
Evolution of More Aggressive LDL-Cholesterol Targets and Therapies for Cardiovascular Disease Prevention

Abstract
:
1. Background
2. LDL-C as a Predictor of CVD
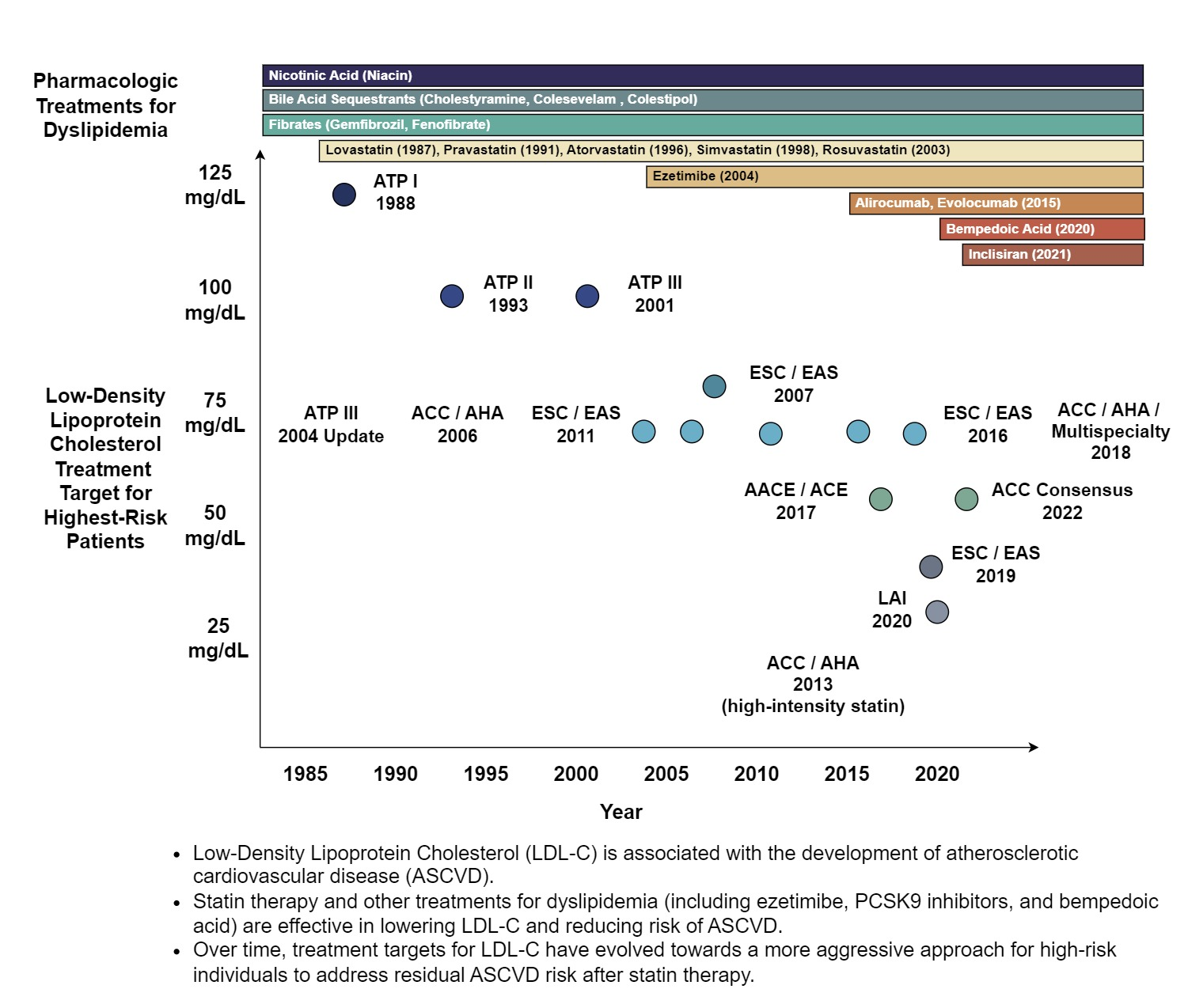
3. LDL-Cholesterol-Lowering Pharmacotherapy and Cardiovascular Outcomes Benefit
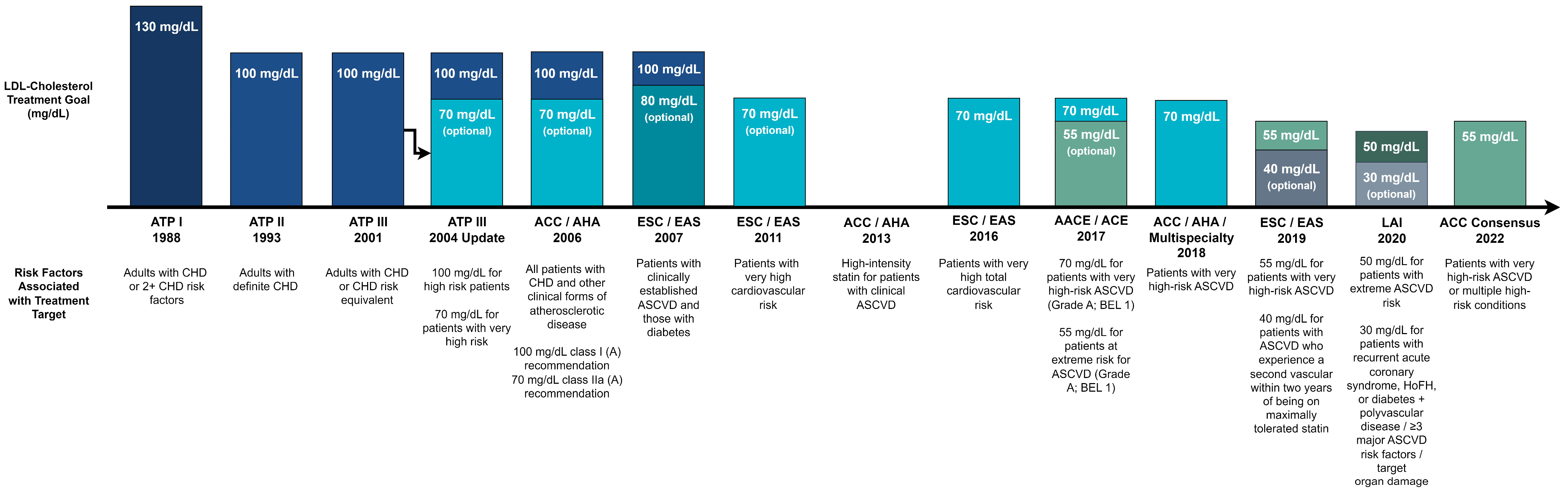
4. Early Years of Cholesterol Treatment Guidelines
5. Lower and More Aggressive LDL-Cholesterol Targets
6. Benefits and Risks of Very Low LDL-Cholesterol
7. Non-HDL Cholesterol and Apolipoprotein B as Secondary Treatment Targets
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable Risk Factors, Cardiovascular Disease, and Mortality in 155,722 Individuals from 21 High-Income, Middle-Income, and Low-Income Countries (PURE): A Prospective Cohort Study. Lancet Lond. Engl. 2020, 395, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Kathiresan, S.; Srivastava, D. Genetics of Human Cardiovascular Disease. Cell 2012, 148, 1242–1257. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, Z.; Joseph, P.; Hu, B.; Yin, L.; Tse, L.A.; Rangarajan, S.; Wang, C.; Wang, Y.; Islam, S.; et al. Modifiable Risk Factors Associated with Cardiovascular Disease and Mortality in China: A PURE Substudy. Eur. Heart J. 2022, 43, 2852–2863. [Google Scholar] [CrossRef] [PubMed]
- Global Cardiovascular Risk Consortium; Magnussen, C.; Ojeda, F.M.; Leong, D.P.; Alegre-Diaz, J.; Amouyel, P.; Aviles-Santa, L.; De Bacquer, D.; Ballantyne, C.M.; Bernabé-Ortiz, A.; et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N. Engl. J. Med. 2023, 389, 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group Prevention of Cardiovascular Events and Death with Pravastatin in Patients with Coronary Heart Disease and a Broad Range of Initial Cholesterol Levels. N. Engl. J. Med. 1998, 339, 1349–1357. [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The Effects of Lowering LDL Cholesterol with Statin Therapy in People at Low Risk of Vascular Disease: Meta-Analysis of Individual Data from 27 Randomised Trials. Lancet Lond. Engl. 2012, 380, 581–590. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Kearney, P.M.; Blackwell, L.; Collins, R.; Keech, A.; Simes, J.; Peto, R.; Armitage, J.; Baigent, C. Efficacy of Cholesterol-Lowering Therapy in 18,686 People with Diabetes in 14 Randomised Trials of Statins: A Meta-Analysis. Lancet Lond. Engl. 2008, 371, 117–125. [Google Scholar] [CrossRef]
- Fox, C.S.; Pencina, M.J.; Wilson, P.W.F.; Paynter, N.P.; Vasan, R.S.; D’Agostino, R.B. Lifetime Risk of Cardiovascular Disease among Individuals with and without Diabetes Stratified by Obesity Status in the Framingham Heart Study. Diabetes Care 2008, 31, 1582–1584. [Google Scholar] [CrossRef]
- Kuijpers, P.M.J.C. History in Medicine: The Story of Cholesterol, Lipids and Cardiology. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-19/history-in-medicine-the-story-of-cholesterol-lipids-and-cardiology (accessed on 4 September 2023).
- Endo, A. A Historical Perspective on the Discovery of Statins. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2010, 86, 484–493. [Google Scholar] [CrossRef]
- Gofman, J.W. Diet and Lipotrophic Agents in Atherosclerosis. Bull. N. Y. Acad. Med. 1952, 28, 279–293. [Google Scholar] [PubMed]
- Gordon, T.; Castelli, W.P.; Hjortland, M.C.; Kannel, W.B.; Dawber, T.R. High Density Lipoprotein as a Protective Factor against Coronary Heart Disease. The Framingham Study. Am. J. Med. 1977, 62, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Kwiterovich, P.O. The Metabolic Pathways of High-Density Lipoprotein, Low-Density Lipoprotein, and Triglycerides: A Current Review. Am. J. Cardiol. 2000, 86, 5L–10L. [Google Scholar] [CrossRef] [PubMed]
- Low-Density Lipoproteins Cause Atherosclerotic Cardiovascular Disease: Pathophysiological, Genetic, and Therapeutic Insights: A Consensus Statement from the European Atherosclerosis Society Consensus Panel|European Heart Journal|Oxford Academic. Available online: https://academic.oup.com/eurheartj/article/41/24/2313/5735221 (accessed on 4 September 2023).
- Moore, K.; Sheedy, F.; Fisher, E. Macrophages in Atherosclerosis: A Dynamic Balance. Nat. Rev. Immunol. 2013, 13, 709–721. [Google Scholar] [CrossRef]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of Plaque Formation and Rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef] [PubMed]
- Glomset, J.A.; Janssen, E.T.; Kennedy, R.; Dobbins, J. Role of Plasma Lecithin:Cholesterol Acyltransferase in the Metabolism of High Density Lipoproteins. J. Lipid Res. 1966, 7, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.; Abbott, R.D.; Castelli, W.P. High Density Lipoprotein Cholesterol and Mortality. The Framingham Heart Study. Arteriosclerosis 1988, 8, 737–741. [Google Scholar] [CrossRef]
- Gordon, D.J.; Probstfield, J.L.; Garrison, R.J.; Neaton, J.D.; Castelli, W.P.; Knoke, J.D.; Jacobs, D.R.; Bangdiwala, S.; Tyroler, H.A. High-Density Lipoprotein Cholesterol and Cardiovascular Disease. Four Prospective American Studies. Circulation 1989, 79, 8–15. [Google Scholar] [CrossRef]
- Liu, C.; Dhindsa, D.; Almuwaqqat, Z.; Ko, Y.-A.; Mehta, A.; Alkhoder, A.A.; Alras, Z.; Desai, S.R.; Patel, K.J.; Hooda, A.; et al. Association Between High-Density Lipoprotein Cholesterol Levels and Adverse Cardiovascular Outcomes in High-Risk Populations. JAMA Cardiol. 2022, 7, 672–680. [Google Scholar] [CrossRef]
- Soutar, A.K.; Naoumova, R.P. Mechanisms of Disease: Genetic Causes of Familial Hypercholesterolemia. Nat. Clin. Pract. Cardiovasc. Med. 2007, 4, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Cuchel, M.; Bruckert, E.; Ginsberg, H.N.; Raal, F.J.; Santos, R.D.; Hegele, R.A.; Kuivenhoven, J.A.; Nordestgaard, B.G.; Descamps, O.S.; Steinhagen-Thiessen, E.; et al. Homozygous Familial Hypercholesterolaemia: New Insights and Guidance for Clinicians to Improve Detection and Clinical Management. A Position Paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur. Heart J. 2014, 35, 2146–2157. [Google Scholar] [CrossRef] [PubMed]
- Alonso, R.; Mata, P.; Zambón, D.; Mata, N.; Fuentes-Jiménez, F. Early Diagnosis and Treatment of Familial Hypercholesterolemia: Improving Patient Outcomes. Expert Rev. Cardiovasc. Ther. 2013, 11, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Nordestgaard, B.G.; Chapman, M.J.; Humphries, S.E.; Ginsberg, H.N.; Masana, L.; Descamps, O.S.; Wiklund, O.; Hegele, R.A.; Raal, F.J.; Defesche, J.C.; et al. Familial Hypercholesterolaemia Is Underdiagnosed and Undertreated in the General Population: Guidance for Clinicians to Prevent Coronary Heart Disease: Consensus Statement of the European Atherosclerosis Society. Eur. Heart J. 2013, 34, 3478–3490. [Google Scholar] [CrossRef] [PubMed]
- Onorato, A.; Sturm, A.C. Heterozygous Familial Hypercholesterolemia. Circulation 2016, 133, e587–e589. [Google Scholar] [CrossRef] [PubMed]
- Sjouke, B.; Kusters, D.M.; Kindt, I.; Besseling, J.; Defesche, J.C.; Sijbrands, E.J.G.; Roeters van Lennep, J.E.; Stalenhoef, A.F.H.; Wiegman, A.; de Graaf, J.; et al. Homozygous Autosomal Dominant Hypercholesterolaemia in the Netherlands: Prevalence, Genotype–Phenotype Relationship, and Clinical Outcome. Eur. Heart J. 2015, 36, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Akioyamen, L.E.; Genest, J.; Shan, S.D.; Reel, R.L.; Albaum, J.M.; Chu, A.; Tu, J.V. Estimating the Prevalence of Heterozygous Familial Hypercholesterolaemia: A Systematic Review and Meta-Analysis. BMJ Open 2017, 7, e016461. [Google Scholar] [CrossRef]
- Raal, F.J.; Hovingh, G.K.; Blom, D.; Santos, R.D.; Harada-Shiba, M.; Bruckert, E.; Couture, P.; Soran, H.; Watts, G.F.; Kurtz, C.; et al. Long-Term Treatment with Evolocumab Added to Conventional Drug Therapy, with or without Apheresis, in Patients with Homozygous Familial Hypercholesterolaemia: An Interim Subset Analysis of the Open-Label TAUSSIG Study. Lancet Diabetes Endocrinol. 2017, 5, 280–290. [Google Scholar] [CrossRef]
- Wang, A.; Richhariya, A.; Gandra, S.R.; Calimlim, B.; Kim, L.; Quek, R.G.W.; Nordyke, R.J.; Toth, P.P. Systematic Review of Low-Density Lipoprotein Cholesterol Apheresis for the Treatment of Familial Hypercholesterolemia. J. Am. Heart Assoc. 2016, 5, e003294. [Google Scholar] [CrossRef]
- Moriarty, P.M.; Parhofer, K.G.; Babirak, S.P.; Cornier, M.-A.; Duell, P.B.; Hohenstein, B.; Leebmann, J.; Ramlow, W.; Schettler, V.; Simha, V.; et al. Alirocumab in Patients with Heterozygous Familial Hypercholesterolaemia Undergoing Lipoprotein Apheresis: The ODYSSEY ESCAPE Trial. Eur. Heart J. 2016, 37, 3588–3595. [Google Scholar] [CrossRef]
- Gao, Y.; Shah, L.M.; Ding, J.; Martin, S.S. US Trends in Cholesterol Screening, Lipid Levels, and Lipid-Lowering Medication Use in US Adults, 1999 to 2018. J. Am. Heart Assoc. 2023, 12, e028205. [Google Scholar] [CrossRef] [PubMed]
- Prior, I.A.; Davidson, F.; Salmond, C.E.; Czochanska, Z. Cholesterol, Coconuts, and Diet on Polynesian Atolls: A Natural Experiment: The Pukapuka and Tokelau Island Studies. Am. J. Clin. Nutr. 1981, 34, 1552–1561. [Google Scholar] [CrossRef] [PubMed]
- Raichlen, D.A.; Pontzer, H.; Harris, J.A.; Mabulla, A.Z.P.; Marlowe, F.W.; Josh Snodgrass, J.; Eick, G.; Colette Berbesque, J.; Sancilio, A.; Wood, B.M. Physical Activity Patterns and Biomarkers of Cardiovascular Disease Risk in Hunter-Gatherers. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2017, 29, e22919. [Google Scholar] [CrossRef] [PubMed]
- Barnicot, N.A.; Bennett, F.J.; Woodburn, J.C.; Pilkington, T.R.; Antonis, A. Blood Pressure and Serum Cholesterol in the Hadza of Tanzania. Hum. Biol. 1972, 44, 87–116. [Google Scholar] [PubMed]
- Kaplan, H.; Thompson, R.C.; Trumble, B.C.; Wann, L.S.; Allam, A.H.; Beheim, B.; Frohlich, B.; Sutherland, M.L.; Sutherland, J.D.; Stieglitz, J.; et al. Coronary Atherosclerosis in Indigenous South American Tsimane: A Cross-Sectional Cohort Study. Lancet 2017, 389, 1730–1739. [Google Scholar] [CrossRef] [PubMed]
- Vasunilashorn, S.; Crimmins, E.M.; Kim, J.K.; Winking, J.; Gurven, M.; Kaplan, H.; Finch, C.E. Blood Lipids, Infection, and Inflammatory Markers in the Tsimane of Bolivia. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2010, 22, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Sikand, G.; Handu, D.; Rozga, M.; de Waal, D.; Wong, N.D. Medical Nutrition Therapy Provided by Dietitians Is Effective and Saves Healthcare Costs in the Management of Adults with Dyslipidemia. Curr. Atheroscler. Rep. 2023, 25, 331–342. [Google Scholar] [CrossRef]
- Carson, J.A.S.; Lichtenstein, A.H.; Anderson, C.A.M.; Appel, L.J.; Kris-Etherton, P.M.; Meyer, K.A.; Petersen, K.; Polonsky, T.; Van Horn, L. Dietary Cholesterol and Cardiovascular Risk: A Science Advisory From the American Heart Association. Circulation 2020, 141, e39–e53. [Google Scholar] [CrossRef]
- Schoeneck, M.; Iggman, D. The Effects of Foods on LDL Cholesterol Levels: A Systematic Review of the Accumulated Evidence from Systematic Reviews and Meta-Analyses of Randomized Controlled Trials. Nutr. Metab. Cardiovasc. Dis. NMCD 2021, 31, 1325–1338. [Google Scholar] [CrossRef]
- Altschul, R.; Herman, I.H. Influence of Oxygen Inhalation on Cholesterol Metabolism. Arch. Biochem. Biophys. 1954, 51, 308–309. [Google Scholar] [CrossRef]
- Altschul, R.; Hoffer, A.; Stephen, J.D. Influence of Nicotinic Acid on Serum Cholesterol in Man. Arch. Biochem. Biophys. 1955, 54, 558–559. [Google Scholar] [CrossRef] [PubMed]
- Parsons, W.B.; Achor, R.W.; Berge, K.G.; Mckenzie, B.F.; Barker, N.W. Changes in Concentration of Blood Lipids Following Prolonged Administration of Large Doses of Nicotinic Acid to Persons with Hypercholesterolemia: Preliminary Observations. Proc. Staff Meet. Mayo Clin. 1956, 31, 377–390. [Google Scholar] [PubMed]
- The Lipid Research Clinics Coronary Primary Prevention Trial Results. I. Reduction in Incidence of Coronary Heart Disease. JAMA 1984, 251, 351–364. [CrossRef] [PubMed]
- Frick, M.H.; Elo, O.; Haapa, K.; Heinonen, O.P.; Heinsalmi, P.; Helo, P.; Huttunen, J.K.; Kaitaniemi, P.; Koskinen, P.; Manninen, V. Helsinki Heart Study: Primary-Prevention Trial with Gemfibrozil in Middle-Aged Men with Dyslipidemia. Safety of Treatment, Changes in Risk Factors, and Incidence of Coronary Heart Disease. N. Engl. J. Med. 1987, 317, 1237–1245. [Google Scholar] [CrossRef]
- FIELD Study Investigators. Effects of Long-Term Fenofibrate Therapy on Cardiovascular Events in 9795 People with Type 2 Diabetes Mellitus (the FIELD Study): Randomised Controlled Trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef] [PubMed]
- ACCORD Study Group. Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus. N. Engl. J. Med. 2010, 362, 1563–1574. [Google Scholar] [CrossRef] [PubMed]
- Das Pradhan, A.; Glynn, R.J.; Fruchart, J.-C.; MacFadyen, J.G.; Zaharris, E.S.; Everett, B.M.; Campbell, S.E.; Oshima, R.; Amarenco, P.; Blom, D.J.; et al. Triglyceride Lowering with Pemafibrate to Reduce Cardiovascular Risk. N. Engl. J. Med. 2022, 387, 1923–1934. [Google Scholar] [CrossRef]
- Canner, P.L.; Berge, K.G.; Wenger, N.K.; Stamler, J.; Friedman, L.; Prineas, R.J.; Friedewald, W. Fifteen Year Mortality in Coronary Drug Project Patients: Long-Term Benefit with Niacin. J. Am. Coll. Cardiol. 1986, 8, 1245–1255. [Google Scholar] [CrossRef]
- Niacin in Patients with Low HDL Cholesterol Levels Receiving Intensive Statin Therapy. N. Engl. J. Med. 2011, 365, 2255–2267. [CrossRef]
- HPS2-THRIVE Collaborative Group; Landray, M.J.; Haynes, R.; Hopewell, J.C.; Parish, S.; Aung, T.; Tomson, J.; Wallendszus, K.; Craig, M.; Jiang, L.; et al. Effects of Extended-Release Niacin with Laropiprant in High-Risk Patients. N. Engl. J. Med. 2014, 371, 203–212. [Google Scholar] [CrossRef]
- Downs, J.R.; Clearfield, M.; Weis, S.; Whitney, E.; Shapiro, D.R.; Beere, P.A.; Langendorfer, A.; Stein, E.A.; Kruyer, W.; Gotto, J.; et al. Primary Prevention of Acute Coronary Events With Lovastatin in Men and Women With Average Cholesterol LevelsResults of AFCAPS/TexCAPS. JAMA 1998, 279, 1615–1622. [Google Scholar] [CrossRef]
- Sacks, F.M.; Pfeffer, M.A.; Moye, L.A.; Rouleau, J.L.; Rutherford, J.D.; Cole, T.G.; Brown, L.; Warnica, J.W.; Arnold, J.M.O.; Wun, C.-C.; et al. The Effect of Pravastatin on Coronary Events after Myocardial Infarction in Patients with Average Cholesterol Levels|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/nejm199610033351401 (accessed on 5 October 2023).
- Intensive Lipid Lowering with Atorvastatin in Patients with Stable Coronary Disease|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa050461 (accessed on 5 October 2023).
- Scandinavian Simvastatin Survival Study Group. Randomised Trial of Cholesterol Lowering in 4444 Patients with Coronary Heart Disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994, 344, 1383–1389. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.H.; Genest, J.; Gotto, A.M.; Kastelein, J.J.P.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef]
- Cuchel, M.; Meagher, E.A.; Theron, H.; du, T.; Blom, D.J.; Marais, A.D.; Hegele, R.A.; Averna, M.R.; Sirtori, C.R.; Shah, P.K.; et al. Efficacy and Safety of a Microsomal Triglyceride Transfer Protein Inhibitor in Patients with Homozygous Familial Hypercholesterolaemia: A Single-Arm, Open-Label, Phase 3 Study. Lancet 2013, 381, 40–46. [Google Scholar] [CrossRef] [PubMed]
- McGowan, M.P.; Tardif, J.-C.; Ceska, R.; Burgess, L.J.; Soran, H.; Gouni-Berthold, I.; Wagener, G.; Chasan-Taber, S. Randomized, Placebo-Controlled Trial of Mipomersen in Patients with Severe Hypercholesterolemia Receiving Maximally Tolerated Lipid-Lowering Therapy. PLoS ONE 2012, 7, e49006. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa1615664 (accessed on 5 September 2023).
- Nissen, S.E.; Lincoff, A.M.; Brennan, D.; Ray, K.K.; Mason, D.; Kastelein, J.J.P.; Thompson, P.D.; Libby, P.; Cho, L.; Plutzky, J.; et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. N. Engl. J. Med. 2023, 388, 1353–1364. [Google Scholar] [CrossRef]
- Raal, F.J.; Rosenson, R.S.; Reeskamp, L.F.; Hovingh, G.K.; Kastelein, J.J.P.; Rubba, P.; Ali, S.; Banerjee, P.; Chan, K.-C.; Gipe, D.A.; et al. Evinacumab for Homozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 383, 711–720. [Google Scholar] [CrossRef]
- Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa1912387 (accessed on 5 September 2023).
- Schwartz, G.G.; Olsson, A.G.; Ezekowitz, M.D.; Ganz, P.; Oliver, M.F.; Waters, D.; Zeiher, A.; Chaitman, B.R.; Leslie, S.; Stern, T.; et al. Effects of Atorvastatin on Early Recurrent Ischemic Events in Acute Coronary SyndromesThe MIRACL Study: A Randomized Controlled Trial. JAMA 2001, 285, 1711–1718. [Google Scholar] [CrossRef]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.P.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA 2016, 316, 2373–2384. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Menon, V.; Nicholls, S.J.; Brennan, D.; Laffin, L.; Ridker, P.; Ray, K.K.; Mason, D.; Kastelein, J.J.P.; Cho, L.; et al. Bempedoic Acid for Primary Prevention of Cardiovascular Events in Statin-Intolerant Patients. JAMA 2023, 330, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Raal, F.J.; Kallend, D.G.; Jaros, M.J.; Koenig, W.; Leiter, L.A.; Landmesser, U.; Schwartz, G.G.; Lawrence, D.; Friedman, A.; et al. Inclisiran and Cardiovascular Events: A Patient-Level Analysis of Phase III Trials. Eur. Heart J. 2023, 44, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Ernst, N.D.; Cleeman, J.; Mullis, R.; Sooter-Bochenek, J.; Horn, L.V. The National Cholesterol Education Program: Implications for Dietetic Practitioners from the Adult Treatment Panel Recommendations. J. Am. Diet. Assoc. 1988, 88, 1401–1409. [Google Scholar] [CrossRef]
- Grundy, S.M.; Bilheimer, D.; Chait, A.; Clark, L.T.; Denke, M.; Havel, R.J.; Hazzard, W.R.; Hulley, S.B.; Hunninghake, D.B.; Kreisberg, R.A.; et al. Summary of the Second Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 1993, 269, 3015–3023. [Google Scholar] [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- De Backer, G.; Ambrosioni, E.; Borch-Johnsen, K.; Brotons, C.; Cifkova, R.; Dallongeville, J.; Ebrahim, S.; Faergeman, O.; Graham, I.; Mancia, G.; et al. European Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2003, 24, 1601–1610. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N.J. Coordinating Committee of the National Cholesterol Education Program Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J. Am. Coll. Cardiol. 2004, 44, 720–732. [Google Scholar] [CrossRef]
- AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update|Circulation. Available online: https://www.ahajournals.org/doi/full/10.1161/circulationaha.106.174516 (accessed on 5 September 2023).
- Graham, I.; Atar, D.; Borch-Johnsen, K.; Boysen, G.; Burell, G.; Cifkova, R.; Dallongeville, J.; De Backer, G.; Ebrahim, S.; Gjelsvik, B.; et al. European Guidelines on Cardiovascular Disease Prevention in Clinical Practice: Executive Summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by Representatives of Nine Societies and by Invited Experts). Eur. Heart J. 2007, 28, 2375–2414. [Google Scholar] [CrossRef]
- European Association for Cardiovascular Prevention & Rehabilitation; Reiner, Z.; Catapano, A.L.; De Backer, G.; Graham, I.; Taskinen, M.-R.; Wiklund, O.; Agewall, S.; Alegria, E.; Chapman, M.J.; et al. ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur. Heart J. 2011, 32, 1769–1818. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.J.; Lepor, N.E.; Michos, E.D. Evolving Management of Low-Density Lipoprotein Cholesterol: A Personalized Approach to Preventing Atherosclerotic Cardiovascular Disease Across the Risk Continuum. J. Am. Heart Assoc. 2023, 12, e028892. [Google Scholar] [CrossRef] [PubMed]
- Writing Committee; Lloyd-Jones, D.M.; Morris, P.B.; Ballantyne, C.M.; Birtcher, K.K.; Covington, A.M.; DePalma, S.M.; Minissian, M.B.; Orringer, C.E.; Smith, S.C.; et al. 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 80, 1366–1418. [Google Scholar] [CrossRef] [PubMed]
- Turpie, A.G.G. Burden of Disease: Medical and Economic Impact of Acute Coronary Syndromes. Am. J. Manag. Care 2006, 12, S430–S434. [Google Scholar] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef]
- Koskinas, K.C.; Windecker, S.; Pedrazzini, G.; Mueller, C.; Cook, S.; Matter, C.M.; Muller, O.; Häner, J.; Gencer, B.; Crljenica, C.; et al. Evolocumab for Early Reduction of LDL Cholesterol Levels in Patients With Acute Coronary Syndromes (EVOPACS). J. Am. Coll. Cardiol. 2019, 74, 2452–2462. [Google Scholar] [CrossRef]
- Puri, R.; Mehta, V.; Duell, P.B.; Iyengar, S.S.; Yusuf, J.; Dalal, J.; Narasingan, S.N.; Kalra, D.; Kapoor, A.; Pradhan, A.; et al. Evidence for Intensive LDL-C Lowering for Acute Coronary Syndrome: Recommendations from the Lipid Association of India. J. Clin. Lipidol. 2022, 16, 261–271. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef]
- Jellinger, P.S.; Handelsman, Y.; Rosenblit, P.D.; Bloomgarden, Z.T.; Fonseca, V.A.; Garber, A.J.; Grunberger, G.; Guerin, C.K.; Bell, D.S.H.; Mechanick, J.I.; et al. American association of clinical endocrinologists and american college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2017, 23, 1–87. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Lipid Association of India Expert Consensus Statement on Management of Dyslipidemia in Indians 2020: Part III—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33350610/ (accessed on 6 October 2023).
- Rong, S.; Li, B.; Chen, L.; Sun, Y.; Du, Y.; Liu, B.; Robinson, J.G.; Bao, W. Association of Low-Density Lipoprotein Cholesterol Levels with More than 20-Year Risk of Cardiovascular and All-Cause Mortality in the General Population. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2022, 11, e023690. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.-C.; Huh, J.H.; Ryu, S.; Lee, J.-Y.; Scorletti, E.; Byrne, C.D.; Kim, J.Y.; Hyun, D.S.; Ko, S.-B. Low Levels of Low-Density Lipoprotein Cholesterol and Mortality Outcomes in Non-Statin Users. J. Clin. Med. 2019, 8, 1571. [Google Scholar] [CrossRef] [PubMed]
- Penson, P.E.; Long, D.L.; Howard, G.; Toth, P.P.; Muntner, P.; Howard, V.J.; Safford, M.M.; Jones, S.R.; Martin, S.S.; Mazidi, M.; et al. Associations between Very Low Concentrations of Low Density Lipoprotein Cholesterol, High Sensitivity C-Reactive Protein, and Health Outcomes in the Reasons for Geographical and Racial Differences in Stroke (REGARDS) Study. Eur. Heart J. 2018, 39, 3641–3653. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dong, Y.; Qi, X.; Huang, C.; Hou, L. Cholesterol Levels and Risk of Hemorrhagic Stroke: A Systematic Review and Meta-Analysis. Stroke 2013, 44, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Gurol, M.E.; Huang, Z.; Lichtenstein, A.H.; Wang, X.; Wang, Y.; Neumann, S.; Wu, S.; Gao, X. Low-Density Lipoprotein Cholesterol and Risk of Intracerebral Hemorrhage. Neurology 2019, 93, e445–e457. [Google Scholar] [CrossRef] [PubMed]
- Rist, P.M.; Buring, J.E.; Ridker, P.M.; Kase, C.S.; Kurth, T.; Rexrode, K.M. Lipid Levels and the Risk of Hemorrhagic Stroke among Women. Neurology 2019, 92, e2286–e2294. [Google Scholar] [CrossRef]
- Benn, M.; Nordestgaard, B.G.; Grande, P.; Schnohr, P.; Tybjaerg-Hansen, A. PCSK9 R46L, Low-Density Lipoprotein Cholesterol Levels, and Risk of Ischemic Heart Disease: 3 Independent Studies and Meta-Analyses. J. Am. Coll. Cardiol. 2010, 55, 2833–2842. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Mach, F.; Zavitz, K.; Kurtz, C.; Im, K.; Kanevsky, E.; Schneider, J.; Wang, H.; Keech, A.; Pedersen, T.R.; et al. Cognitive Function in a Randomized Trial of Evolocumab. N. Engl. J. Med. 2017, 377, 633–643. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Wiviott, S.D.; Blazing, M.A.; De Ferrari, G.M.; Park, J.-G.; Murphy, S.A.; White, J.A.; Tershakovec, A.M.; Cannon, C.P.; Braunwald, E. Long-Term Safety and Efficacy of Achieving Very Low Levels of Low-Density Lipoprotein Cholesterol. JAMA Cardiol. 2017, 2, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, L.B.; Toth, P.P.; Dearborn-Tomazos, J.L.; Giugliano, R.P.; Hirsh, B.J.; Peña, J.M.; Selim, M.H.; Woo, D. Aggressive LDL-C Lowering and the Brain: Impact on Risk for Dementia and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2023, 43, e404–e442. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Cannon, C.P.; Morrow, D.A.; Ray, K.K.; Pfeffer, M.A.; Braunwald, E. PROVE IT-TIMI 22 Investigators Can Low-Density Lipoprotein Be Too Low? The Safety and Efficacy of Achieving Very Low Low-Density Lipoprotein with Intensive Statin Therapy: A PROVE IT-TIMI 22 Substudy. J. Am. Coll. Cardiol. 2005, 46, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Raichlen, J.S.; Cain, V.A. Statin Therapy Alters the Relationship Between Apolipoprotein B and Low-Density Lipoprotein Cholesterol and Non–High-Density Lipoprotein Cholesterol Targets in High-Risk Patients: The MERCURY II (Measuring Effective Reductions in Cholesterol Using Rosuvastatin TherapY II) Trial. J. Am. Coll. Cardiol. 2008, 52, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Andrews, T.C.; Hsia, J.A.; Kramer, J.H.; Shear, C.; ACCESS Study Group. Atorvastatin Comparative Cholesterol Efficacy and Safety Study Correlation of Non-High-Density Lipoprotein Cholesterol with Apolipoprotein B: Effect of 5 Hydroxymethylglutaryl Coenzyme A Reductase Inhibitors on Non-High-Density Lipoprotein Cholesterol Levels. Am. J. Cardiol. 2001, 88, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Johannesen, C.D.L.; Mortensen, M.B.; Langsted, A.; Nordestgaard, B.G. Apolipoprotein B and Non-HDL Cholesterol Better Reflect Residual Risk Than LDL Cholesterol in Statin-Treated Patients. J. Am. Coll. Cardiol. 2021, 77, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Sniderman, A.D.; Williams, K.; Contois, J.H.; Monroe, H.M.; McQueen, M.J.; de Graaf, J.; Furberg, C.D. A Meta-Analysis of Low-Density Lipoprotein Cholesterol, Non-High-Density Lipoprotein Cholesterol, and Apolipoprotein B as Markers of Cardiovascular Risk. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, T.A.; Ito, M.K.; Maki, K.C.; Orringer, C.E.; Bays, H.E.; Jones, P.H.; McKenney, J.M.; Grundy, S.M.; Gill, E.A.; Wild, R.A.; et al. National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 1—Executive Summary. J. Clin. Lipidol. 2014, 8, 473–488. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Drug | Year of FDA Approval | Mechanism of Action | Major Randomized Controlled Trials |
|---|---|---|---|
| Nicotinic acid (Niacin) | 1950s * | Mechanism not well defined | Coronary Drug Project: Patients with a history of myocardial infarction on nicotinic acid had an 11% lower mortality compared to those on placebo [50]. Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes (AIM-HIGH) and Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) did not demonstrate reductions in vascular events compared to statin monotherapy [51,52]. |
| Bile acid sequestrants (Cholestyramine, Colesevelam, Colestipol) | 1970s * | Increased cholesterol metabolism via bile excretion | Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT): Colestipol reduced the risk of coronary heart disease mortality by 24% in middle-aged men with primary hypercholesterolemia [45]. |
| Fibrates (Gemfibrozil, Fenofibrate) | 1970s * | Promote receptor-mediated LDL-C clearance and increased catabolism of LDL-C | Helsinki Heart Study: Gemfibrozil was associated with a 34% reduction in incident coronary heart disease in middle-aged men with dyslipidemia [46]. FIELD (Fenofibrate Event Lowering and Intervention in Diabetes) and ACCORD (Action to Control Cardiovascular Risk in Diabetes) did not show significant reductions in cardiovascular events with fenofibrate monotherapy or in combination with other lipid-lowering medications [47,48]. |
| Lovastatin | 1987 | Competitive inhibitor of HMG-CoA reductase | Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TEXCAPS): Lovastatin reduced the risk of major coronary events by 37% in patients with moderately elevated cholesterol [53]. |
| Pravastatin | 1991 | Competitive inhibitor of HMG-CoA reductase | Cholesterol and Recurrent Events (CARE): Pravastatin decreased the incidence of fatal coronary events or nonfatal myocardial infarction by 24% in patients with myocardial infarction who had plasma total cholesterol levels below 240 mg/dL [54]. |
| Atorvastatin | 1996 | Competitive inhibitor of HMG-CoA reductase | Treating to New Targets (TNT): Intense lipid lowering with 80 mg/day atorvastatin showed a 22% relative risk reduction in cardiovascular events over treatment with 10 mg/day in patients with stable coronary heart disease [55]. |
| Simvastatin | 1998 | Competitive inhibitor of HMG-CoA reductase | Scandinavian Simvastatin Survival Study (4S): Simvastatin treatment was associated with a 30% reduction in death in patients with coronary heart disease [56]. |
| Rosuvastatin | 2003 | Competitive inhibitor of HMG-CoA reductase | Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER): Rosuvastatin decreased cardiovascular events by 44% in patients with LDL-C < 130 mg/dL but elevated C-reactive protein [57]. |
| Ezetimibe | 2004 | Inhibitor of the NPC1L1 cholesterol transporter | Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT): Ezetimibe-simvastatin therapy provided reduction in LDL-C, with a 6% relative risk reduction in adverse cardiovascular outcomes compared to statin monotherapy [58]. |
| Lomitapide | 2012 | Microsomal triglyceride transfer protein inhibitor | Phase III trials in patients with homozygous familial hypercholesterolemia on current lipid-lowering therapy demonstrate a 50% LDL-C reduction (8.7 mmol/L to 4.3 mmol/L) at 26 weeks [59]. |
| Mipomersen | 2013 | Small interfering RNA inhibitor of apolipoprotein B | A randomized controlled trial of individuals with familial hypercholesterolemia on lipid-lowering therapy showed a 36% reduction in LDL-C and significant reductions in apolipoprotein B [60]. |
| Alirocumab | 2015 | Monoclonal antibody inhibitor of PCSK9 | Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment with Alirocumab (ODYSSEY OUTCOMES): Alirocumab treatment resulted in a relative risk reduction of 15% for ASCVD events compared to the placebo in acute coronary syndrome patients on statin therapy [61]. |
| Evolocumab | 2015 | Monoclonal antibody inhibitor of PCSK9 | Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER): Evolocumab treatment was associated with a relative risk reduction of 15% for ASCVD events in patients with ASCVD on statin therapy [62]. |
| Bempedoic Acid | 2020 | Adenosine triphosphate-citrate lyase inhibitor | Cholesterol Lowering via Bempedoic Acid, an ACL-Inhibiting Regimen (CLEAR OUTCOMES): Bempedoic acid compared to placebo given to patients with statin intolerance showed a reduction in the primary endpoint of death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or coronary revascularization of 13% [63]. |
| Evinacumab | 2021 | Monoclonal antibody inhibitor of angiopoietin-like protein 3 | Evinacumab for Homozygous Familial Hypercholesterolemia (ELIPSE HoFH): Evinacumab decreases LDL-C by 49% in patients with homozygous familial hypercholesterolemia (average LDL-C 255.1 mg/dL) on a maximum background lipid-lowering therapy [64]. |
| Inclisiran | 2021 | Small interfering RNA inhibitor of PCSK9 | Inclisiran for Participants with Atherosclerotic Cardiovascular Disease and Elevated Low-density Lipoprotein Cholesterol (ORION-10 and 11): Inclisiran reduces LDL-C by 50% in ASCVD patients on maximally tolerated statin [65]. Cardiovascular outcomes trials are ongoing. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, J.E.; Tang, K.S.; Barseghian, A.; Wong, N.D. Evolution of More Aggressive LDL-Cholesterol Targets and Therapies for Cardiovascular Disease Prevention. J. Clin. Med. 2023, 12, 7432. https://doi.org/10.3390/jcm12237432
Jones JE, Tang KS, Barseghian A, Wong ND. Evolution of More Aggressive LDL-Cholesterol Targets and Therapies for Cardiovascular Disease Prevention. Journal of Clinical Medicine. 2023; 12(23):7432. https://doi.org/10.3390/jcm12237432
Chicago/Turabian StyleJones, Jeffrey E., Kevin S. Tang, Ailin Barseghian, and Nathan D. Wong. 2023. "Evolution of More Aggressive LDL-Cholesterol Targets and Therapies for Cardiovascular Disease Prevention" Journal of Clinical Medicine 12, no. 23: 7432. https://doi.org/10.3390/jcm12237432