin-Loeches, I.; Guinan, E. 1-year quality of life and health-outcomes in patients hospitalised with COVID-19: A longitudinal cohort study. Respir. Res. 2022, 23, 115. [Google Scholar] [CrossRef] [PubMed]
- Magdy, D.M.; Metwally, A.; Tawab, D.A.; Hassan, S.A.; Makboul, M.; Farghaly, S. Long-term COVID-19 effects on pulmonary function, exercise capacity, and health status. Ann. Thorac. Med. 2022, 17, 28–36. [Google Scholar] [CrossRef]
- Chen, K.-Y.; Li, T.; Gong, F.-H.; Zhang, J.-S.; Li, X.-K. Predictors of Health-Related Quality of Life and Influencing Factors for COVID-19 Patients, a Follow-Up at One Month. Front. Psychiatry 2020, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Corona, C.; Gutierrez-Canales, L.G.; Ortiz-Ledesma, C.; Martinez-Navarro, L.J.; Marcias, A.E.; Scavo-Montes, D.A.; Guani-Guerra, E. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J. Int. Med. Res. 2022, 50, 3000605221110492. [Google Scholar] [CrossRef] [PubMed]
- Segura-Ortí, E.; Martinez-Olmos, F.J.; Rodenas-Pascual, A.; Guillem-Gimenez, E.; Vercher-Narbona, V.; Pinon-Ruiz, M.J.; Garcia-Testal, A. Impact of COVID-19 Pandemic on Health-Related Quality of Life and Physical Activity of Patients in Hemodialysis. Healthcare 2022, 10, 2217. [Google Scholar] [CrossRef] [PubMed]
- van den Borst, B.; Peter, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive Health Assessment 3 Months After Recovery from Acute Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e1089–e1098. [Google Scholar] [CrossRef]
- Kersten, J.; Wolf, A.; Hoyo, L.; Hull, E.; Tadic, M.; Andreß, S.; d’Almeida, S.; Scharnbeck, D.; Roder, E.; Beschoner, P.; et al. Symptom burden correlates to impairment of diffusion capacity and exercise intolerance in long COVID patients. Sci. Rep. 2022, 12, 8801. [Google Scholar] [CrossRef]
- Suzukamo, Y.; Fukuhara, S.; Green, J.; Kosinski, M.; Gandek, B.; Ware, J.E., Jr. Validation testing of a three-component model of Short Form-36 scores. J. Clin. Epidemiol. 2011, 64, 301–308. [Google Scholar] [CrossRef]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef]
- Fukuhara, S.; Ware, J.E., Jr.; Kosinski, M.; Wada, S.; Gandek, B. Psychometric and clinical tests of validity of the Japanese SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1045–1053. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Yu, C.-J.; Chang, S.-C.; Galvin, J.-R.; Liu, H.-M.; Hsiao, C.-H.; Kuo, P.-H.; Chen, K.-Y.; Franks, T.-J.; Huang, K.-M.; et al. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: Evaluation with thin-section CT. Radiology 2005, 236, 1067–1075. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; Maclntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600016. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, A.; Miwata, K.; Kitahara, Y.; Okimoto, M.; Abe, K.; Bunthen, E.; Ouoba, S.; Akita, T.; Tanimine, N.; Ohdan, H.; et al. Long COVID occurrence in COVID-19 survivors. Sci. Rep. 2022, 12, 6039. [Google Scholar] [CrossRef] [PubMed]
- Terai, H.; Ishii, M.; Takemura, R.; Namkoong, H.; Shimamoto, K.; Masaki, K.; Tanosaki, T.; Chubachi, S.; Matsuyama, E.; Hayashi, R.; et al. Comprehensive analysis of long COVID in a Japanese nationwide prospective cohort study. Respir. Investig. 2023, 61, 802–814. [Google Scholar] [CrossRef]
- Rodríguez-Galán, I.; Albaladejo-Blazquez, N.; Ruiz-Robledillo, N.; Pascual-Liedo, J.F.; Ferrer-Cascales, R.; Gil-Carbonell, J. Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample. Int. J. Environ. Res. Public Health 2022, 19, 10421. [Google Scholar] [CrossRef] [PubMed]
- Rass, V.; Ianosi, B.A.; Zamarian, L.; Beer, R.; Sahanic, S.; Lindner, A.; Kofler, M.; Schiefecker, A.J.; Mahlknecht, P.; Heim, B.; et al. Factors associated with impaired quality of life three months after being diagnosed with COVID-19. Qual. Life Res. 2022, 31, 1401–1414. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Mackowiak, J.I. Evaluation of the short-form 36-item questionnaire to measure health-related quality of life in patients with COPD. Chest 1995, 107, 1585–1589. [Google Scholar] [CrossRef]
- Martinez, T.Y.; Pereira, C.A.; dos Santos, M.L.; Ciconelli, R.M.; Guimaraes, S.M.; Martinez, J.A. Evaluation of the short-form 36-item questionnaire to measure health-related quality of life in patients with idiopathic pulmonary fibrosis. Chest 2000, 117, 1627–1632. [Google Scholar] [CrossRef]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 253–262. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-Term Respiratory and Neurological Sequelae of COVID-19. Med. Sci. Monit. 2020, 26, e928996. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Baricich, A.; Patrucco, F.; Zeppegno, P.; Gramaglia, C.; Balbo, P.E.; Carriero, A.; Amico, C.S.; Avanzi, G.C.; Barini, M.; et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci. Rep. 2021, 11, 22666. [Google Scholar] [CrossRef] [PubMed]
- Froidure, A.; Mahsouli, A.; Liistro, G.; De Greef, J.; Belkhir, L.; Gerad, L.; Bertrand, A.; Koenig, S.; Pothen, L.; Yildiz, H.; et al. Integrative respiratory follow-up of severe COVID-19 reveals common functional and lung imaging sequelae. Respir. Med. 2021, 181, 106383. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, W.; Qurashi, A. Effectiveness of COVID-19 diagnosis and management tools: A review. Radiography 2021, 27, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef] [PubMed]
- González, J.; Benitez, I.D.; Carcoma, P.; Santisteve, S.; Monge, A.; Moncusi-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratala, A.; Zuil, M.; et al. Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n = 74 | Parameter | n = 74 |
|---|---|---|---|
| Age group | Treatment received during hospital stay | 65 (88%) | |
| 65 years | 40 (54%) | Corticosteroids | 48 (65%) |
| ≥65 years | 34 (46%) | Remdesivir | 25 (34%) |
| Sex | Tocilizumab | 5 (7%) | |
| Male | 54 (73%) | Baricitinib | 2 (3%) |
| Female | 20 (27%) | Medical equipment | |
| BMI | Supplemental Oxygen | 59 (80%) | |
| <25 (kg/m2) | 40 (54%) | High-flow nasal cannula | 2 (3%) |
| ≥25 (kg/m2) | 27 (36%) | Intubation | 14 (19%) |
| Unknown | 7 (10%) | ECMO | 1 (1%) |
| Smoking history Yes | 48 (65%) | Length of hospital stay, days | 19.8 (13.8) |
| No | 26 (35%) | ||
| Comorbidity | 54 (73%) | ||
| Hypertension | 35 (47%) | ||
| Diabetes | 18 (24%) | ||
| Cardiovascular disease | 11 (15%) | ||
| Cerebrovascular disease | 6 (8%) | ||
| Malignant tumor | 3 (4%) | ||
| Autoimmune disease | 3 (4%) | ||
| Respiratory disease | 16 (22%) | ||
| Interstitial lung disease | 3 (4%) | ||
| COPD | 9 (12%) | ||
| Bronchial asthma | 7 (9%) | ||
| 3 Months | 6 Months | |
|---|---|---|
| SF-36 Scale | Mean score (±SD) | Mean score (±SD) |
| PF | 46.6 ± 9.7 | 47.9 ± 8.1 |
| RP | 43.9 ± 13.1 | 46.7 ± 11.7 |
| BP | 49.8 ± 11.9 | 48.8 ± 11.1 |
| GH | 51.2 ± 7.6 | 51.9 ± 8.01 |
| VT | 54.3 ± 10.0 | 53.8 ± 10.1 |
| SF | 42.8 ± 14.3 | 47.6 ± 11.4 |
| RE | 45.0 ± 12.8 | 48.1 ± 11.3 |
| MH | 52.6 ± 9.1 | 53.9 ± 8.71 |
| PCS | 48.4 ± 11.0 | 47.5 ± 9.8 |
| MCS | 56.1 ± 8.5 | 55.5 ± 9.1 |
| RCS | 40.7 ± 13.9 | 45.7 ± 12.3 |
| Role/Social Component Summary Score | ||||||||
|---|---|---|---|---|---|---|---|---|
| 3 Months | 6 Months | |||||||
| Coefficient | 95% C.I. | p-Value | Coefficient | 95% C.I. | p-Value | |||
| PASC at each time points (yes/no) | ||||||||
| any symptoms | −4.76 | −11.3 | 1.78 | 0.151 | −5.52 | −11.91 | 0.87 | 0.090 |
| respiratory symptoms | −6.99 | −13.54 | −0.44 | 0.037 | −5.74 | −12.35 | 0.88 | 0.088 |
| dyspnea | 1.20 | −6.76 | 9.14 | 0.766 | −7.57 | −16.23 | 1.10 | 0.086 |
| cough | −6.86 | −16.3 | 2.58 | 0.152 | −2.94 | −15.71 | 9.82 | 0.647 |
| fatigue | −8.85 | −20.67 | 2.96 | 0.140 | −4.42 | −14.25 | 5.40 | 0.372 |
| numbness | −1.70 | −16.17 | 12.78 | 0.816 | 2.50 | −10.27 | 15.28 | 0.697 |
| joint pain | −13.47 | −33.41 | 6.48 | 0.182 | 2.88 | −22.14 | 27.90 | 0.819 |
| olfactory disorder | 13.82 | −6.11 | 33.75 | 0.171 | - | - | - | - |
| Pulmonary Function Test | ||||||||
| FVC (L) | - | - | - | - | 3.59 | 0.40 | 6.78 | 0.028 |
| %FVC (%) | - | - | - | - | 0.19 | 0.01 | 0.38 | 0.045 |
| FEV1 (L) | - | - | - | - | 3.99 | 0.24 | 7.73 | 0.037 |
| FEV1/FVC (%) | - | - | - | - | −0.07 | −0.31 | 0.17 | 0.554 |
| Role/Social Component Summary Score | ||||||||
|---|---|---|---|---|---|---|---|---|
| 3 Months | 6 Months | |||||||
| Coefficient | 95% C.I. | p-Value | Coefficient | 95% C.I. | p-Value | |||
| Background (yes/no) | ||||||||
| Age ≥ 65 (years old) | −7.74 | −14.00 | −1.45 | 0.016 | −6.91 | −12.50 | −1.32 | 0.016 |
| Sex, male | −4.61 | −11.90 | 2.68 | 0.212 | −0.32 | −6.84 | 6.21 | 0.923 |
| BMI ≥ 25 (kg/m2) | 2.00 | −5.31 | 9.31 | 0.586 | −3.25 | −9.58 | 3.07 | 0.308 |
| Smoking history | 0.85 | −6.01 | 7.71 | 0.806 | −3.69 | −9.70 | 2.33 | 0.226 |
| Any comorbidities | −3.60 | −3.59 | −10.90 | 0.332 | −6.23 | −12.58 | 0.13 | 0.055 |
| Respiratory disease | −7.42 | −15.18 | 0.34 | 0.061 | −1.19 | −8.22 | 5.84 | 0.736 |
| Status during hospitalization (yes/no) | ||||||||
| Treatment | ||||||||
| Corticosteroids | 0.73 | −6.13 | 7.59 | 0.830 | −1.39 | −7.46 | 4.67 | 0.648 |
| Remdesivir | 2.20 | −4.70 | 9.11 | 0.526 | 0.81 | −5.32 | 6.94 | 0.793 |
| Tocilizumab | −5.13 | −18.12 | 7.86 | 0.430 | −5.06 | −16.52 | 6.39 | 0.381 |
| Baricitinib | 11.72 | −8.55 | 31.99 | 0.250 | 1.32 | −16.71 | 19.36 | 0.884 |
| Medical equipment | ||||||||
| Supplemental Oxygen | −7.80 | −15.73 | 0.14 | 0.054 | −5.76 | −12.83 | 1.31 | 0.109 |
| High-flow nasal cannula | −26.57 | −45.78 | −7.37 | 0.007 | −6.74 | −24.50 | 11.01 | 0.452 |
| Intubation | −6.88 | −15.08 | 1.33 | 0.099 | 1.34 | −6.04 | 8.73 | 0.718 |
| ECMO | −2.03 | −30.39 | 26.33 | 0.887 | 2.90 | −22.14 | 27.91 | 0.819 |
| CT score (≥10 points) on admission | −4.08 | −10.87 | 2.70 | 0.233 | −7.76 | −13.88 | −1.65 | 0.014 |
| 3 Months | 6 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% C.I. | p-Value | Coefficient | 95% C.I. | p-Value | |||
| Age ≥ 65 (years old) | −6.39 | −13.69 | 0.91 | 0.085 | −6.08 | −12.89 | 0.72 | 0.078 |
| Sex, male | −1.22 | −9.26 | 6.81 | 0.762 | 1.47 | −6.02 | 8.96 | 0.695 |
| Smoking history | 3.80 | −3.52 | 11.12 | 0.303 | −2.75 | −9.57 | 4.08 | 0.424 |
| Intubation | −10.00 | −19.06 | −0.95 | 0.031 | 2.84 | −5.60 | 11.28 | 0.503 |
| Respiratory disease | −5.91 | −14.39 | 2.58 | 0.169 | 4.65 | −3.26 | 12.55 | 0.244 |
| CT score (≥10 points) | 0.59 | −6.74 | 7.93 | 0.872 | −8.72 | −15.55 | −1.88 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ando, T.; Shimada, S.; Sugihara, J.; Takayama, K.; Kobayashi, M.; Miyashita, Y.; Ito, T.; Okayasu, K.; Tsuyuki, S.; Ohba, T.; et al. Impairment of Social-Related Quality of Life in COVID-19 Pneumonia Survivors: A Prospective Longitudinal Study. J. Clin. Med. 2023, 12, 7640. https://doi.org/10.3390/jcm12247640
Ando T, Shimada S, Sugihara J, Takayama K, Kobayashi M, Miyashita Y, Ito T, Okayasu K, Tsuyuki S, Ohba T, et al. Impairment of Social-Related Quality of Life in COVID-19 Pneumonia Survivors: A Prospective Longitudinal Study. Journal of Clinical Medicine. 2023; 12(24):7640. https://doi.org/10.3390/jcm12247640
Chicago/Turabian StyleAndo, Takahiro, Sho Shimada, Jun Sugihara, Koji Takayama, Masayoshi Kobayashi, Yoshihiro Miyashita, Tatsuya Ito, Kaori Okayasu, Shun Tsuyuki, Takehiko Ohba, and et al. 2023. "Impairment of Social-Related Quality of Life in COVID-19 Pneumonia Survivors: A Prospective Longitudinal Study" Journal of Clinical Medicine 12, no. 24: 7640. https://doi.org/10.3390/jcm12247640