
Effect of Mobilization with Movement on Pain, Disability, and Range of Motion in Patients with Shoulder Pain and Movement Impairment: A Systematic Review and Meta-Analysis
 ,
,  and
and
Abstract
:1. Introduction
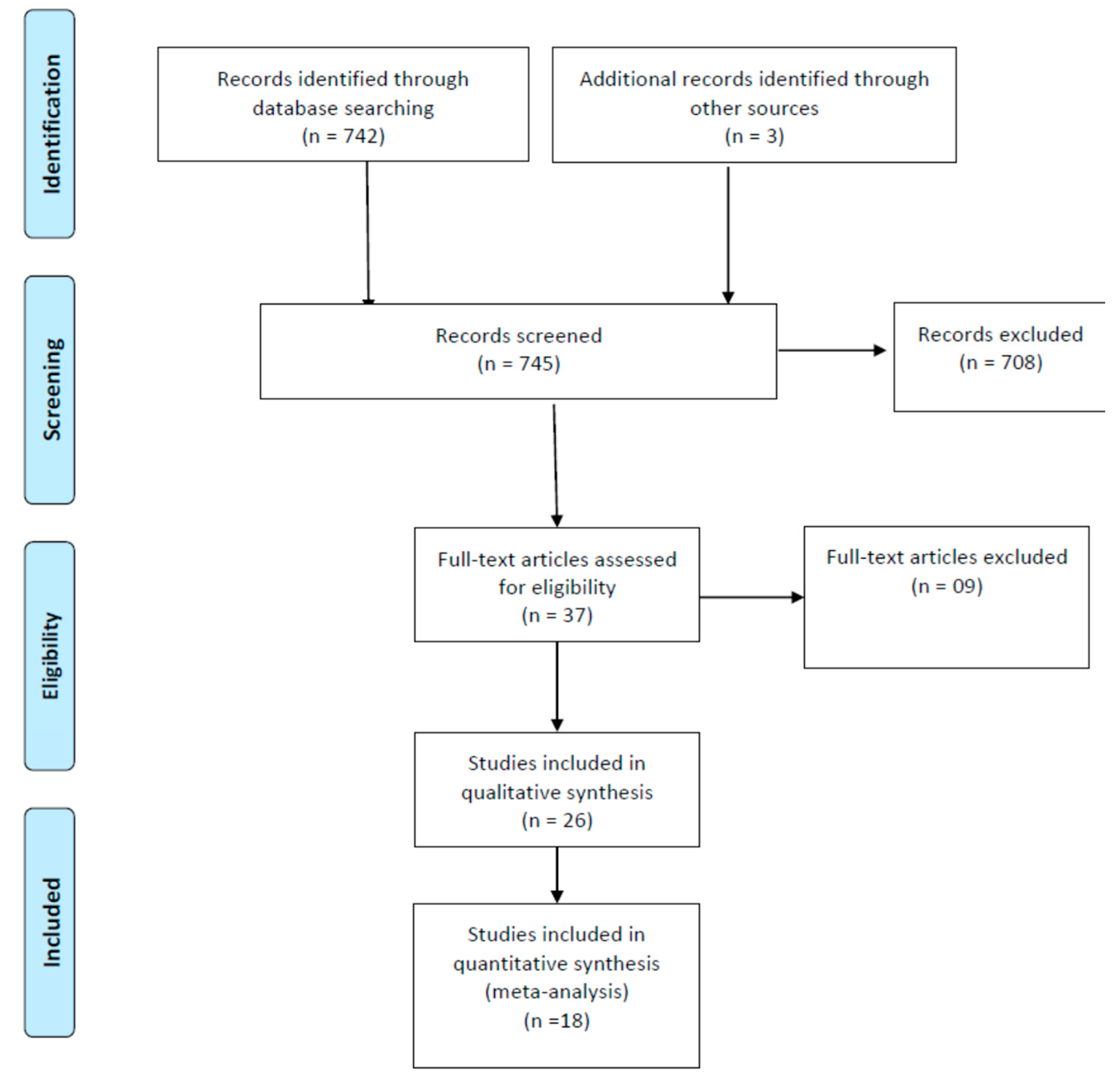
2. Methods
3. Results
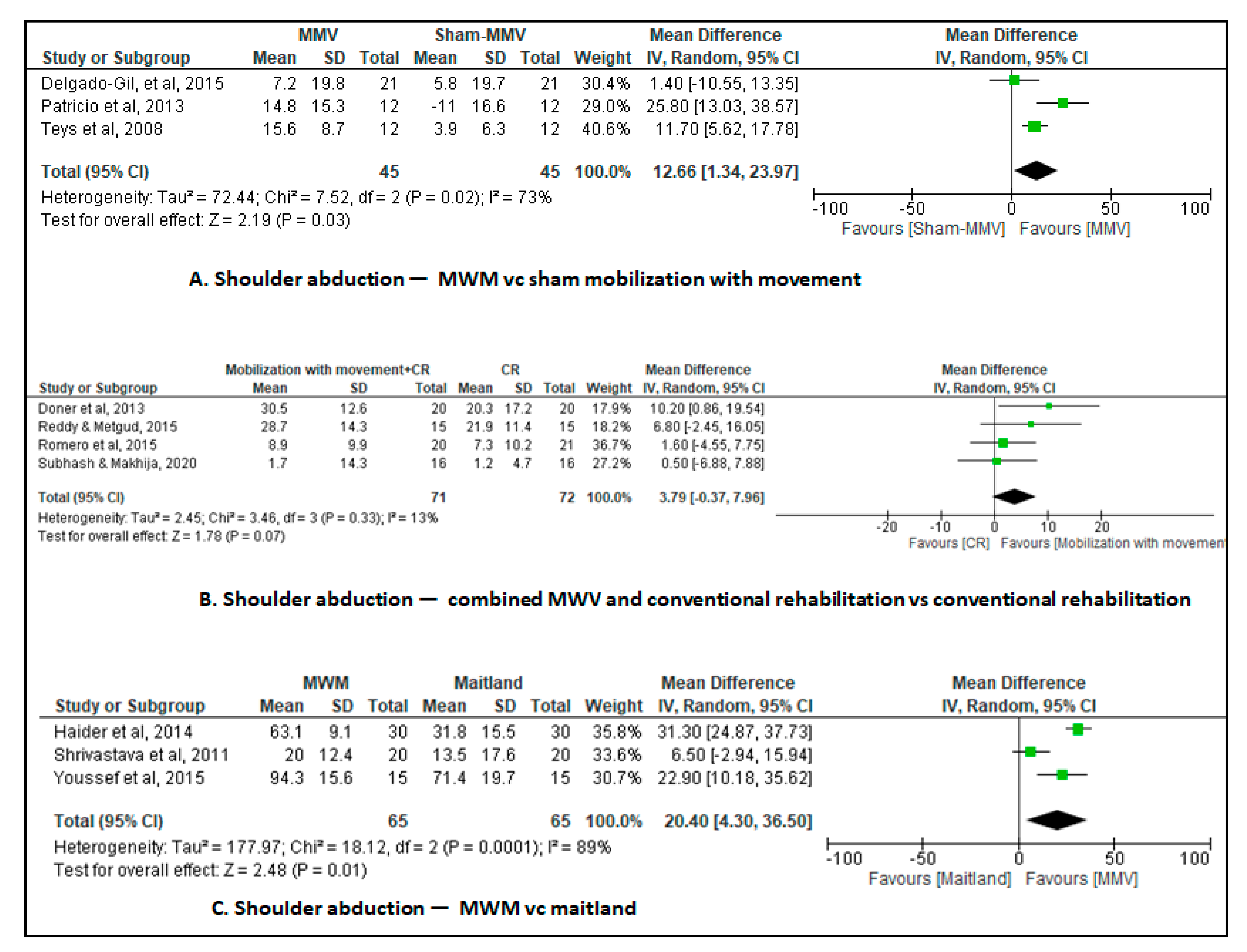
3.1. Mobilization with Movement vs. Sham Mobilization with Movement
Combined Mobilization with Movement and Conventional Rehabilitation versus Conventional Rehabilitation
3.2. Combined Mobilization with Movement and Conventional Rehabilitation vs. Conventional Rehabilitation
3.3. Mobilization with Movement vs. Exercise
3.4. Combined Mobilization with Movement and Conventional Rehabilitation vs. Conventional Rehabilitation
3.5. Mobilization with Movement vs. Sham Mobilization with Movement
3.6. Combined Mobilization with Movement and Conventional Rehabilitation vs. Conventional Rehabilitation
3.7. Mobilization with Movement vs. End Range Mobilization
3.8. Combined Mobilization with Movement and Conventional Rehabilitation vs. Conventional Rehabilitation
3.9. Mobilization with Movement vs. End Range Mobilization
3.10. Combined Mobilization with Movement and Conventional Rehabilitation vs. Conventional Rehabilitation
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McClure, P.W.; Michener, L.A. Staged Approach for Rehabilitation Classification: Shoulder Disorders (STAR-Shoulder). Phys. Ther. 2015, 95, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Adebajo, A.; Hay, E.; Carr, A. Shoulder pain: Diagnosis and management in primary care. BMJ 2005, 331, 1124–1128. [Google Scholar] [CrossRef]
- Cadogan, A.; Laslett, M.; Hing, W.A.; McNair, P.J.; Coates, M.H. A prospective study of shoulder pain in primary care: Prevalence of imaged pathology and response to guided diagnostic blocks. BMC Musculoskelet. Disord. 2011, 12, 119. [Google Scholar] [CrossRef] [PubMed]
- Pennella, D.; Giagio, S.; Maselli, F.; Giovannico, G.; Roncone, A.; Fiorentino, F.; Brindisino, F. Red flags useful to screen for gastrointestinal and hepatic diseases in patients with shoulder pain: A scoping review. Musculoskelet. Care 2022, 20, 721–730. [Google Scholar] [CrossRef]
- House, J.; Mooradian, A. Evaluation and management of shoulder pain in primary care clinics. South. Med. J. 2010, 103, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Ryösä, A.; Laimi, K.; Äärimaa, V.; Lehtimäki, K.; Kukkonen, J.; Saltychev, M. Surgery or conservative treatment for rotator cuff tear: A meta-analysis. Disabil. Rehabil. 2017, 39, 1357–1363. [Google Scholar] [CrossRef]
- Noten, S.; Meeus, M.; Stassijns, G.; Van Glabbeek, F.; Verborgt, O.; Struyf, F. Efficacy of Different Types of Mobilization Techniques in Patients with Primary Adhesive Capsulitis of the Shoulder: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 815–825. [Google Scholar] [CrossRef]
- Do Moon, G.; Lim, J.Y.; Kim, D.Y.; Kim, T.H. Comparison of Maitland and Kaltenborn mobilization techniques for improving shoulder pain and range of motion in frozen shoulders. J. Phys. Ther. Sci. 2015, 27, 1391–1395. [Google Scholar] [CrossRef]
- Hing, W.; Bigelow, R.; Bremner, T. Mulligan’s mobilization with movement: A review of the tenets and prescription of MWMs. N. Z. J. Physiother. 2008, 36, 144–164. [Google Scholar]
- Anggiat, L.; Altavas, A.J.; Budhyanti, W. Joint Mobilization: Theory and evidence review. Int. J. Sport. Exerc. Health Res. 2020, 4, 86–90. [Google Scholar] [CrossRef]
- Ho, C.Y.; Sole, G.; Munn, J. The effectiveness of manual therapy in the management of musculoskeletal disorders of the shoulder: A systematic review. Man. Ther. 2009, 14, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulos, N.; Dimitriadis, Z.; Koumantakis, G.A. Effectiveness of mulligan’s mobilization with movement techniques on range of motion in peripheral joint pathologies: A Systematic review with meta-analysis between 2008 and 2018. J. Manip. Physiol. Ther. 2019, 42, 439–449. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane. 2021. Available online: www.training.cochrane.org/handbook (accessed on 12 February 2022).
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.N.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to assess the quality of randomized controlled trials: A systematic review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Macedo, L.G.; Elkins, M.R.; Maher, C.G.; Moseley, A.M.; Herbert, R.D.; Sherrington, C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J. Clin. Epidemiol. 2010, 63, 920–925. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating of quality randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Review Manager (RevMan) [Computer Program], Version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Chandrasekaran, K.; Sundaram, M.; Senthil Selvam, P.; Viswanath Reddy, A.; Senthilkumar, S.; Rathnapandi, V. A comparative study on the effectiveness of Mulligan mobilization versus Positional release therapy technique in patients with Adhesive capsulitis. Int. J. Res. Pharm. Sci. 2021, 12, 1–5. [Google Scholar] [CrossRef]
- Rana, A.A.; Fatima, S.; Sajjad, S.A.; Niaz, M.; Hayat, M.K.; Ahmad, I. Effectiveness of Maitland vs. Mulligan Mobilization Techniques in Adhesive Capsulitis of Shoulder Joint. Pak. J. Med. Health Sci. 2021, 15, 2561–2564. [Google Scholar] [CrossRef]
- Fernandes, A.; Shah, L.; Mohan, A. Effectiveness of Kaltenborn Mobilization Technique Versus Mulligan’s MWM in Patients with Adhesive Capsulitis of Shoulder. Indian J. Physiother. Occup. Ther. 2020, 14, 18–24. [Google Scholar]
- Subhash, R.; Makhija, M. Effectiveness of Mobilization with Movement in weight bearing position on pain, shoulder range of motion and function in patients with shoulder dysfunction. Indian J. Public. Health Res. Dev. 2020, 11, 901–905. [Google Scholar]
- Menek, B.; Tarakci, D.; Algun, Z.C. The effect of Mulligan mobilization on pain and life quality of patients with Rotator cuff syndrome: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2019, 32, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Ragav, S.; Singh, A. Comparison of Effectiveness of Mulligan ‘MWM’ Technique versus Kaltenborn Mobilization Technique on Pain and End Range of Motion in Patients with Adhesive Capsulitis of Shoulder Joint: A Randomized Controlled Trial. J. Exerc. Sci. Physiother. 2019, 15, 1–9. [Google Scholar] [CrossRef]
- Rayudu, G.M.; Alagingi, N.K. Efficacy of mulligan technique versus muscle energy technique on Functional ability in subjects with adhesive capsulitis. Int. J. Recent. Sci. Res. 2018, 9, 25638–25641. [Google Scholar] [CrossRef]
- Srivastava, S.; Eapen, C.; Mittal, H. Comparison of Mobilisation with Movement and Cryotherapy in Shoulder Impingement Syndrome-A Randomised Clinical Trial. J. Clin. Diagn. Res. 2018, 12, 1–5. [Google Scholar] [CrossRef]
- Yeole, U.L.; Dighe, P.D.; Gharote, G.M.; Panse, R.S.; Kulkarni, S.A.; Pawar, P.A. Effectiveness of movement with mobilization in adhesive capsulitis of shoulder: Randomized controlled trial. Indian J. Med. Res. Pharm. Sci. 2017, 4, 1–8. [Google Scholar]
- Guimarães, J.F.; Salvini, T.F.; Siqueira, A.L., Jr.; Ribeiro, I.L.; Camargo, P.R.; Alburquerque-Sendín, F. Immediate Effects of Mobilization with Movement vs Sham Technique on Range of Motion, Strength, and Function in Patients with Shoulder Impingement Syndrome: Randomized Clinical Trial. J. Manip. Physiol. Ther. 2016, 39, 605–615. [Google Scholar] [CrossRef]
- Arshad, H.S.; Shah, I.H.; Nasir, R.H. Comparison of Mulligan Mobilization with Movement and End-Range Mobilization Following Maitland Techniques in Patients with Frozen Shoulder in Improving Range of Motion. Int. J. Health Sci. Res. 2015, 4, 2761–2767. [Google Scholar]
- Neelapala, R.; Reddy, R.S.; Danait, R. Effect of Mulligan’s posterolateral glide on shoulder rotator strength, scapular upward rotation in shoulder pain subjects—A randomized controlled trial. J. Musculoskelet. Res. 2016, 19, 1650014. [Google Scholar] [CrossRef]
- Delgado-Gil, J.A.; Prado-Robles, E.; Rodrigues-de-Souza, D.P.; Cleland, J.A.; Fernández-de-las-Peñas, C.; Alburquerque-Sendín, F. Effects of mobilization with movement on pain and range of motion in patients with unilateral shoulder impingement syndrome: A randomized controlled trial. J. Manip. Physiol. Ther. 2015, 38, 245–252. [Google Scholar] [CrossRef]
- Reddy, B.C.; Metgud, S. A randomized controlled trial to investigate the effect of Mlligan’s MWM and conventional therapy in stage II Adhesive capsulitis. Indian. J. Phys. Ther. 2015, 3, 55–59. [Google Scholar]
- Romero, C.; Torres Lacomba, M.; Castilla Montoro, Y.; Prieto Merino, D.; Pacheco da Costa, S.; Velasco Marchante, M.J. Mobilization with Movement for Shoulder Dysfunction in Older Adults: A Pilot Trial. J. Chiropr. Med. 2015, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Satpute, K.H.; Bhandari, P.; Hall, T. Efficacy of hand behind back mobilization with movement for acute shoulder pain and movement impairment: A randomized controlled trial. J. Manip. Physiol. Ther. 2015, 38, 324–334. [Google Scholar] [CrossRef]
- Youssef, A.R.; Ibrahim, A.M.A.; Ayad, K.E. Mulligan mobilization is more effective in treating diabetic frozen shoulder than the maitland technique. Int. J. Physiother. 2015, 2, 804–810. [Google Scholar] [CrossRef]
- Haider, R.; Ahmad, A.; Saum-re-Zahra Hanif, M.K. To compare effects of maitland and mulligan’s mobilization techniques in the treatment of frozen shoulder. Annals 2014, 20, 257–264. [Google Scholar]
- Doner, G.; Guven, Z.; Atalay, A.; Celiker, R. Evaluation of Mulligan’s technique for adhesive capsulitis of the shoulder. J. Rehabil. Med. 2013, 45, 87–91. [Google Scholar] [CrossRef]
- Patrício, R.I.T. Efeitos Imediatos da Mobilização com Movimento na Dor, Amplitude de Movimento e Actividade Electromiográfica dos Músculos da Cintura Escapular em Indivíduos com Síndrome do Conflito Subacromial. Master’s Thesis, Escola Superior de Tecnologia da Saúde do Porto, Instituto Politécnico do Porto, Vila Nova de Gaia, Portugal, 2013. [Google Scholar]
- Teys, P.; Bisset, L.; Collins, N.; Coombes, B.; Vicenzino, B. One-week time course of the effects of Mulligan’s Mobilisation with Movement and taping in painful shoulders. Man. Ther. 2013, 18, 372–377. [Google Scholar] [CrossRef]
- Djordjevic, O.C.; Vukicevic, D.; Katunac, L.; Jovic, S. Mobilization with movement and kinesiotaping compared with a supervised exercise program for painful shoulder: Results of a clinical trial. J. Manip. Physiol. Ther. 2012, 35, 454–463. [Google Scholar] [CrossRef]
- Shrivastava, A.; Shyam, A.K.; Sabnis, S.; Sancheti, P. Randomized Controlled Study of Mulligan’s Vs. Maitland’s Mobilization Technique in Adhesive Capsulitis of Shoulder Joint. Indian J. Physiother. Occup. Ther. Int. J. 2011, 5, 12–15. [Google Scholar]
- Kachingwe, A.F.; Phillips, B.; Sletten, E.; Plunkett, S.W. Comparison of manual therapy techniques with therapeutic exercise in the treatment of shoulder impingement: A randomized controlled pilot clinical trial. J. Man. Manip. Ther. 2008, 16, 238–247. [Google Scholar] [CrossRef]
- Teys, P.; Bisset, L.; Vicenzino, B. The initial effects of a Mulligan’s mobilization with movement technique on range of movement and pressure pain threshold in pain-limited shoulders. Man. Ther. 2008, 13, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.L.; Chang, C.W.; Chen, S.Y.; Wang, S.F.; Lin, J.J. Mobilization techniques in subjects with frozen shoulder syndrome: Randomized multiple-treatment trial. Phys. Ther. 2007, 87, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Hao, Q.; Devji, T.; Zeraatkar, D.; Wang, Y.; Qasim, A.; Siemieniuk, R.A.C. Minimal important differences for improvement in shoulder condition patient-reported outcomes: A systematic review to inform a BMJ Rapid Recommendation. BMJ Open 2019, 9, e028777. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Groups | Intervention | Volume (Repetition Sets) | Frequency (Times a Week) | Time (Minutes) | Duration (Week) |
|---|---|---|---|---|---|---|
| Chandrasekaran et al., 2021 [20] | Mobilization with movement (n = 15) Positional release technique (n = 15) | Mobilization with movement Positional release technique | NR | NR | NR | 2 |
| Rana et al., 2021 [21] | Mobilization with movement (n = 20) Maitland mobilization (n = 20) | Mobilization with movement + conventional exercises Maitland mobilization + conventional exercises | NR | NR | NR | 6 |
| Fernandes et al., 2020 [22] | Group M—Mobilization with movement (n = 28) Group K—Kaltenborn (n = 28) | Mobilization with movement Kaltenborn mobilization | 3 × 10 | 3 | NR | 2 |
| Subhash and Makhija, 2020 [23] | Mobilization with movement (n = 16) Control group (n = 16) | Mobilization with movement + Conventional physiotherapy Conventional physiotherapy | 3 × 7 | 1 | NR | 2 |
| Menek et al., 2018 [24] | Mobilization with movement (n = 15) Control group (n = 15) | Mobilization with movement + Conventional physiotherapy Conventional physiotherapy | 3 × 10 | 3 | 20 | NR |
| Ragav and Singh, 2019 [25] | Group A—Mobilization with movement (n = 10) Group B—Kaltenborn (n = 10) Control C—Control group (n = 10) | Mobilization with movement Kaltenborn mobilization Hot water fomentation and home-based range of motion exercises program of the shoulder joint | 3 × 10 | 6 | NR | 3 |
| Rayudu and Alagingi, 2018 [26] | Mobilization with movement (n = 30) Control group (n = 30) | Mobilization with movement + Conventional exercises Muscle energy technique + conventional exercises | 3 × 10 | 3 | NR | 3 |
| Srivastava et al., 2018 [27] | Mobilization with movement (n = 11) Cryotherapy (n = 11) | Mobilization with movement + impairment-based exercises Cryotherapy + impairment-based exercises | 3 × 10 | 1 | NR | 1 |
| Yeole et al., 2017 [28] | Mobilization with movement (n = 15) Control group (n = 15) | Mobilization with movement + Supervised exercises Supervised exercises | NR | 1 | NR | 1 |
| Neelapala et al., 2016 [31] | Mobilization with movement (n = 15) Control group (15) | Mobilization with movement Supervised exercises | NR | 3 | NR | 1 |
| Guimarães et al. 2016 [29] | Mobilization with movement (n = 14) Control group (n = 13) | Mobilization with movement + Sham Sham + mobilization with movement | 3 × 10 | 2 | NR | 3 |
| Delgado Gil et al. 2015 [32] | Mobilization with movement (n = 21) Control group (n = 21) | Mobilization with movement Sham | 3 × 10 | 2 | 10 | 2 |
| Romero et al. 2015 [34] | Mobilization with movement (n = 22) Control group (n = 22) | Mobilization with movement + standard physiotherapy Standard physiotherapy | 3 × 10 | 3 | 20 | 2 |
| Satpute et al. 2015 [35] | Mobilization with movement (n = 22) Control group (n = 22) | Mobilization with movement + exercise + hot pack Exercise + hot pack | 3 × 10 | 3 | NR | 3 |
| Reddy and Metgud, 2015 [33] | Mobilization with movement (n = 15) Control group (n = 15) | Mobilization with movement + conventional physiotherapy Conventional physiotherapy | 3 × 10 | 15 sessions followed | NR | 2 |
| Youssef et al., 2015 [36] | Mobilization with movement (n = 15) Control group (n = 15) | Mobilization with movement + conventional physiotherapy Conventional Physiotherapy | 3 × 10 | 3 | NR | 6 |
| Haider et al., 2014 [37] | Mobilization with movement (n = 60) Control group (n = 60) | Mobilization with movement Maitland’s technique | NR | NR | 30 | 8 |
| Arshad et al., 2015 [30] | Mobilization with movement (n = 50) Control group (n = 50) | Mobilization with movement + Ultrasound + transcutaneus electrical nerve stimulation + home plan for exercises Maitland + ultrasound + transcutaneus electrical nerve stimulation + home plan for exercises | NR | 2 | NR | 8 |
| Doner et al. 2013 [38] | Mobilization with movement (n = 20) Control group (n = 20) | Hot pack + transcutaneus electrical nerve stimulation + mobilization with movement Hot pack + transcutaneus electrical nerve stimulation + stretching | 3 × 10 | 5 | NR | 3 |
| Patrício et al. 2013 [39] | Mobilization with movement (n = 12) Control group (n = 12) | Mobilization with movement Placebo | 3 × 10 | 2 | 30 | 3 |
| Teys et al. 2013 [40] | Mobilization with movement (n = 13) Control group (n = 12) | Mobilization with movement Mobilization with movement + tape | 3 × 10 | 1 | NR | 2 |
| Djordjevic et al., 2012 [41] | Mobilization with movement (n = 10) Control group (n = 10) | Mobilization with movement + Kinesio-taping Supervised exercises | 3 × 10 | 5 | NR | 2 |
| Shrivastava et al. 2011 [42] | Mobilization with movement (n = 20) Grupo Intervenção (n = 20) | Mobilization with movement + hot pack + exercises Maitland + hot pack + exercises | NR | 6 | NR | 2 |
| Kachingwe et al., 2008 [43] | Exercises (n = 8) Exercises + Manual mobilization (n = 9) Mobilization with movement (n = 9) Control group (n = 7) | Supervised exercises Supervised exercises + glenoumeral mobilization; Supervisioned exercises + mobilization with movement Control group with orientations | 3 × 10 | NR | NR | NR |
| Teys et al. 2008 [44] | Mobilization with movement (n = 12) Control group (n = 12) | Mobilization with movement Sham mobilization with movement | 3 × 10 | 3 | NR | 1 |
| Yang et al. 2007 [45] | Mobilization with movement (n = 14) Control group (n = 14) | Mobilization with movement Middle and end range mobilization | 3 × 10 | 2 | 30 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias, D.; Neto, M.G.; Sales, S.d.S.R.; Cavalcante, B.d.S.; Torrierri, P., Jr.; Roever, L.; Araújo, R.P.C.d. Effect of Mobilization with Movement on Pain, Disability, and Range of Motion in Patients with Shoulder Pain and Movement Impairment: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 7416. https://doi.org/10.3390/jcm12237416
Dias D, Neto MG, Sales SdSR, Cavalcante BdS, Torrierri P Jr., Roever L, Araújo RPCd. Effect of Mobilization with Movement on Pain, Disability, and Range of Motion in Patients with Shoulder Pain and Movement Impairment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(23):7416. https://doi.org/10.3390/jcm12237416
Chicago/Turabian StyleDias, Daniela, Mansueto Gomes Neto, Stephane da Silva Ribeiro Sales, Bárbara dos Santos Cavalcante, Palmiro Torrierri, Jr., Leonardo Roever, and Roberto Paulo Correia de Araújo. 2023. "Effect of Mobilization with Movement on Pain, Disability, and Range of Motion in Patients with Shoulder Pain and Movement Impairment: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 23: 7416. https://doi.org/10.3390/jcm12237416