
Comparison of Intravenous Acetaminophen and Intravenous Patient-Controlled Analgesia Fentanyl after Total Hip Arthroplasty: A Multicenter Randomized Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Protocol
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fischer, H.B.J.; Simanski, C.J.P. A procedure-specific systematic review and consensus recommendations for analgesia after total hip replacement. Anaesthesia 2005, 60, 1189–1202. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Miller, A.G.; Gandhi, K. Multimodal pain management after total joint arthroplasty. J. Bone Joint Surg. Am. 2011, 93, 1075–1084. [Google Scholar] [CrossRef]
- Roberts, G.W.; Bekker, T.B.; Carlsen, H.H.; Moffatt, C.H.; Slattery, P.J.; McClure, A.F. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth. Analg. 2005, 101, 1343–1348. [Google Scholar] [CrossRef]
- Woodhouse, A.; Mather, L.E. Nausea and vomiting in the postoperative patient-controlled analgesia environment. Anaesthesia 1997, 52, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Tramèr, M.R.; Walder, B. Efficacy and adverse effects of prophylactic antiemetics during patient-controlled analgesia therapy: A quantitative systematic review. Anesth. Analg. 1999, 88, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Sinatra, R.S.; Jahr, J.S.; Reynolds, L.W.; Viscusi, E.R.; Groudine, S.B.; Payen-Champenois, C. Efficacy and safety of single and repeated administration of 1 gram intravenous acetaminophen injection (paracetamol) for pain management after major orthopedic surgery. Anesthesiology 2005, 102, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, C.I.; Pérez, M.J.; Manautou, J.E.; Mottino, A.D. Acetaminophen from liver to brain: New insights into drug pharmacological action and toxicity. Pharmacol. Res. 2016, 109, 119–131. [Google Scholar] [CrossRef]
- Takeda, Y.; Fukunishi, S.; Nishio, S.; Yoshiya, S.; Hashimoto, K.; Simura, Y. Evaluating the effect of intravenous acetaminophen in multimodal analgesia after total hip arthroplasty: A randomized controlled trial. J. Arthroplasty 2019, 34, 1155–1161. [Google Scholar] [CrossRef]
- Maiese, B.A.; Pham, A.T.; Shah, M.V.; Eaddy, M.T.; Lunacsek, O.E.; Wan, G.J. Hospitalization costs for patients undergoing orthopedic surgery treated with intravenous acetaminophen (IV-APAP) plus other IV analgesics or IV opioid monotherapy for postoperative pain. Adv. Ther. 2017, 34, 421–435. [Google Scholar] [CrossRef]
- Shaffer, E.E.; Pham, A.; Woldman, R.L.; Spiegelman, A.; Strassels, S.A.; Wan, G.J.; Zimmerman, T. Estimating the effect of intravenous acetaminophen for postoperative pain management on length of stay and inpatient hospital costs. Adv. Ther. 2017, 33, 2211–2228. [Google Scholar] [CrossRef]
- Berend, K.R.; Lombardi, A.V., Jr.; Seng, B.E.; Adams, J.B. Enhanced early outcomes with the anterior supine intermuscular approach in primary total hip arthroplasty. J. Bone Joint Surg. Am. 2009, 91 (Suppl. 6), 107–120. [Google Scholar] [CrossRef] [PubMed]
- Meneghini, R.M.; Pagnano, M.W.; Trousdale, R.T.; Hozack, W.J. Muscle damage during MIS total hip arthroplasty: Smith-Petersen versus posterior approach. Clin. Orthop. Relat. Res. 2006, 453, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Takada, R.; Jinno, T.; Miyatake, K.; Hirao, M.; Kimura, A.; Koga, D.; Yagishita, K.; Okawa, A. Direct anterior versus anterolateral approach in one-stage supine total hip arthroplasty. Focused on nerve injury: A prospective, randomized, controlled trial. J. Orthop. Sci. 2018, 23, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Hou, J.Z.; Wu, C.H.; Zhou, Y.J.; Gu, X.M.; Wang, H.H.; Feng, W.; Cheng, Y.X.; Sheng, X.; Bao, H.W. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J. Orthop. Surg. Res. 2018, 13, 229. [Google Scholar] [CrossRef] [PubMed]
- Imai, N.; Dohmae, Y.; Suda, K.; Miyasaka, D.; Ito, T.; Endo, N. Tranexamic acid for reduction of blood loss during total hip arthroplasty. J. Arthroplasty 2012, 27, 1838–1843. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.B. Estimating allowable blood loss: Corrected for dilution. Anesthesiology 1983, 58, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; McFarland, C.A. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain 1993, 55, 195–203. [Google Scholar] [CrossRef]
- Rodriguez, C.S. Pain measurement in the elderly: A review. J. Pain Manag. 2001, 2, 38–46. [Google Scholar] [CrossRef]
- Ong, C.K.; Seymour, R.A.; Lirk, P.; Merry, A.F. Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory drugs: A qualitative systematic review of analgesic efficacy for acute postoperative pain. Anesth. Analg. 2010, 110, 1170–1179. [Google Scholar] [CrossRef]
- Gazendam, A.; Ekhtiari, S.; Horner, N.S.; Simunovic, N.; Khan, M.; Sa, D.L.; Madden, K.; Ayeni, O.R. Effect of a postoperative multimodal opioid-sparing protocol vs standard opioid prescribing on postoperative opioid consumption after knee or shoulder arthroscopy: A randomized clinical trial. JAMA 2022, 328, 1326–1335. [Google Scholar]
- Parvataneni, H.K.; Shah, V.P.; Howard, H.; Cole, N.; Ranawat, A.S.; Ranawat, C.S. Controlling pain after total hip and knee arthroplasty using a multimodal protocol with local periarticular injections: A prospective randomized study. J. Arthroplasty 2007, 22 (Suppl. 2), 33–38. [Google Scholar] [CrossRef] [PubMed]
- De Boer, H.D.; Detriche, O.; Forget, P. Opioid-related side effects: Postoperative ileus, urinary retention, nausea and vomiting, and shivering. A review of the literature. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, Q.; Lin, J.; Qian, W.; Jin, J.; Gao, P.; Zhang, B.; Feng, B.; Weng, X. Risk factors of postoperative nausea and vomiting after total hip arthroplasty or total knee arthroplasty: A retrospective study. Ann. Transl. Med. 2020, 8, 1088. [Google Scholar] [CrossRef] [PubMed]
- Ukai, T.; Ebihara, G.; Watanabe, M. Comparison of short-term outcomes of anterolateral supine approach and posterolateral approach for primary total hip arthroplasty: A retrospective study. J. Orthop. Traumatol. 2021, 22, 6. [Google Scholar] [CrossRef]


{kind=link}
| APAP (n = 90) | IV-PCA (n = 88) | p-Value | |
|---|---|---|---|
| Age (years) | 66.5 ± 8.2 | 67.9 ± 9.3 | * 0.281 |
| Sex (male/female) | 18/72 | 20/66 | † 0.600 |
| Body mass index (kg/m2) | 24.2 ± 4.2 | 23.9 ± 3.5 | * 0.654 |
| Operation time (min) | 92.5 ± 20.1 | 89.8 ± 21.0 | * 0.414 |
| Intraoperative bleed (mL) | 338.9 ± 147.5 | 346.7 ± 182.5 | * 0.763 |
| Estimated blood loss (mL) | 899.9 ± 340.6 | 909.4 ± 370.1 | * 0.864 |
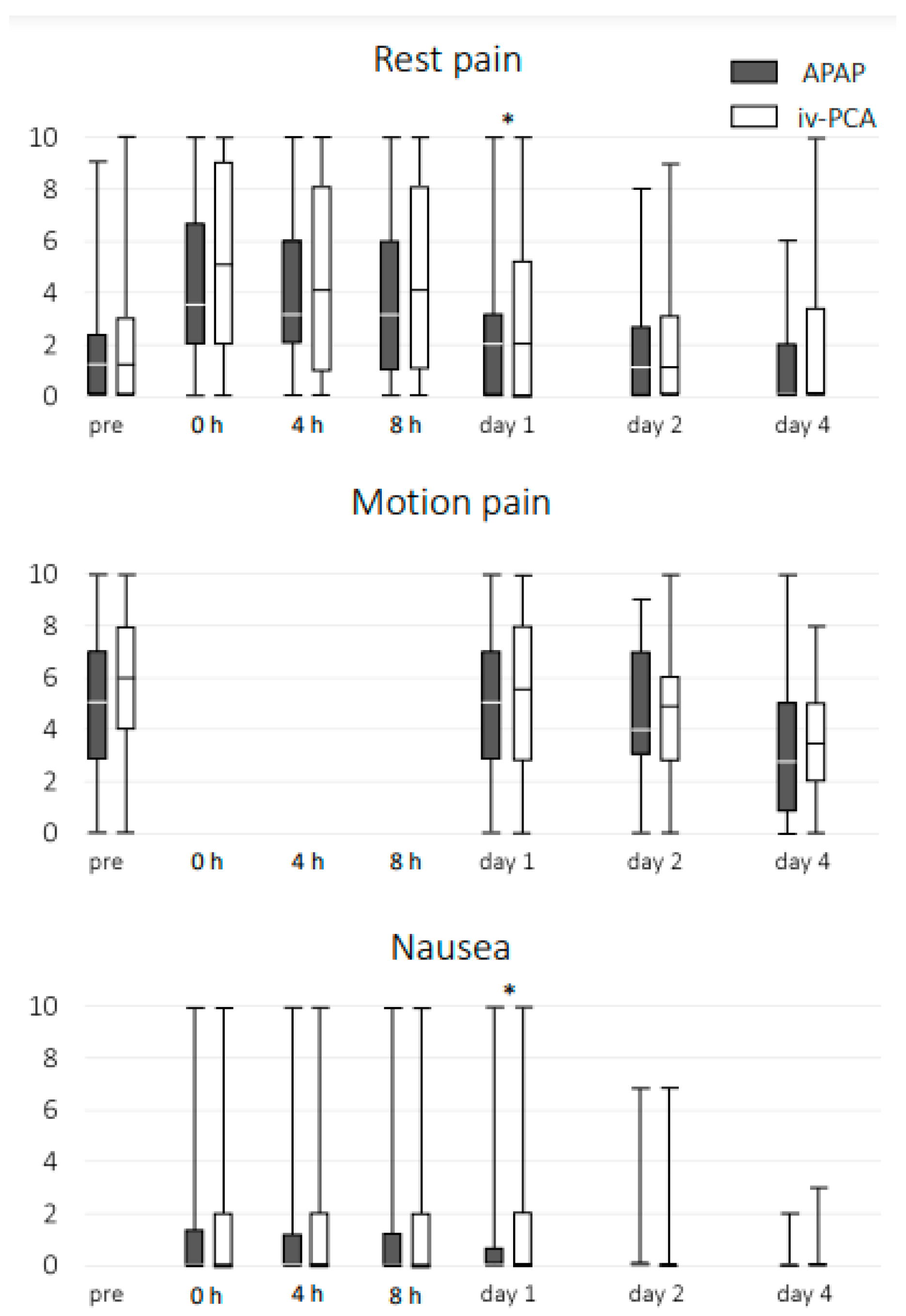
| Pre | 0 h | 4 h | 8 h | Day 1 | Day 2 | Day 4 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RP | MP | RP | N | RP | N | RP | N | RP | MP | N | RP | MP | N | RP | MP | N | |
| APAP | 13 | 22 | 45 | 15 | 41 | 11 | 37 | 11 | 20 | 26 | 9 | 17 | 55 | 2 | 9 | 34 | 0 |
| IV-PCA | 14 | 21 | 52 | 14 | 46 | 16 | 45 | 19 | 32 | 29 | 19 | 26 | 52 | 5 | 17 | 43 | 0 |
| p-value | 0.537 | 0.928 | 0.223 | 0.891 | 0.370 | 0.163 | 0.179 | 0.095 | 0.009 * | 0.557 | 0.034 * | 0.097 | 0.736 | 0.247 | 0.030 * | 0.175 | / |
| 0 h | 4 h | 8 h | Day 1 | Day 2 | Day 4 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RP | N | RP | N | RP | N | RP | MP | N | RP | MP | N | RP | MP | N | |
| Age | −0.038 | 0.024 | −0.198 * | −0.024 | −0.071 | −0.009 | −0.080 | −0.036 | 0.078 | −0.122 | −0.110 | −0.168 | −0.105 | −0.049 | −0.084 |
| Body mass index | 0.029 | 0.101 | 0.027 | 0.027 | −0.021 | 0.038 | −0.064 | 0.022 | 0.058 | −0.031 | −0.004 | −0.033 | −0.038 | −0.026 | 0.155 |
| Pre RP | 0.292 * | 0.201 * | 0.306 * | 0.048 | 0.352 * | 0.094 | 0.457 * | 0.237 * | −0.085 | 0.517 * | 0.218 * | −0.035 | 0.472 * | 0.211 * | 0.001 |
| Pre MP | 0.192 * | −0.093 | 0.150 | −0.071 | 0.167 | −0.090 | 0.073 | 0.096 | −0.090 | 0.106 | 0.095 | −0.105 | 0.134 | 0.021 | −0.091 |
| Rest Pain | 0 h | 4 h | 8 h | Day 1 | Day 2 | Day 4 |
|---|---|---|---|---|---|---|
| Nausea at 4 h | 0.072 | 0.118 | 0.131 | 0.199 * | 0.160 | 0.036 |
| at 8 h | 0.096 | 0.193 * | 0.194 * | 0.245 * | 0.188 * | 0.073 |
| APAP (n = 90) | IV-PCA (n = 88) | p-Value | |
|---|---|---|---|
| DVT | 3 (3.3%) | 4 (4.5%) | 0.677 |
| Elevated liver enzymes | 1 (1.1%) | 1 (1.1%) | 0.987 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, Y.; Imai, N.; Miyasaka, D.; Suzuki, H.; Horigome, Y.; Takahashi, Y.; Kawashima, H. Comparison of Intravenous Acetaminophen and Intravenous Patient-Controlled Analgesia Fentanyl after Total Hip Arthroplasty: A Multicenter Randomized Controlled Trial. J. Clin. Med. 2023, 12, 7445. https://doi.org/10.3390/jcm12237445
Sakai Y, Imai N, Miyasaka D, Suzuki H, Horigome Y, Takahashi Y, Kawashima H. Comparison of Intravenous Acetaminophen and Intravenous Patient-Controlled Analgesia Fentanyl after Total Hip Arthroplasty: A Multicenter Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(23):7445. https://doi.org/10.3390/jcm12237445
Chicago/Turabian StyleSakai, Yoshinori, Norio Imai, Dai Miyasaka, Hayato Suzuki, Yoji Horigome, Yasuhito Takahashi, and Hiroyuki Kawashima. 2023. "Comparison of Intravenous Acetaminophen and Intravenous Patient-Controlled Analgesia Fentanyl after Total Hip Arthroplasty: A Multicenter Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 23: 7445. https://doi.org/10.3390/jcm12237445