

Combined Neurological Syndrome in Electrohypersensitivity and Multiple Chemical Sensitivity: A Clinical Study of 2018 Cases

Abstract
:
1. Introduction
2. Material and Methods
2.1. Patient Accrual
2.2. Inclusion Criteria
2.3. Patient Inclusion
2.4. Statistical Analysis
3. Results
3.1. Frequency of MCS Associated with EHS
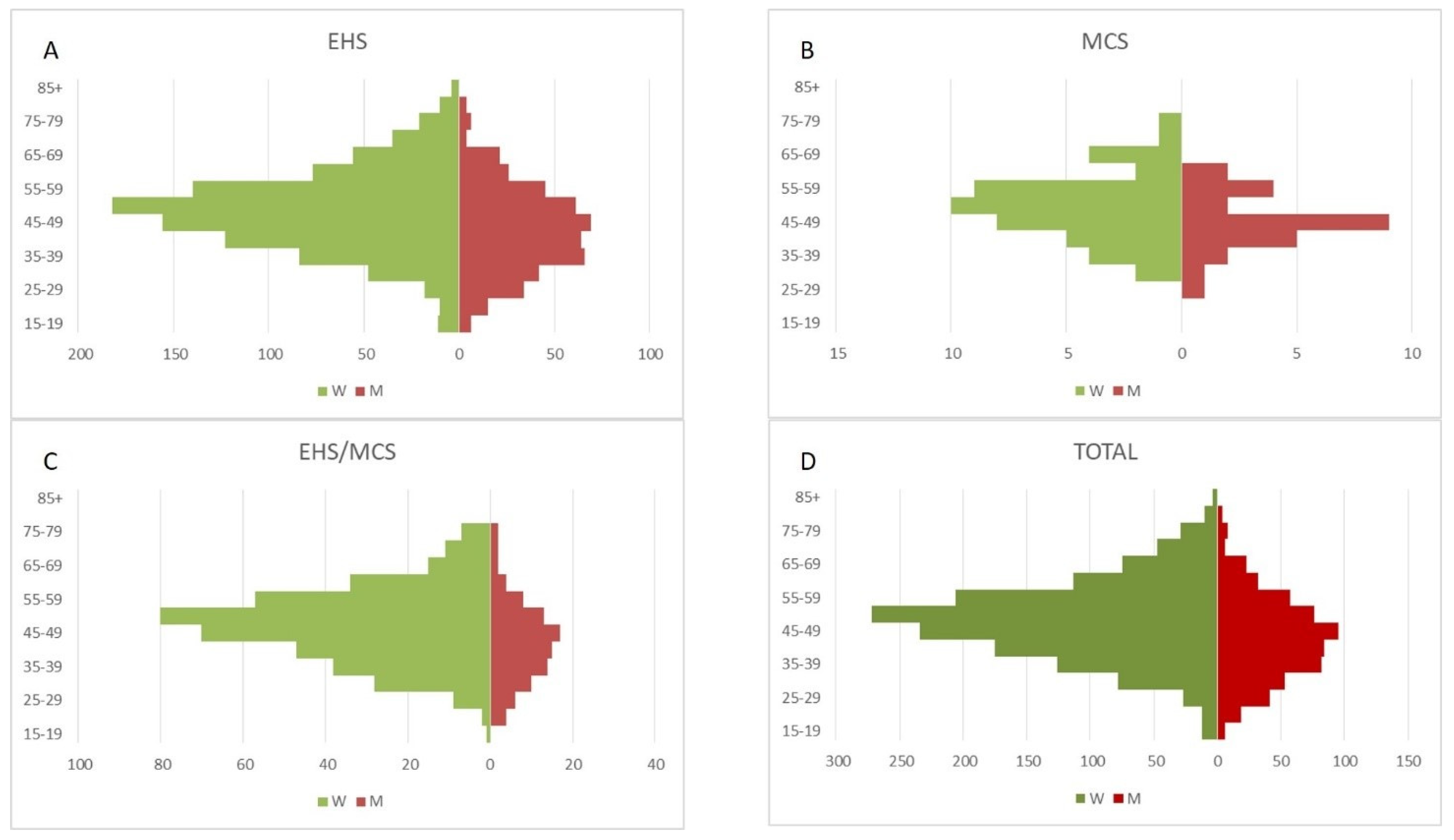
3.2. Demographic Data
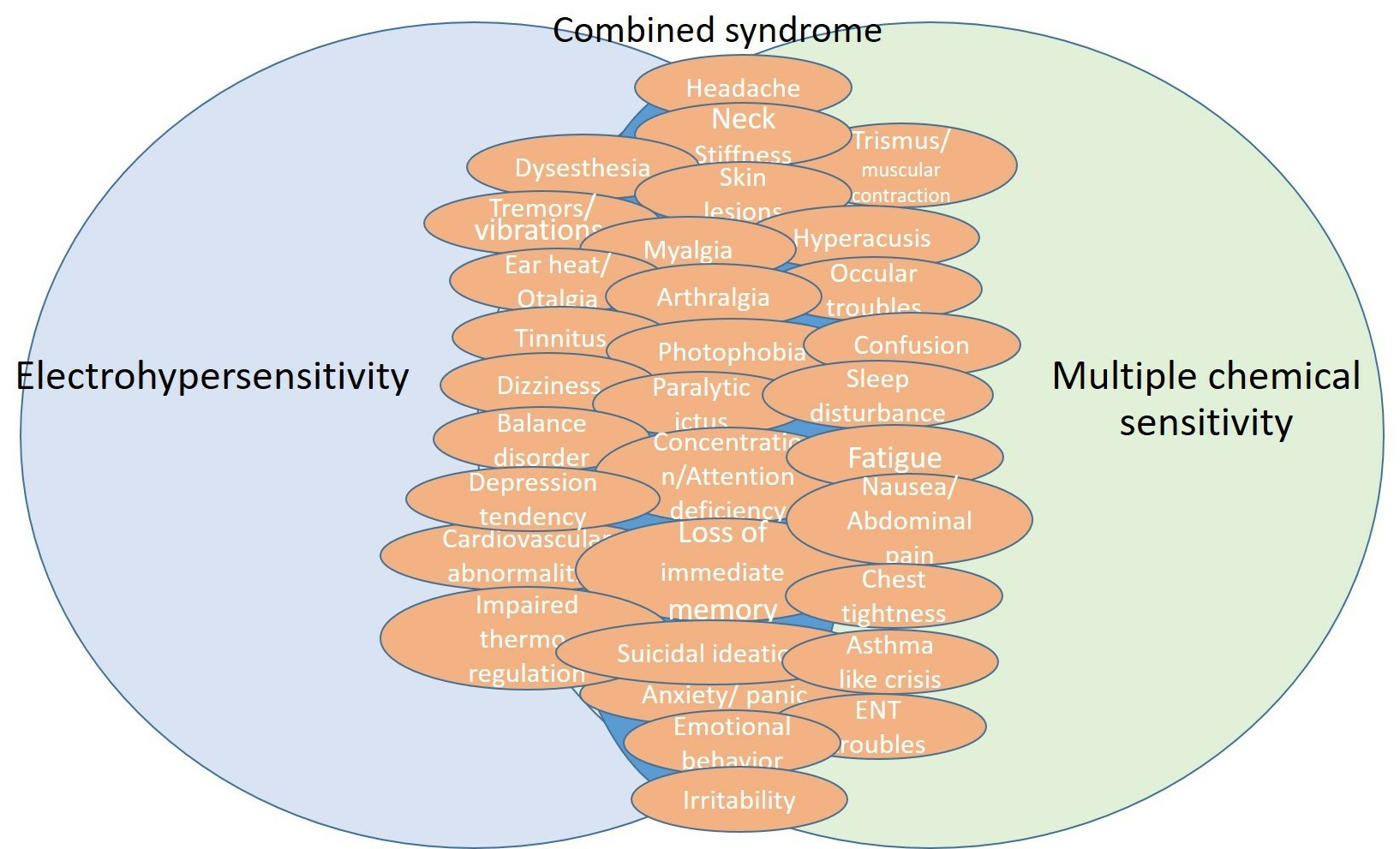
3.3. Symptomatic Presentation
4. Discussion
4.1. Study Limitations
4.2. Demographic Data
4.3. Symptomatic Presentation of EHS and/or MCS
4.4. Toward a Medical Assessment of EHS and/or MCS as Acquired Environmental Sensitivity-Related Somatic Neurological Disorders
4.5. EHS and/or MCS as New Brain Disorders
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Randolph, T.G. Human Ecology and Susceptibility to the Chemical Environment; Charles C Thomas: Springfield, IL, USA, 1962. [Google Scholar]
- Rea, W.J.; Pan, Y.; Fenyves, E.F.; Sujisawa, I.; Suyama, H.; Samadi, N.; Ross, G.H. Electromagnetic field sensitivity. J. Bioelectr. 1991, 10, 214–256. [Google Scholar] [CrossRef]
- Bartha, L.; Baumzweiger, W.; Buscher, D.S.; Callender, T.; Dahl, K.A.; Davidoff, A.; Donnay, A.; Edelson, S.B.; Elson, B.D.; Elliott, E.; et al. Multiple chemical sensitivity: A 1999 consensus. Arch. Environ. Health 1999, 54, 147–149. [Google Scholar]
- Mild, K.H.; Repacholi, M.; van Deventer, E.; Ravazzani, P. Electromagnetic hypersensitivity. In Proceedings of the WHO International Seminar and Working Group Meeting on EMF Hypersensitivity, Prague, Czech Republic, 25–27 October 2004; World Health Organization: Geneva, Switzerland, 2006. ISBN 92-4-159412-8. [Google Scholar]
- WHO (World Health Organization). Electromagnetic Fields and Public Health, Electromagnetic Hypersensitivity; WHO Fact Sheet No. 296; World Health Organization: Geneva, Switzerland, 2005.
- WHO (World Health Organization). Electromagnetic Fields and Public Health: Mobile Phones (October 2014); WHO Updated Fact Sheet No. 193; World Health Organization: Geneva, Switzerland, 2014.
- McCarty, D.E.; Carrubba, S.; Chesson, A.L.; Frilot, C.; Gonzalez-Toledo, E.; Marino, A.A. Electromagnetic Hypersensitivity: Evidence for a Novel Neurological Syndrome. Int. J. Neurosci. 2011, 121, 670–676. [Google Scholar] [CrossRef]
- Belpomme, D.; Campagnac, C.; Irigaray, P. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev. Environ. Health 2015, 30, 251–271. [Google Scholar] [CrossRef]
- Belpomme, D.; Irigaray, P. Electrohypersensitivity as a newly identified and characterized neurologic pathological disorder: How to diagnose, treat, and prevent it. Int. J. Mol. Sci. 2020, 21, 1915. [Google Scholar] [CrossRef] [PubMed]
- Belpomme, D.; Irigaray, P. Why electrohypersensitivity and related symptoms are caused by non-ionizing man-made electromagnetic fields: An overview and medical assessment. Environ. Res. 2022, 212, 113374. [Google Scholar] [CrossRef]
- Irigaray, P.; Caccamo, D.; Belpomme, D. Oxidative stress in electrohypersensitivity self-reporting patients: Results of a prospective in vivo investigation with comprehensive molecular analysis. Int. J. Mol. Med. 2018, 42, 1885–1898. [Google Scholar] [CrossRef] [PubMed]
- Heuser, G.; Heuser, S.A. Functional brain MRI in patients complaining of electrohypersensitivity after long term exposure to electromagnetic fields. Rev. Environ. Health 2017, 32, 291–299. [Google Scholar] [PubMed]
- Lacour, M.; Zunder, T.; Schmidtke, K.; Vaith, P.; Scheidt, C. Multiple chemical sensitivity syndrome (MCS)—Suggestions for an extension of the U.S. MCS-case definition. Int. J. Hyg. Environ. Health 2005, 208, 141–151. [Google Scholar] [CrossRef]
- Bell, I.R.; Miller, C.S.; Schwartz, G.E. An olfactory-limbic model of multiple chemical sensitivity syndrome: Possible relationships to kindling and affective spectrum disorders. Biol. Psychiatry 1992, 32, 218–242. [Google Scholar] [CrossRef]
- Meggs, W.J. Neurogenic inflammation and sensitivity to environmental chemicals. Environ. Health Perspect. 1993, 101, 234–238. [Google Scholar] [CrossRef]
- Meggs, W.J. Hypothesis for induction and propagation of chemical sensitivity based on biopsy studies. Environ. Health Perspect. 1997, 105, 473–478. [Google Scholar]
- Hillert, L.; Musabasic, V.; Berglund, H.; Ciumas, C.; Savic, I. Odor processing in multiple chemical sensitivity. Hum. Brain Mapp. 2007, 28, 172–182. [Google Scholar] [CrossRef]
- Sobel, E.; Davanipour, Z.; Sulkava, R.; Erkinjuntti, T.; Wikstrom, J.; Henderson, V.W.; Buckwalter, G.; Bowman, J.D.; Lee, P. Occupations with exposure to electromagnetic fields: A possible risk factor for Alzheimer’s disease. Am. J. Epidemiol. 1995, 142, 515–524. [Google Scholar] [CrossRef]
- Sobel, E.; Dunn, M.; Davanipour, Z.; Qian, Z.; Chui, H.C. Elevated risk of Alzheimer’s disease among workers with likely electromagnetic field exposure. Neurology 1996, 47, 1477–1481. [Google Scholar] [CrossRef]
- Garcia, A.M.; Sisternas, A.; Hoyos, S.P. Occupational exposure to extremely low frequency electric and magnetic fields and Alzheimer disease: A meta-analysis. Int. J. Epidemiol. 2008, 37, 329–340. [Google Scholar] [CrossRef]
- Davanipour, Z.; Sobel, E. Long-term exposure to magnetic fields and the risks of Alzheimer’s disease and breast cancer: Further biological research. Pathophysiology 2009, 16, 149–156. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Framework for Developing Health-Based EMF Standards; WHO: Geneva, Switzerland, 2006; ISBN 9241594330.
- Belpomme, D.; Carlo, G.L.; Irigaray, P.; Carpenter, D.O.; Hardell, L.; Kundi, M.; Belyaev, I.; Havas, M.; Adlkofer, F.; Heuser, G.; et al. The critical importance of molecular biomarkers and imaging in the study of electrohypersensitivity. A scientific consensus international report. Int. J. Mol. Sci. 2021, 22, 7321. [Google Scholar] [CrossRef]
- Kheifets, L.; Repacholi, M.; Saunders, R.; van Deventer, E. The sensitivity of children to electromagnetic fields. Pediatrics 2005, 116, e303–e313. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Letter from the American Academy of Pediatrics to the FCC Regarding Radiofrequency Electromagnetic Radiation Standards. 29 August 2013. Available online: http://www.wirelesswatchblog.org/wp-content/uploads/2011/06/FCC-13-84-09-03-2013-American-Academy-of-Pediatrics-7520941318-1.pdf (accessed on 6 September 2023).
- Bergqvist, U.; Vogel, E. Possible Health Implications of Subjective Symptoms and Electromagnetic Fields. In A Report Prepared by a European Group of Experts for the European Commission, DGV; Arbete Och Hälsa, 19; Swedish National Institute for Working Life: Stockholm, Sweden, 1997. [Google Scholar]
- Hillert, L.; Berglind, N.; Arnetz, B.B.; Bellander, T. Prevalence of self-reported hypersensitivity to electric or magnetic fields in a population-based questionnaire survey. Scand. J. Work. Environ. Health 2002, 28, 33–41. [Google Scholar] [CrossRef]
- Schreier, N.; Huss, A.; Röösli, M. The prevalence of symptoms attributed to electromagnetic field exposure: A cross-sectional representative survey in Switzerland. Soz. Praventivmed. 2006, 51, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Schüz, J.; Petters, C.; Egle, U.T.; Jansen, B.; Kimbel, R.; Letzel, S.; Nix, W.; Schmidt, L.G.; Vollrath, L. The “Mainzer EMF-Wachhund”: Results from a watchdog project on self-reported health complaints attributed to exposure to electromagnetic fields. Bioelectromagnetics 2006, 27, 280–287. [Google Scholar] [CrossRef]
- Johansson, A.; Nordin, S.; Heiden, M.; Sandström, M. Symptoms, personality traits, and stress in people with mobile phone-related symptoms and electromagnetic hypersensitivity. J. Psychosom. Res. 2010, 68, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Röösli, M.; Mohler, E.; Frei, P. Sense and sensibility in the context of radiofrequency electromagnetic field exposure. C. R. Phys. 2010, 11, 576–584. [Google Scholar] [CrossRef]
- Kato, Y.; Johansson, O. Reported functional impairments of electrohypersensitive Japanese: A questionnaire survey. Pathophysiology 2012, 19, 95–100. [Google Scholar] [CrossRef]
- Baliatsas, C.; van Kamp, I.; Hooiveld, M.; Yzermans, J.; Lebret, E. Comparing non-specific physical symptoms in environmentally sensitive patients: Prevalence, duration, functional status and illness behavior. J. Psychosom. Res. 2014, 76, 405–413. [Google Scholar] [CrossRef]
- Nordin, S.; Neely, G.; Olsson, D.; Sandström, M. Odor and noise intolerance in persons with self-reported electromagnetic hypersensitivity. Int. J. Environ. Res. Public Health 2014, 11, 8794–8805. [Google Scholar] [CrossRef]
- van Dongen, D.; Smid, T.; Timmermans, D.R. Symptom attribution and risk perception in individuals with idiopathic environmental intolerance to electromagnetic fields and in the general population. Perspect. Public Health 2014, 134, 160–168. [Google Scholar] [CrossRef]
- Levallois, P. Hypersensitivity of human subjects to environmental electric and magnetic field exposure: A review of the literature. Environ. Health Perspect. 2002, 110, 613–618. [Google Scholar] [CrossRef]
- Röösli, M. Radiofrequency electromagnetic field exposure and non-specific symptoms of ill health: A systematic review. Environ. Res. 2008, 107, 277–287. [Google Scholar] [CrossRef]
- Hocking, B. Preliminary report: Symptoms associated with mobile phone use. Occup. Med. 1998, 48, 357–360. [Google Scholar] [CrossRef]
- Hocking, B.; Westerman, R. Neurological changes induced by a mobile phone. Occup. Med. 2002, 52, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Frick, U.; Rehm, J.; Eichhammer, P. Risk perception, somatization, and self-report of complaints related to electromagnetic fields—A randomized survey study. Int. J. Hyg. Environ. Health 2002, 205, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Hahn, G.; Everitt, B.S.; Cleare, A.J.; Wessely, S. Are some people sensitive to mobile phone signals? Within participants double blind randomised provocation study. BMJ 2006, 332, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Greco, F.; Garnier, O.; Macioce, V.; Picot, M.C. Prevalence of Migraine Disease in Electrohypersensitive Patients. J. Clin. Med. 2023, 12, 4092. [Google Scholar] [CrossRef]
- Wang, L.; Peng, R.; Hu, X.-J.; Gao, Y.-B.; Wang, S.-M.; Zhao, L.; Dong, J.; Su, Z.-T.; Xu, X.-P.; Gao, R.-L.; et al. Abnormality of synaptic vesicular associated proteins in cerebral cortex and hippocampus after microwave exposure. Synapse 2009, 63, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Dobrek, L.; Thor, P. Glutamate NMDA receptors in pathophysiology and pharmacotherapy of selected nervous system diseases. Postep. Hig. Med. Dosw. 2011, 65, 338–346. [Google Scholar] [CrossRef]
- Suzuki, S.; Seki, M.; Suzuki, N. Recent concept of limbic encephalitis: Progress in anti-NMDA receptor encephalitis. Nihon. Rinsho Meneki Gakkai Kaishi 2013, 36, 86–94. [Google Scholar] [CrossRef]
- Pall, M.L. Elevated nitric oxide/peroxynitrite theory of multiple chemical sensitivity: Central role of N-methyl-D-aspartate receptors in the sensitivity mechanism. Environ. Health Perspect. 2013, 111, 1461–1464. [Google Scholar] [CrossRef]
- Xiong, L.; Sun, C.F.; Zhang, J.; Gao, Y.B.; Wang, L.F.; Zuo, H.Y.; Wang, S.M.; Zhou, H.M.; Xu, X.P.; Dong, J.; et al. Microwave exposure impairs synaptic plasticity in the rat hippocampus and PC12 cells through over-activation of the NMDA receptor signaling pathway. Biomed. Environ. Sci. 2015, 28, 13–24. [Google Scholar]


{kind=link}
{kind=link}
| 2015 Analysis | Present Analysis | |
|---|---|---|
| Evaluable Cases n = 727 | Evaluable Cases n = 2018 | |
| EHS | 521/727 (71.7%) | 1428/2018 (70.8%) |
| MCS | 52/727 (7.1%) * | 85/2018 (4.2%) * |
| EHS/MCS | 154/727 (21.2%) * 154/675 (22.8%) ** | 505/2018 (25%) * 505/1933 (26.1%) ** |
| Total number of evaluable EHS/MCS combined cases * | 484 |
| EHS patients that latter suffered of MCS | 272/484 (56.2%) |
| MCS patients who latter suffered of EHS | 212/484 (43.8%) |
| Demographic Data | EHS | MCS | p * | EHS/MCS | p ** |
|---|---|---|---|---|---|
| Number of cases (%) | 1428 (70.8%) | 85 (4.2%) | - | 505 (25%) | - |
| Age (mean ± SD) | 48.86 ± 12.74 | 49.15 ± 9.71 | 0.84 | 48.57 ± 11.38 | 0.67 |
| Age (median (range)) | 49 (16–85) | 48 (29–77) | - | 49 (19–76) | - |
| Sex ratio (women/men) | 972/456 (68%) | 50/35 (58.8%) | 0.07 | 406/99 (80.4%) | <0.0001 |
| Clinical Symptoms | EHS Ratio (%) | Normal Controls (%) n = 100 | p ** | MCS Ratio (%) | p *** | EHS/MCS Ratio (%) | p **** |
|---|---|---|---|---|---|---|---|
| Headache | 1285/1428 (90%) | 13 | <0.0001 | 76/85 (89%) | 0.86 | 454/505 (90%) | 0.95 |
| Neck stiffness * | 251/783 (32%) | 0 | <0.0001 | 16/51 (31%) | 0.92 | 101/307 (33%) | 0.79 |
| Dysesthesia | 1200/1428 (84%) | 0 | <0.0001 | 60/85 (71%) | 0.001 | 374/505 (74%) | <0.0001 |
| Skin lesions | 228/1428 (16%) | 0 | <0.0001 | 15/85 (18%) | 0.68 | 227/505 (45%) | <0.0001 |
| Tremors/vibrations * | 157/783 (20%) | 0 | <0.0001 | 5/51 (10%) | 0.07 | 61/307 (20%) | 0.95 |
| Myalgia * | 360/783 (46%) | 6 | <0.0001 | 22/51 (43%) | 0.69 | 154/307 (50%) | 0.21 |
| Trismus/muscular contraction * | 62/783 (8%) | 0 | <0.0001 | 1/51 (2%) | 0.12 | 49/307 (16%) | 0.0004 |
| Arthralgia * | 250/783 (32%) | 19 | 0.008 | 14/51 (27%) | 0.51 | 83/307 (27%) | 0.11 |
| Ear heat/otalgia * | 493/783 (63%) | 0 | <0.0001 | 22/51 (43%) | 0.004 | 166/307 (54%) | 0.0013 |
| Tinnitus | 914/1428 (64%) | 5 | <0.0001 | 34/85 (40%) | <0.0001 | 313/505 (62%) | 0.42 |
| Hyperacusis | 500/1428 (35%) | 6 | <0.0001 | 26/85 (31%) | 0.41 | 278/505 (55%) | <0.0001 |
| Photophobia * | 260/783 (33%) | 0 | <0.0001 | 14/51 (27.5%) | 0.92 | 90/307 | 0.41 (29.4%) |
| Ocular troubles | 472/1428 (33%) | 0 | <0.0001 | 38/85 (45%) | 0.03 | 222/505 (44%) | <0.0001 |
| Paralytic ictus * | 78/783 (10%) | 0 | <0.0001 | 7/51 (14%) | 0.39 | 46/307 (15%) | 0.02 |
| Dizziness | 985/1428 (69%) | 0 | <0.0001 | 43/85 (51%) | 0.0004 | 303/505 (60%) | 0.0002 |
| Balance disorder | 485/1428 (34%) | 0 | <0.0001 | 30/85 (35%) | 0.80 | 116/505 (23%) | <0.0001 |
| Concentration/attention deficiency | 1114/1428 (78%) | 0 | <0.0001 | 55/85 (65%) | 0.004 | 424/505 (84%) | 0.002 |
| Loss of immediate memory | 1085/1428 (76%) | 6 | <0.0001 | 57/85 (67%) | 0.06 | 394/505 (78%) | 0.35 |
| Confusion * | 47/783 (6%) | 0 | <0.0001 | 2/51 (4%) | 0.54 | 46/307 (15%) | <0.0001 |
| Sleep disturbance | 1071/1428 (75%) | 6 | <0.0001 | 43/85 (51%) | <0.0001 | 409/505 (81%) | 0.006 |
| Fatigue | 1200/1428 (84%) | 10 | <0.0001 | 41/51 (80%) | 0.49 | 444/505 (88%) | 0.04 |
| Depression tendency | 814/1428 (57%) | 0 | <0.0001 | 26/85 (30%) | <0.0001 | 237/505 (47%) | <0.0001 |
| Suicidal ideation | 229/1428 (16%) | 0 | <0.0001 | 9/85 (11%) | 0.18 | 91/505 (18%) | 0.30 |
| Anxiety/panic | 372/1428 (26%) | 0 | <0.0001 | 31/85 (36%) | 0.03 | 152/505 (30%) | 0.08 |
| Emotional behavior | 186/1428 (13%) | 11 | 0.56 | 13/85 (15%) | 0.55 | 75/505 (15%) | 0.30 |
| Irritability | 328/1428 (23%) | 6 | <0.0001 | 15/85 (18%) | 0.25 | 126/505 (25%) | 0.37 |
| Nausea/abdominal pain * | 141/783 (18%) | 0 | <0.0001 | 8/51 (16%) | 0.67 | 101/307 (33%) | <0.0001 |
| Cardiovascular abnormalities | 657/1428 (46%) | 0 | <0.0001 | 36/85 (42%) | 0.51 | 253/505 (50%) | 0.11 |
| Chest tightness * | 94/783 (12%) | 2 | <0.0001 | 29/51 (56%) | <0.0001 | 172/307 (56%) | <0.0001 |
| Asthma-like crisis * | 47/783 (6%) | 0 | <0.0001 | 22/51 (43%) | <0.0001 | 132/307 (43%) | <0.0001 |
| ENT (ear, nose, and throat) troubles * | 94/783 (12%) | 4 | <0.0001 | 44/51 (86%) | <0.0001 | 92/307 (30%) | <0.0001 |
| Impaired thermoregulation | 186/1428 (13%) | 0 | 0.02 | 5/85 (6%) | 0.05 | 25/505 (5%) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belpomme, D.; Irigaray, P. Combined Neurological Syndrome in Electrohypersensitivity and Multiple Chemical Sensitivity: A Clinical Study of 2018 Cases. J. Clin. Med. 2023, 12, 7421. https://doi.org/10.3390/jcm12237421
Belpomme D, Irigaray P. Combined Neurological Syndrome in Electrohypersensitivity and Multiple Chemical Sensitivity: A Clinical Study of 2018 Cases. Journal of Clinical Medicine. 2023; 12(23):7421. https://doi.org/10.3390/jcm12237421
Chicago/Turabian StyleBelpomme, Dominique, and Philippe Irigaray. 2023. "Combined Neurological Syndrome in Electrohypersensitivity and Multiple Chemical Sensitivity: A Clinical Study of 2018 Cases" Journal of Clinical Medicine 12, no. 23: 7421. https://doi.org/10.3390/jcm12237421