
The Effects of Heparan Sulfate Infusion on Endothelial and Organ Injury in a Rat Pneumosepsis Model

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Information
2.2. Pneumosepsis Model
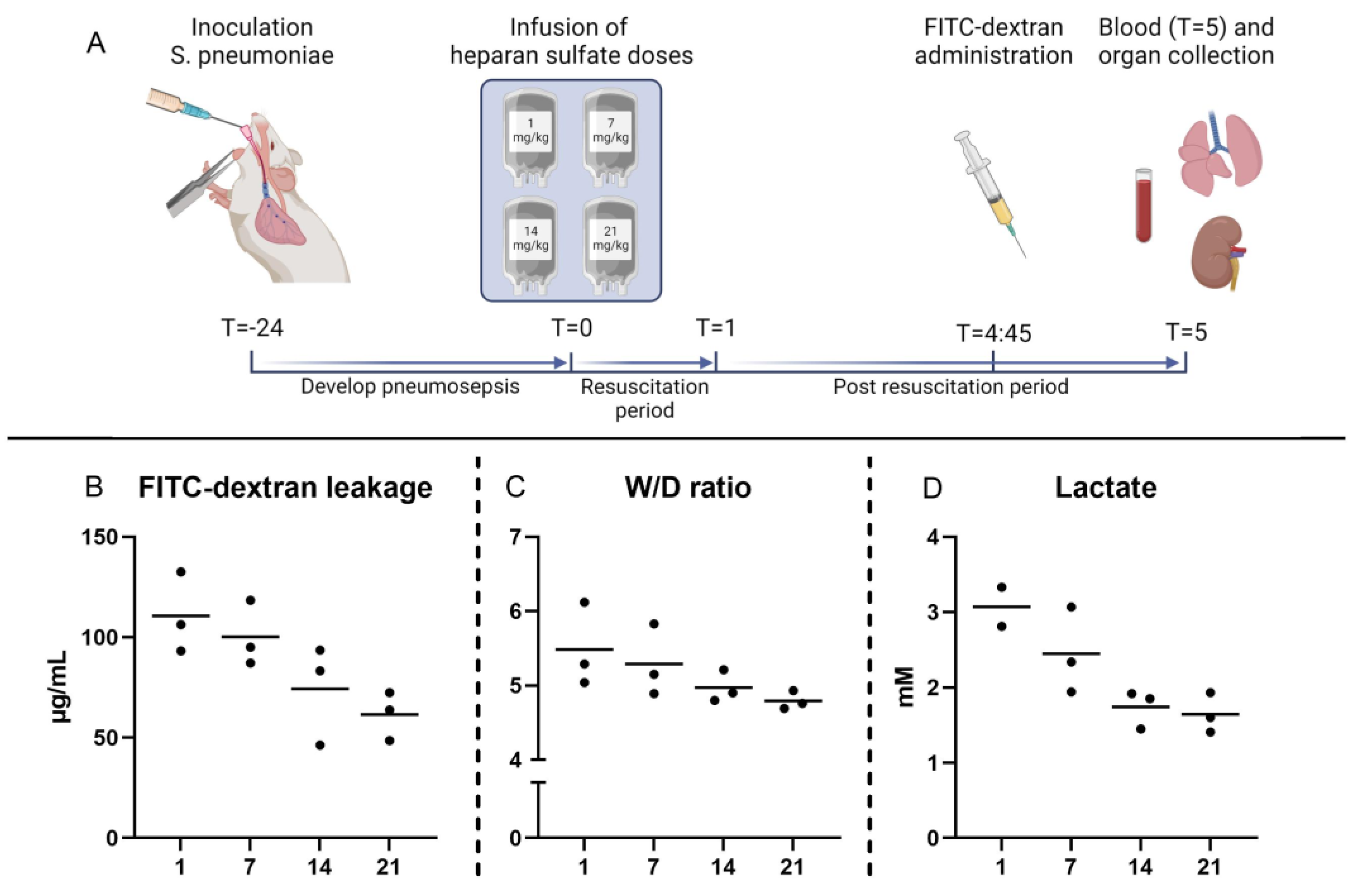
2.3. Dose–Response Study
2.4. Animal Welfare
2.5. Measurements
2.6. Pulmonary Vascular Leakage
2.7. Histopathology
2.8. Bacterial Growth
2.9. Sample Size and Statistical Analyses
3. Results
3.1. Pneumosepsis Model
3.2. Effects of Heparan Sulfate on Pulmonary Injury
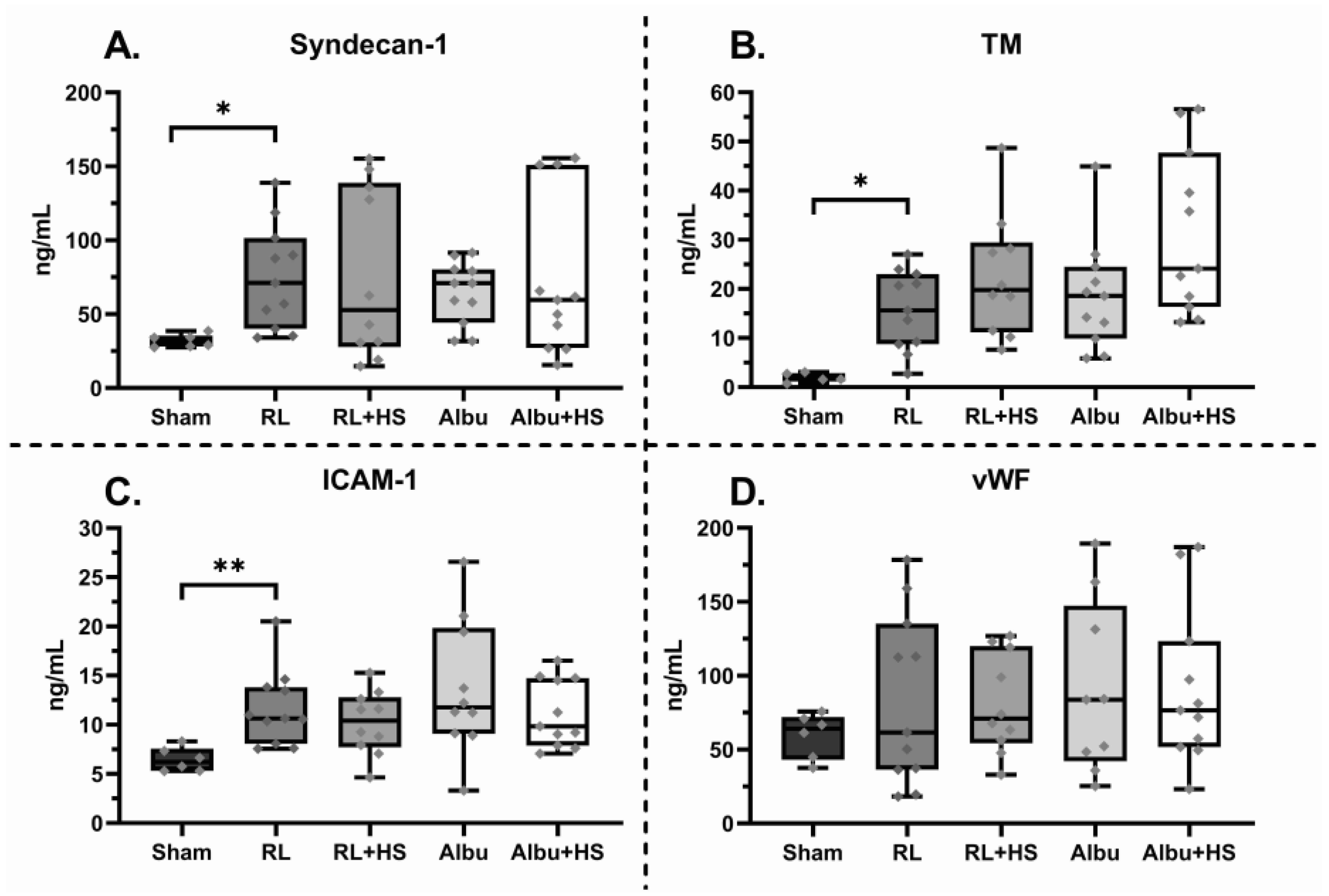
3.3. Effects of Heparan Sulfate on Systemic Injury
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Sham (n = 6) | RL (n = 11) | RL + HS (n = 11) | Albu (n = 10) | Albu + HS (n = 11) |
|---|---|---|---|---|---|
| Interstitial inflammation | 0 (0–1) | 2 * (1–2) | 2 * (1–3) | 2 (1–2) | 1 * (0–2) |
| Endothelialitis | 0 (0–0) | 1 * (0–2) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Bronchitis | 0 (0–0) | 3 * (1–3) | 3 * (3–4) | 3 * (2–3) | 4 * (3–4) |
| Edema | 0 (0–1) | 3 * (1–3) | 3 * (3–4) | 3 * (3–3) | 4 * (3–4) |
| Thrombi formation | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |


| Fur Aspect | Actively Grooming | Dulling of Hair Coat | Rough Hard Coat | Piloerection |
|---|---|---|---|---|
| Activity | Normal | Reduced activity disturbed | No activity disturbed Reduced activity stimulated | Nil activity disturbed or stimulated |
| Behavior | Normal, no abd splinting | Slightly hunched, moving freely, mild splinting | Hunched with stiff movement/posture, moderate splinting | Hunched with no movement stimulated, severe splinting |
| Face | Normal | Normal eyelid opening when disturbed | Orbital tightening, moderate grimacing | Eyelids closed, obvious grimacing |
| Diarrhea | None | Mild | Moderate | Severe |
| Respiratory distress | None | Mild dyspnea | Moderate dyspnea | Severe dyspnea with abdominal breathing |
| Score | 1 | 2 | 3 | 4 |
References
- Vincent, J.-L.; Jones, G.; David, S.; Olariu, E.; Cadwell, K.K. Frequency and mortality of septic shock in Europe and North America: A systematic review and meta-analysis. Crit. Care 2019, 23, 196. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.; Stensballe, J.; Ostrowski, S. Shock induced endotheliopathy (SHINE) in acute critical illness—A unifying pathophysiologic mechanism. Crit. Care 2017, 21, 25. [Google Scholar] [CrossRef]
- Moore, K.H.; Murphy, H.A.; George, E.M. The glycocalyx: A central regulator of vascular function. Am. J. Physiol. Integr. Comp. Physiol. 2021, 320, R508–R518. [Google Scholar] [CrossRef] [PubMed]
- Oshima, K.; King, S.I.; McMurtry, S.A.; Schmidt, E.P. Endothelial Heparan Sulfate Proteoglycans in Sepsis: The Role of the Glycocalyx. Semin. Thromb. Hemost. 2021, 47, 274–282. [Google Scholar] [CrossRef]
- Ding, R.; Meng, Y.; Ma, X. The Central Role of the Inflammatory Response in Understanding the Heterogeneity of Sepsis-3. BioMed Res. Int. 2018, 2018, 5086516. [Google Scholar] [CrossRef] [PubMed]
- Steppan, J.; Hofer, S.; Funke, B.; Brenner, T.; Henrich, M.; Martin, E.; Weitz, J.; Hofmann, U.; Weigand, M.A. Sepsis and Major Abdominal Surgery Lead to Flaking of the Endothelial Glycocalix. J. Surg. Res. 2011, 165, 136–141. [Google Scholar] [CrossRef]
- Deutschman, C.S.; Hellman, J.; Roca, R.F.; De Backer, D.; Coopersmith, C.M.; Antonelli, M.; Evans, L.; Ferrer-Roca, R.; Jog, S.; Kesecioglu, J.; et al. The surviving sepsis campaign: Basic/translational science research priorities. Intensiv. Care Med. Exp. 2020, 8, 31. [Google Scholar] [CrossRef]
- Uchimido, R.; Schmidt, E.P.; Shapiro, N.I. The glycocalyx: A novel diagnostic and therapeutic target in sepsis. Crit. Care 2019, 23, 16. [Google Scholar] [CrossRef]
- Colbert, J.F.; Schmidt, E.P. Endothelial and Microcirculatory Function and Dysfunction in Sepsis. Clin. Chest Med. 2016, 37, 263–275. [Google Scholar] [CrossRef]
- Nelson, A.; Berkestedt, I.; Bodelsson, M. Circulating glycosaminoglycan species in septic shock. Acta Anaesthesiol. Scand. 2014, 58, 36–43. [Google Scholar] [CrossRef]
- Zhang, F.; Zheng, L.; Cheng, S.; Peng, Y.; Fu, L.; Zhang, X.; Linhardt, R.J. Comparison of the Interactions of Different Growth Factors and Glycosaminoglycans. Molecules 2019, 24, 3360. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Haeger, S.M.; Suflita, M.A.; Zhang, F.; Dailey, K.L.; Colbert, J.F.; Ford, J.A.; Picon, M.A.; Stearman, R.S.; Lin, L.; et al. Fibroblast Growth Factor Signaling Mediates Pulmonary Endothelial Glycocalyx Reconstitution. Am. J. Respir. Cell Mol. Biol. 2017, 56, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Henry, C.B.S.; Duling, B.R.; McClatchey, P.M.; Schafer, M.; Hunter, K.S.; Reusch, J.E.B.; Filho, I.P.T.; Torres, L.N.; Salgado, C.; Dubick, M.A.; et al. Permeation of the luminal capillary glycocalyx is determined by hyaluronan. Am. J. Physiol. Circ. Physiol. 1999, 277, H508–H514. [Google Scholar] [CrossRef]
- Liu, J.; Pedersen, L.C. Anticoagulant heparan sulfate: Structural specificity and biosynthesis. Appl. Microbiol. Biotechnol. 2007, 74, 263–272. [Google Scholar] [CrossRef]
- Liao, Y.-E.; Liu, J.; Arnold, K. Heparan sulfates and heparan sulfate binding proteins in sepsis. Front. Mol. Biosci. 2023, 10, 1146685. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Haeger, S.M.; Yang, Y.; Dailey, K.L.; Ford, J.A.; Schmidt, E.P. Circulating Heparan Sulfate Fragments Attenuate Histone-Induced Lung Injury Independently of Histone Binding. Shock 2017, 48, 666–673. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; Emerson, M.; et al. Reporting animal research: Explanation and elaboration for the ARRIVE guidelines 2.0. PLoS Biol. 2020, 18, e3000411. [Google Scholar] [CrossRef]
- Watkins, J.M.; Spain, D.A.; Krysztopik, R.J.; Downard, P.J.; Wilson, M.A.; Garrison, R. Heparan Preserves Intestinal Perfusion after Hemorrhage and Resuscitation. J. Surg. Res. 1996, 66, 154–158. [Google Scholar] [CrossRef]
- Liao, Y.-E.; Xu, Y.; Arnold, K.; Zhang, F.; Li, J.; Sellers, R.; Yin, C.; Pagadala, V.; Inman, A.M.; Linhardt, R.J.; et al. Using heparan sulfate octadecasaccharide (18-mer) as a multi-target agent to protect against sepsis. 2023, 120, e2209528120. Proc. Natl. Acad. Sci. USA 2023, 120, e2209528120. [Google Scholar] [CrossRef]
- Huet, O.; Ramsey, D.; Miljavec, S.; Jenney, A.; Aubron, C.; Aprico, A.; Stefanovic, N.; Balkau, B.; Head, G.A.; de Haan, J.B.; et al. Ensuring Animal Welfare While Meeting Scientific Aims Using a Murine Pneumonia Model of Septic Shock. Shock 2013, 39, 488–494. [Google Scholar] [CrossRef]
- Chang, R.; Holcomb, J.B.; Johansson, P.I.; Pati, S.; Schreiber, M.A.; Wade, C.E. Plasma Resuscitation Improved Survival in a Cecal Ligation and Puncture Rat Model of Sepsis. Shock 2018, 49, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Esko, J.D. Demystifying Heparan Sulfate–Protein Interactions. Annu. Rev. Biochem. 2014, 83, 129–157. [Google Scholar] [CrossRef]
- Marques, C.; Reis, C.A.; Vivès, R.R.; Magalhães, A. Heparan Sulfate Biosynthesis and Sulfation Profiles as Modulators of Cancer Signalling and Progression. Front. Oncol. 2021, 11, 778752. [Google Scholar] [CrossRef] [PubMed]
- Oshima, K.; Haeger, S.M.; Hippensteel, J.A.; Herson, P.S.; Schmidt, E.P. More than a biomarker: The systemic consequences of heparan sulfate fragments released during endothelial surface layer degradation (2017 Grover Conference Series). Pulm. Circ. 2018, 8, 2045893217745786. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.; Berkestedt, I.; Schmidtchen, A.; Ljunggren, L.; Bodelsson, M. Increased levels of glycosaminoglycans during septic shock: Relation to mortality and the antibacterial actions of plasma. Shock 2008, 30, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.B.; Brunn, G.J.; Kodaira, Y.; Platt, J.L. Receptor-mediated monitoring of tissue well-being via detection of soluble heparan sulfate by Toll-like receptor 4. J. Immunol. 2002, 168, 5233–5239. [Google Scholar] [CrossRef]
- Fannon, M.; Forsten, K.E.; Nugent, M.A. Potentiation and inhibition of bFGF binding by heparin: A model for regulation of cellular response. Biochemistry 2000, 39, 1434–1445. [Google Scholar] [CrossRef]
- Krufka, A.; Guimond, S.; Rapraeger, A.C. Two hierarchies of FGF-2 signaling in heparin: Mitogenic stimulation and high-affinity binding/receptor transphosphorylation. Biochemistry 1996, 35, 11131–11141. [Google Scholar] [CrossRef]
- Hippensteel, J.A.; Uchimido, R.; Tyler, P.D.; Burke, R.C.; Han, X.; Zhang, F.; McMurtry, S.A.; Colbert, J.F.; Lindsell, C.J.; Angus, D.C.; et al. Intravenous fluid resuscitation is associated with septic endothelial glycocalyx degradation. Crit. Care 2019, 23, 259. [Google Scholar] [CrossRef]
- Lat, I.; Coopersmith, C.M.; De Backer, D. The Surviving Sepsis Campaign: Fluid Resuscitation and Vasopressor Therapy Research Priorities in Adult Patients. Crit. Care Med. 2021, 49, 623–635. [Google Scholar] [CrossRef]



| Parameter | Sham (n = 6) | RL (n = 11) | RL + HS (n = 11) | Albu (n = 11) | Albu + HS (n = 11) |
|---|---|---|---|---|---|
| Weight loss (%) | 0.9 (0.3–1.4) | 7.5 * (6.9–9.5) | 8.2 * (7.3–8.7) | 8.2 * (7.4–9.3) | 7.8 * (7.3–8.5) |
| Vitals | |||||
| Heart rate (bpm) | 370 (344–385) | 367 (340–377) | 340 (314–360) | 365 (338–381) | 364 (324–379) |
| Saturation (%) | 97 (95–99) | 98 (97–99) | 96 (94–98) | 95 (93–98) | 97 (93–98) |
| Blood count | |||||
| Hb (mM) | 10.1 (10.0–11.1) | 10.6 (10.0–12.0) | 11.5 (10.6–11.9) | 11.1 (10.8–11.7) | 11.7 (10.2–12.2) |
| Leukocytes (*109/L) | 12.0 (7.1–14.6) | 2.6 * (1.1–8.6) | 2.7 (1.6–4.5) | 4.1 * (1.5–9.1) | 1.9 * (1.3–2.9) |
| Platelets (*109/L) | 965 (743–989) | 678 * (452–865) | 621 * (353–812) | 775 (580–917) | 668 * (546–849) |
| Blood gas | |||||
| Lactate (mM) | 1.98 (1.62–2.05) | 2.55 * (2.37–2.72) | 2.77 * (2.36–2.83) | 2.51 * (2.41–3.04) | 2.71 * (2.50–2.79) |
| pH | 7.42 (7.41–7.44) | 7.43 (7.42–7.45) | 7.44 (7.39–7.45) | 7.41 (7.38–7.44) | 7.44 (7.40–7.46) |
| BE (mM) | 3.2 (2.1–4.6) | 4.6 (3.6–5.9) | 6.0 * (5.0–6.6) | 4.6 (2.6–6.9) | 5.3 * (4.2–6.1) |
| HCO3− (mM) | 28.2 (27.2–29.8) | 30.2 * (28.0–32.0) | 31.8 * (30.2–33.5) | 31.0 * (28.6–32.2) | 30.7 * (29.9–32.4) |
| Natrium (mM) | 138 (137–139) | 139 (137–139) | 139 (138–139) | 139 (138–140) | 139 (137–140) |
| Potassium (mM) | 5.3 (5.1–5.4) | 5.9 * (5.3–6.6) | 5.9 * (5.3–6.1) | 5.6 * (5.4–5.8) | 5.7 * (5.4–5.9) |
| Calcium (mM) | 1.21 (1.19–1.25) | 1.12 * (1.04–1.17) | 1.12 * (1.08–1.15) | 1.16 * (1.09–1.19) | 1.09 * (1.07–1.16) |
| Glucose (mM) | 8.9 (7.5–12.2) | 8.0 (7.4–8.9) | 7.2 (6.9–8.5) | 7.6 (7.4–9.5) | 7.2 (6.7–7.7) |
| Parameter | Sham (n = 6) | RL (n = 11) | RL + HS (n = 11) | Albu (n = 10) | Albu + HS (n = 11) |
|---|---|---|---|---|---|
| Blood gas | |||||
| Lactate (mM) | 1.56 (0.87–1.69) | 2.24 * (2.10–2.71) | 2.18 * (2.00–2.89) | 2.12 * (2.04–2.67) | 2.74 * (2.08–2.99) |
| Hb (mM) | 8.9 (8.3–9.4) | 10.1 * (9.4–11.6) | 10.9 * (10.4–12.5) | 10.4 * (9.6–10.9) | 11.7 * (10.3–12.7) |
| Glucose (mM) | 10.3 (9.5–11.6) | 8.2 * (7.1–9.4) | 6.9 * (6.5–7.4) | 7.9 * (7.6–8.1) | 7.6 * (6.6–8.3) |
| HCO3− (mM) | 29.9 (27.5–32.8) | 29.4 (26.6–30.5) | 30.6 (28.4–31.1) | 30.8 (30–32.6) | 28.7 (25.6–30.2) |
| Saturation (%) | 98 (98–99) | 94 (90–96) | 96 (94–97) | 96 (92–96) | 94 (93–97) |
| Organ injury | |||||
| ALT (U/L) | 34.0 (30.8–38.3) | 35.0 (30.0–38.3) | 32.0 (25.8–39) | 34.5 (29.8–37.3) | 32.5 (25.8–35.3) |
| AST (U/L) | 64.5 (59.8–73.5) | 75.0 (54.0–82.5) | 92.0 (61.8–101.5) | 86.0 (62.0–95.5) | 66.0 (58.5–99.0) |
| Albumin (g/L) | 36.5 (33.5–39.0) | 36.0 (34.0–38.0) | 35 (33.5–37.3) | 37 (35.5–38.3) | 35 (32.8–37.3) |
| Creatinine (µM) | 23.5 (19.5–28.3) | 23.0 (21.8–25) | 22 (20–25.5) | 21.0 (20.0–25.0) | 23.0 (22.0–24.8) |
| Kidney W/D ratio | 3.6 (3.4–4.0) | 3.9 * (3.7–4.1) | 3.9 * (3.8–4.0) | 4.0 * (3.7–4.1) | 3.9 * (3.9–4.1) |
| Inflammation | |||||
| IL-6 plasma | 12.4 (12.4–12.4) | 262.3 * (67.6–1119.9) | 349.7 * (142.0–619.4) | 567.4 * (329.5–1311.5) | 745.7 * (117.4–971.6) |
| IL-6 lung homogenate (ng/mL) | 18.0 (16.1–19.0) | 21.9 (18.7–35.4) | 36.1 * (31.8–47.1) | 41.6 * (24.1–46.0) | 41.6 * (30.5–45.1) |
| TNF-α lung homogenate (ng/mL) | 5.0 (4.8–6.4) | 10.6 (5.4–15.2) | 14.4 * (12.6–23.6) | 18.0 * (11.9–28.8) | 12.4 * (11.0–25.7) |
| Lung homogenate bacterial outgrowth (CFU/gram) | 0 * (0–0) | 6.0 × 107 * (1.0 × 107–1.3 × 108) | 6.0 × 107 * (3.4 × 107–1.6 × 108) | 7.0 × 107 * (1.3 × 107–3.6 × 108) | 8.1 × 107 * (6 × 107–1.6 × 108) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Brink, D.P.; Kleinveld, D.J.B.; Bongers, A.; Vos, J.; Roelofs, J.T.H.; Weber, N.C.; van Buul, J.D.; Juffermans, N.P. The Effects of Heparan Sulfate Infusion on Endothelial and Organ Injury in a Rat Pneumosepsis Model. J. Clin. Med. 2023, 12, 6438. https://doi.org/10.3390/jcm12206438
van den Brink DP, Kleinveld DJB, Bongers A, Vos J, Roelofs JTH, Weber NC, van Buul JD, Juffermans NP. The Effects of Heparan Sulfate Infusion on Endothelial and Organ Injury in a Rat Pneumosepsis Model. Journal of Clinical Medicine. 2023; 12(20):6438. https://doi.org/10.3390/jcm12206438
Chicago/Turabian Stylevan den Brink, Daan P., Derek J. B. Kleinveld, Annabel Bongers, Jaël Vos, Joris T. H. Roelofs, Nina C. Weber, Jaap D. van Buul, and Nicole P. Juffermans. 2023. "The Effects of Heparan Sulfate Infusion on Endothelial and Organ Injury in a Rat Pneumosepsis Model" Journal of Clinical Medicine 12, no. 20: 6438. https://doi.org/10.3390/jcm12206438