
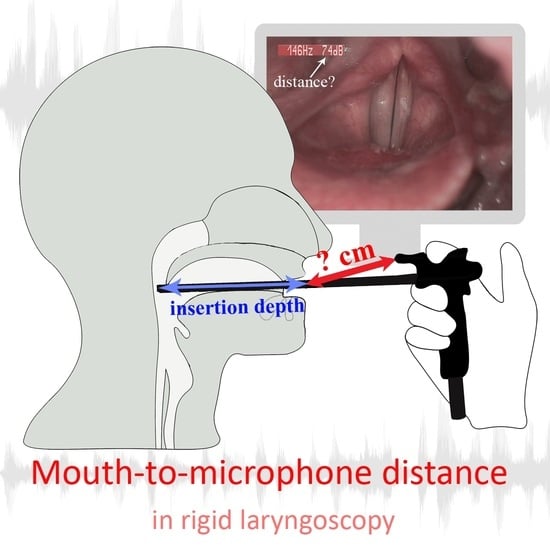
Determining the Mouth-to-Microphone Distance in Rigid Laryngoscopy: A Simple Solution Based on the Newly Measured Values of the Depth of Endoscope Insertion into the Mouth

Abstract
:
1. Introduction
- Is the insertion depth different between male and female patients? We hypothesized the insertion depth to be larger in males, due to their longer vocal tract.
- Is the insertion depth different for the laryngoscopes with a 70° and 90° view? We hypothesized the insertion depth to be larger in the 70° laryngoscope type since its tip is expected to be placed lower in the oropharynx, closer to the larynx.
2. Materials and Methods
2.1. Subjects
2.2. Examination Procedures and Division of the Subjects into Groups
2.3. Examination Equipment
2.4. Calibration Measurements—Laryngoscope Lengths
2.5. Measurements of the Depth of Laryngoscope Insertion into the Mouth
3. Results
3.1. Female–Male Differences
3.2. Differences among the Laryngoscopes
4. Discussion
- The laryngoscope insertion depth was larger in male than female patients;
- The insertion depth was slightly larger for the 70°-view laryngoscope than for the 90°-view laryngoscope.
4.1. Female–Male Differences in Insertion Depth
4.2. Insertion Depth Differences among Different Laryngoscopes
- The 70° scope (L70K) was inserted about 3 mm deeper into the mouth, and its insertion depth varied slightly more among the subjects than in the case of the 90° laryngoscope (L90S);
- The two 90° laryngoscopes (L90S and L90K) could be considered similar in terms of their insertion depth (Table 4).
4.3. Stroboscopy–Videokymography Differences in Insertion Depth
4.4. Rules for Estimating the MTM Distance in Rigid Laryngoscopy
4.5. Uncertainty of the MTM Distance
4.6. MTM Distances for L70K, L90K, and L90S Laryngoscopes
4.7. Representativeness of the Sample Size in Relation to the Broader Population and Study Limitations
5. Practical Recommendations and Conclusions
- Use the table value of the laryngoscope insertion depth, DI (i.e., 9.7/9.4 cm for men, 8.9/8.7 cm for women, or 9.3/9.0 cm for all adults for 70°/90° endoscopes, respectively);
- Calculate the typical MTM distance for that endoscope by using the Equation (2). These steps were used for specifying the MTM distances of the three microphones reported in Table 5 that can be considered typical case examples.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. MTM Distances for Females and Males


References
- Angerstein, W.; Baracca, G.; Dejonckere, P.; Echternach, M.; Eysholdt, U.; Fussi, F.; Geneid, A.; Hacki, T.; Karmelita-Katulska, K.; Haubrich, R.; et al. Diagnosis and Differential Diagnosis of Voice Disorders. In Phoniatrics I: Fundamentals–Voice Disorders–Disorders of Language and Hearing Development; Zehnhoff-Dinnesen, A.A., Wiskirska-Woznica, B., Neumann, K., Nawka, T., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 349–430. [Google Scholar]
- Woo, P. Objective Measures of Laryngeal Imaging: What Have We Learned Since Dr. Paul Moore. J. Voice 2014, 28, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Bless, D.M.; Patel, R.R.; Connor, N. Laryngeal Imaging: Stroboscopy, High-Speed Digital Imaging, and Kymography. In The Larynx; Fried, M.P., Ferlito, A., Eds.; Plural Publishing: San Diego, CA, USA, 2009; pp. 181–210. [Google Scholar]
- Švec, J.G.; Schutte, H.K. Kymographic Imaging of Laryngeal Vibrations. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Woo, P. Objective Measures of Stroboscopy and High-Speed Video. Adv. Oto-Rhino-Laryngol. 2020, 85, 25–44. [Google Scholar] [CrossRef]
- Kumar, S.P.; Švec, J.G. A Simple Method to Obtain Basic Acoustic Measures from Video Recordings as Subtitles. J. Speech Lang. Hear. Res. 2018, 61, 2196–2204. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.R.; Awan, S.N.; Barkmeier-Kraemer, J.; Courey, M.; Deliyski, D.; Eadie, T.; Paul, D.; Švec, J.G.; Hillman, R. Recommended Protocols for Instrumental Assessment of Voice: American Speech-Language-Hearing Association Expert Panel to Develop a Protocol for Instrumental Assessment of Vocal Function. Am. J. Speech Lang. Pathol. 2018, 27, 887–905. [Google Scholar] [CrossRef] [PubMed]
- Švec, J.G.; Granqvist, S. Tutorial and Guidelines on Measurement of Sound Pressure Level in Voice and Speech. J. Speech Lang. Hear. Res. 2018, 61, 441–461. [Google Scholar] [CrossRef] [PubMed]
- Wendler, J. Stroboscopy. J. Voice 1992, 6, 149–154. [Google Scholar] [CrossRef]
- Shao, J.; Stern, J.; Wang, Z.-M.; Hanson, D.; Jiang, J. Clinical Evaluation of 70° and 90° Laryngeal Telescopes. Arch. Otolaryngol. Neck Surg. 2002, 128, 941. [Google Scholar] [CrossRef] [PubMed]
- Junaid, M.; Roohullah, M.; Uddin, I.; Hussain, A.; Khan, M.A. Comparative Evaluation of 70° And 90° Rigid Endoscope In Successful Visualization of The Hidden Areas of Larynx. J. Med. Sci. 2021, 29, 243–246. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Prodecure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Valášková, D. Variability of Distance of a Laryngoscope-Attached Microphone from the Mouth in Laryngoscopic Examinations. Bachelor’s Thesis, Palacký University, Olomouc, Czechia, 2018. [Google Scholar]
- Valášková, D. Depth of Laryngoscope Insertion in the Mouth during Laryngoscopic Examinations: Implications for Measurements of Sound Pressure Level by a Microphone Attached to the Laryngoscope. Master’s Thesis, Palacký University, Olomouc, Czechia, 2020. [Google Scholar]
- Fitch, W.T.; Giedd, J. Morphology and Development of the Human Vocal Tract: A Study Using Magnetic Resonance Imaging. J. Acoust. Soc. Am. 1999, 106, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- Barbier, G.; Boë, L.-J.; Captier, G.; Laboissière, R. Human Vocal Tract Growth: A Longitudinal Study of the Development of Various Anatomical Structures. In Proceedings of the Interspeech 2015-16th Annual Conference of the International Speech Communication Association, Dresden, Germany, 10 September 2015; pp. 364–368. [Google Scholar]
- Vorperian, H.K.; Wang, S.; Michael Schimek, E.; Durtschi, R.B.; Kent, R.D.; Gentry, L.R.; Chung, M.K. Developmental Sexual Dimorphism of the Oral and Pharyngeal Portions of the Vocal Tract: An Imaging Study. J. Speech Lang. Hear. Res. 2011, 54, 995–1010. [Google Scholar] [CrossRef] [PubMed]
- Vorperian, H.K.; Wang, S.; Chung, M.K.; Schimek, E.M.; Durtschi, R.B.; Kent, R.D.; Ziegert, A.J.; Gentry, L.R. Anatomic Development of the Oral and Pharyngeal Portions of the Vocal Tract: An Imaging Study. J. Acoust. Soc. Am. 2009, 125, 1666–1678. [Google Scholar] [CrossRef] [PubMed]
- Vorperian, H.K.; Schimek, E.M.; Wang, S.; Chung, M.K.; Kent, R.D.; Ziegert, A.J.; Gentry, L.R. Anatomic Development of the Vocal Tract during the First Two Decades of Life: Evidence on Prepubertal Sexual Dimorphism from MRI and CT Studies. J. Acoust. Soc. Am. 2007, 122, 3031. [Google Scholar] [CrossRef]
- Goldstein, U.G. An Articulatory Model for the Vocal Tracts of Growing Children. Doctoral Dissertation, Massachusetts Institue of Technology, Cambridge, MA, USA, 1980. [Google Scholar]
- ISO/IEC Guide 98:1993; Guide to the Expression of Uncertainty in Measurement (GUM). International Organization for Standardization: Geneva, Switzerland, 1993.
- Xue, S.A.; Hao, G.J.P.; Mayo, R. Volumetric Measurements of Vocal Tracts for Male Speakers from Different Races. Clin. Linguist. Phon. 2006, 20, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Xue, S.A.; Hao, J.G. Normative Standards for Vocal Tract Dimensions by Race as Measured by Acoustic Pharyngometry. J. Voice 2006, 20, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Primov-Fever, A.; Amir, O.; Jedwab, D. The Feasibility of Rigid Stroboscopy in Children. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 1077–1079. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Number of Males (M), Females (F) | Type of Used Laryngoscope | Age (Mean ± SD) |
|---|---|---|---|
| 1 | 20 M 20 F | L70K + L90S | M 53 ± 17 |
| F 42 ± 20 | |||
| 2 | 20 M 20 F | L90K + L90S | M 47 ± 17 |
| F 50 ± 18 | |||
| 3 | 20 M 20 F | L90S | M 50 ± 17 |
| F 44 ± 15 |
| Laryngoscope Code | Type of Examination | Angle (°) | Length of Tube, l (cm) | Reference Length, r (cm) | Microphone Distance, a (cm) | Microphone Distance, b (cm) | Lens to Tip Distance, c (cm) |
|---|---|---|---|---|---|---|---|
| L70K | VKG | 70 | 18.64 ± 0.08 | 4.44 ± 0.02 | 30.52 ± 0.05 | 2.67 ± 0.06 | 0.46 ± 0.01 |
| L90K | VKG | 90 | 19.09 ± 0.06 | 4.31 ± 0.08 | 30.26 ± 0.04 | 2.67 ± 0.06 | 0.61 ± 0.01 |
| L90S | Stroboscopy | 90 | 17.27 ± 0.06 | 7.26 ± 0.05 | 17.27 ± 0.06 | 1.08 ± 0.03 | 0.30 ± 0.01 |
| Sex | L70K | L90K | L90S | L90K + L90S | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | Insertion Depth, DI (cm) | n | Insertion Depth, DI (cm) | n | Insertion Depth, DI (cm) | n | Insertion Depth, DI (cm) | ||
| Insertion Depth | Females (F) | 20 | 8.91 ± 0.86 | 20 | 8.84 ± 0.68 | 60 | 8.63 ± 0.63 | 80 | 8.68 ± 0.65 |
| Males (M) | 20 | 9.70 ± 0.90 | 20 | 9.47 ± 0.63 | 60 | 9.39 ± 0.65 | 80 | 9.41 ± 0.64 | |
| Adults (F + M) | 40 | 9.31 ± 0.90 | 40 | 9.15 ± 0.72 | 120 | 9.01 ± 0.74 | 160 | 9.05 ± 0.74 | |
| F-test (p-value) | Females vs. Males | 20/20 | 0.44 | 20/20 | 0.38 | 60/60 | 0.42 | 80/80 | 0.47 |
| t-test (p-value) | Females vs. Males | 20/20 | 0.009 ** | 20/20 | 0.005 ** | 60/60 | <0.001 *** | 80/80 | <0.001 *** |
| Sex | Insertion Depth Differences (cm) | Pair t-Test (p-Value) | F-Test (p-Value) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | L70K–L90S | L90K–L90S | N | L70K vs. L90S | L90K vs. L90S | N | L70K vs. L90S | L90K vs. L90S | |
| Females (F) | 20/20 | 0.28 ± 0.56 | 0.04 ± 0.38 | 20/20 | 0.04 * | 0.55 | 20/20 | 0.04 * | 0.32 |
| Males (M) | 20/20 | 0.25 ± 0.76 | 0.05 ± 0.38 | 20/20 | 0.16 | 0.72 | 20/20 | 0.07 | 0.39 |
| Adults (F + M) | 40/40 | 0.27 ± 0.67 | 0.04 ± 0.38 | 40/40 | 0.17 | 0.80 | 40/40 | 0.04 * | 0.47 |
| Type of Laryngoscope | d Adults (cm) | d Females (cm) | d Males (cm) |
|---|---|---|---|
| L70K | 21.38 ± 0.89 | 21.77 ± 0.86 | 20.99 ± 0.89 |
| L90K | 21.28 ± 0.72 | 21.59 ± 0.68 | 20.96 ± 0.63 |
| L90S | 8.33 ± 0.74 | 8.71 ± 0.63 | 7.95 ± 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valášková, D.; Vydrová, J.; Švec, J.G. Determining the Mouth-to-Microphone Distance in Rigid Laryngoscopy: A Simple Solution Based on the Newly Measured Values of the Depth of Endoscope Insertion into the Mouth. J. Clin. Med. 2023, 12, 7560. https://doi.org/10.3390/jcm12247560
Valášková D, Vydrová J, Švec JG. Determining the Mouth-to-Microphone Distance in Rigid Laryngoscopy: A Simple Solution Based on the Newly Measured Values of the Depth of Endoscope Insertion into the Mouth. Journal of Clinical Medicine. 2023; 12(24):7560. https://doi.org/10.3390/jcm12247560
Chicago/Turabian StyleValášková, Dominika, Jitka Vydrová, and Jan G. Švec. 2023. "Determining the Mouth-to-Microphone Distance in Rigid Laryngoscopy: A Simple Solution Based on the Newly Measured Values of the Depth of Endoscope Insertion into the Mouth" Journal of Clinical Medicine 12, no. 24: 7560. https://doi.org/10.3390/jcm12247560