

Diagnostic Efficacy of Serum Asialo α1-Acid Glycoprotein Levels for Advanced Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Compared to That in Healthy Subjects: A Prospective Study
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Liver Stiffness Assessment
2.3. Measurement of Serum AsAGP Level
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Result
3.1. Baseline Characteristics
3.2. Serum AsAGP Level Accroding to Fibrosis Stages
3.3. Correlation between Serum AsAGP Level and Baseline Variables including Liver Stiffness
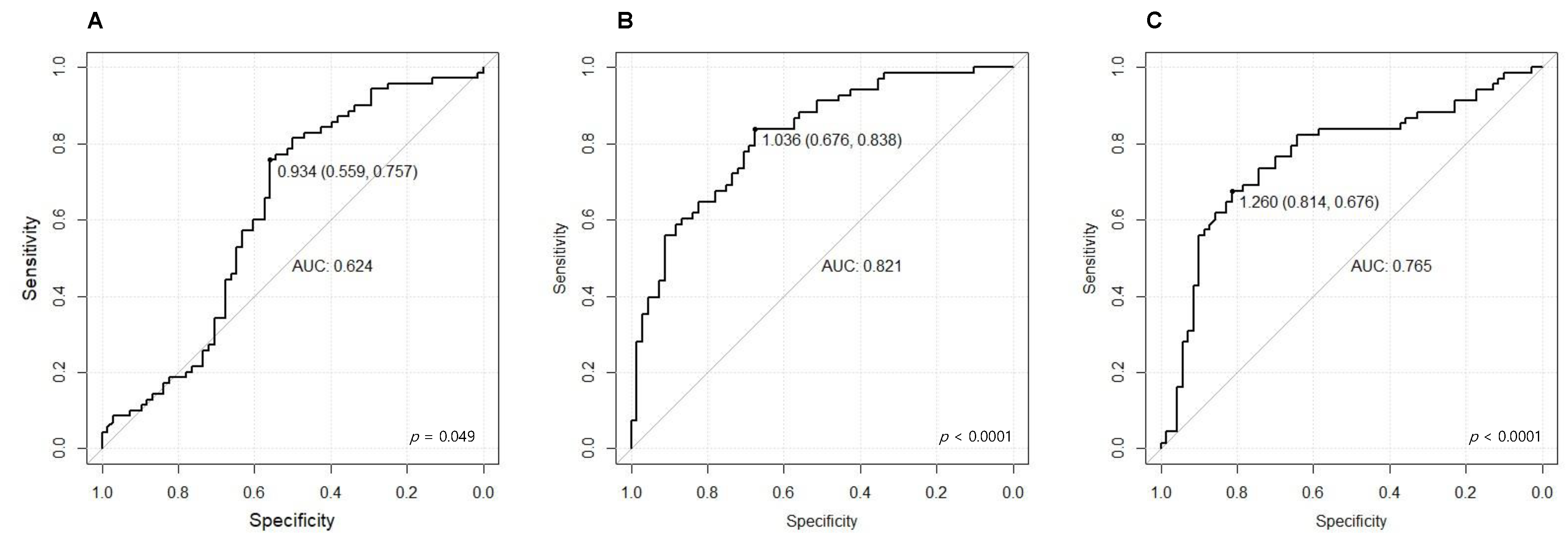
3.4. Diagnostic Performance of AsAGP Level
3.5. Logistic Regression Analyses of Predictors for Detecting CHB with LC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report, 2017. 2017. Available online: https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (accessed on 14 February 2021).
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Weissberg, J.I.; Andres, L.L.; Smith, C.I.; Weick, S.; Nichols, J.E.; Garcia, G.; Robinson, W.S.; Merigan, T.C.; Gregory, P.B. Survival in chronic hepatitis B. An analysis of 379 patients. Ann. Intern. Med. 1984, 101, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Song, K.; Han, K.-H. Transient Elastography is Superior to FIB-4 in Assessing the Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis B. Medicine 2016, 95, e3434. [Google Scholar] [CrossRef] [PubMed]
- Yim, H.J.; Kim, J.H.; Park, J.Y.; Yoon, E.L.; Park, H.; Kwon, J.H.; Sinn, D.H.; Lee, S.H.; Lee, J.-H.; Lee, H.W. Comparison of clinical practice guidelines for the management of chronic hepatitis B: When to start, when to change, and when to stop. Clin. Mol. Hepatol. 2020, 26, 411–429. [Google Scholar] [CrossRef] [PubMed]
- Bataller, R.; Brenner, D.A. Liver fibrosis. J. Clin. Investig. 2005, 115, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Degos, F.; Perez, P.; Roche, B.; Mahmoudi, A.; Asselineau, J.; Voitot, H.; Bedossa, P. Diagnostic accuracy of FibroScan and comparison to liver fibrosis biomarkers in chronic viral hepatitis: A multicenter prospective study (the FIBROSTIC study). J. Hepatol. 2010, 53, 1013–1021. [Google Scholar] [CrossRef]
- Odagiri, N.; Matsubara, T.; Sato-Matsubara, M.; Fujii, H.; Enomoto, M.; Kawada, N. Anti-fibrotic treatments for chronic liver diseases: The present and the future. Clin. Mol. Hepatol. 2021, 27, 413–424. [Google Scholar] [CrossRef]
- Lim, T.S.; Kim, J.K. Is liver biopsy still useful in the era of non-invasive tests? Clin. Mol. Hepatol. 2020, 26, 302–304. [Google Scholar] [CrossRef]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef]
- Castera, L. Noninvasive methods to assess liver disease in patients with hepatitis B or C. Gastroenterology 2012, 142, 1293–1302. [Google Scholar] [CrossRef]
- Afdhal, N.H.; Bacon, B.R.; Patel, K.; Lawitz, E.J.; Gordon, S.C.; Nelson, D.R.; Challies, T.L.; Nasser, I.; Garg, J.; Wei, L.-J.; et al. Accuracy of fibroscan, compared with histology, in analysis of liver fibrosis in patients with hepatitis B or C: A United States multicenter study. Clin. Gastroenterol. Hepatol. 2015, 13, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Khac, E.; Chatelain, D.; Tramier, B.; Decrombecque, C.; Robert, B.; Joly, J.-P.; Brevet, M.; Grignon, P.; Lion, S.; Le Page, L.; et al. Assessment of asymptomatic liver fibrosis in alcoholic patients using fibroscan: Prospective comparison with seven non-invasive laboratory tests. Aliment. Pharmacol. Ther. 2008, 28, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Kim, D.Y.; Park, J.Y.; Ahn, S.H.; Chon, C.Y.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Park, Y.N.; Han, K.-H. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver. Int. 2010, 30, 546–553. [Google Scholar] [CrossRef]
- Xiao, G.; Yang, J.; Yan, L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: A systemic review and meta-analysis. Hepatology 2015, 61, 292–302. [Google Scholar] [CrossRef]
- Kim, W.R.; Berg, T.; Asselah, T.; Flisiak, R.; Fung, S.; Gordon, S.C.; Janssen, H.L.; Lampertico, P.; Lau, D.; Bornstein, J.D.; et al. Evaluation of APRI and FIB-4 scoring systems for non-invasive assessment of hepatic fibrosis in chronic hepatitis B patients. J. Hepatol. 2016, 64, 773–780. [Google Scholar] [CrossRef]
- Hochepied, T.; Berger, F.G.; Baumann, H.; Libert, C. Alpha(1)-acid glycoprotein: An acute phase protein with inflammatory and immunomodulating properties. Cytokine Growth Factor Rev. 2003, 14, 25–34. [Google Scholar] [CrossRef]
- Weigel, P.H. Evidence that the hepatic asialoglycoprotein receptor is internalized during endocytosis and that receptor recycling can be uncoupled from endocytosis at low temperature. Biochem. Biophys. Res. Commun. 1981, 101, 1419–1425. [Google Scholar] [CrossRef]
- Sawamura, T.; Shiozaki, Y. Mechanism and clinical relevance of elevated levels of circulating asialoglycoproteins. Liver Dis. Target. Diagn. Ther. Using Specif. Recept. Ligands 1991, 4, 215–234. [Google Scholar]
- Arima, T. Serum glycoproteins in the liver diseases. VIII. Desialylated glycoproteins in the liver cirrhosis. Gastroenterol. Jpn. 1979, 14, 349–352. [Google Scholar] [CrossRef]
- Song, E.Y.; Kim, K.A.; Kim, Y.D.; Lee, E.Y.; Lee, H.S.; Kim, H.J.; Ahn, B.M.; Choe, Y.K.; Kim, C.H.; Chung, T.W. Elevation of serum asialo-alpha(1) acid glycoprotein concentration in patients with hepatic cirrhosis and hepatocellular carcinoma as measured by antibody-lectin sandwich assay. Hepatol. Res. 2003, 26, 311–317. [Google Scholar] [CrossRef]
- Lim, D.H.; Kim, M.; Jun, D.W.; Kwak, M.J.; Yoon, J.H.; Lee, K.N.; Lee, H.L.; Lee, O.Y.; Yoon, B.C.; Choi, H.S.; et al. Diagnostic Performance of Serum Asialo alpha1-Acid Glycoprotein Levels to Predict Liver Cirrhosis. Gut Liver. 2021, 15, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.U.; Jeon, M.Y.; Lim, T.S. Diagnostic Performance of Serum Asialo-alpha1-acid Glycoprotein for Advanced Liver Fibrosis or Cirrhosis in Patients with Chronic Hepatitis B or Nonalcoholic Fatty Liver Disease. Korean J. Gastroenterol. 2019, 74, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Marcellin, P.; Ziol, M.; Bedossa, P.; Douvin, C.; Poupon, R.; De Lédinghen, V.; Beaugrand, M. Non-invasive assessment of liver fibrosis by stiffness measurement in patients with chronic hepatitis B. Liver Int. 2009, 29, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Lee, E.Y.; Kang, J.H.; Lee, H.G.; Kim, J.W.; Kwon, D.H.; Jang, Y.J.; Yeom, Y.I.; Chung, T.W.; Kim, Y.D.; et al. Diagnostic accuracy of serum asialo-alpha1-acid glycoprotein concentration for the differential diagnosis of liver cirrhosis and hepatocellular carcinoma. Clin. Chim. Acta 2006, 369, 46–51. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- European Association for Study of Liver; Asociacion Latinoamericana para el Estudio del Higado. EASL Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [Green Version]
- Jia, J.; Hou, J.; Ding, H.; Chen, G.; Xie, Q.; Wang, Y.; Zeng, M.; Zhao, J.; Wang, T.; Hu, X.; et al. Transient elastography compared to serum markers to predict liver fibrosis in a cohort of Chinese patients with chronic hepatitis B. J. Gastroenterol. Hepatol. 2015, 30, 756–762. [Google Scholar] [CrossRef]
- Thompson, S.; Matta, K.L.; Turner, G.A. Changes in fucose metabolism associated with heavy drinking and smoking: A preliminary report. Clin. Chim. Acta 1991, 201, 59–64. [Google Scholar] [CrossRef]
- Mann, A.C.; Record, C.O.; Self, C.H.; Turner, G.A. Monosaccharide composition of haptoglobin in liver diseases and alcohol abuse: Large changes in glycosylation associated with alcoholic liver disease. Clin. Chim. Acta 1994, 227, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Hada, T.; Fukui, K.; Iwasaki, A.; Higashino, K.; Yasukawa, K. Enzyme-linked immunosorbent assay (ELISA) for Aleuria aurantia lectin-reactive serum cholinesterase to differentiate liver cirrhosis and chronic hepatitis. Clin. Chim. Acta 1995, 243, 1–9. [Google Scholar] [CrossRef]
- Hada, T.; Kondo, M.; Yasukawa, K.; Amuro, Y.; Higashino, K. Discrimination of liver cirrhosis from chronic hepatitis by measuring the ratio of Aleuria aurantia lectin-reactive serum cholinesterase to immunoreactive protein. Clin. Chim. Acta 1999, 281, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Naitoh, A.; Aoyagi, Y.; Asakura, H. Highly enhanced fucosylation of serum glycoproteins in patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 1999, 14, 436–445. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Saitoh, A.; Suzuki, Y.; Igarashi, K.; Oguro, M.; Yokota, T.; Mori, S.; Suda, T.; Asakura, H.; Isemura, M. Fucosylation index of alpha-fetoprotein, a possible aid in the early recognition of hepatocellular carcinoma in patients with cirrhosis. Hepatology 1993, 17, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Kang, J.H.; Kim, K.A.; Chung, T.W.; Kim, H.J.; Yoon, D.Y.; Lee, H.G.; Kwon, D.H.; Kim, J.W.; Kim, C.H.; et al. Development of a rapid, immunochromatographic strip test for serum asialo alpha1-acid glycoprotein in patients with hepatic disease. J. Immunol. Methods 2006, 308, 116–123. [Google Scholar] [CrossRef]
- Forsgren, M.F.; Nasr, P.; Karlsson, M.; Dahlström, N.; Norén, B.; Ignatova, S.; Sinkus, R.; Cedersund, G.; Leinhard, O.D.; Ekstedt, M.; et al. Biomarkers of liver fibrosis: Prospective comparison of multimodal magnetic resonance, serum algorithms and transient elastography. Scand. J. Gastroenterol. 2020, 55, 848–859. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Flamm, S.L.; Singh, S.; Falck-Ytter, Y.T.; Clinical Guidelines Committee of the American Gastroenterological Association. American Gastroenterological Association Institute Guideline on the Role of Elastography in the Evaluation of Liver Fibrosis. Gastroenterology 2017, 152, 1536–1543. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 206) | Healthy Controls (n = 68) | CHB Patients (n = 70) | CHB Patients with LC (n = 68) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 53.3 ± 11.3 | 50.9 ± 13.4 | 53.7 ± 10.4 | 55.3 ± 9.6 | 0.07 |
| Male gender (number, %) | 100 (48.5) | 18 (26.5) | 43 (61.4) | 39 (57.4) | <0.001 |
| Diabetes (number, %) | 20 (9.7) | 0 (0.0) | 6 (8.6) | 14 (20.6) | <0.001 |
| Hypertension (number, %) | 35 (17.0) | 0 (0.0) | 17 (24.3) | 18 (26.5) | 0.001 |
| AST (IU/L) | 30.1 ± 14.4 | 21.9 ± 6.4 | 29.6 ± 14.2 | 38.8 ± 15.4 | <0.001 |
| ALT (IU/L) | 28.8 ± 18.8 | 18.1 ± 8.3 | 29.8 ± 17.8 | 38.5 ± 21.7 | <0.001 |
| Total bilirubin (mg/dL) | 0.9 ± 1.0 | 0.8 ± 1.5 | 0.9 ± 0.4 | 1.1 ± 0.5 | 0.309 |
| Albumin (g/dL) | 4.2 ± 0.3 | 4.3 ± 0.2 | 4.3 ± 0.2 | 4.1 ± 0.3 | 0.01 |
| Liver stiffness (kPa) | 12.8 ± 8.3 * | NA | 6.9 ± 2.3 | 18.8 ± 7.9 | <0.001 |
| Participants Group | Total (n = 206) | p-Value | |
|---|---|---|---|
| n | AsAGP (μg/mL) | ||
| Healthy controls | 68 | 1.036 ± 0.308 | <0.001 |
| CHB patients | 70 | 1.121 ± 0.337 | |
| CHB patients with LC | 68 | 1.505 ± 0.432 | |
| Fibrosis Stage | Total (n = 206) | p-Value | |
|---|---|---|---|
| n | AsAGP (μg/mL) | ||
| Healthy controls | 68 | 1.036 ± 0.308 | <0.001 |
| F0-1 | 39 | 1.068 ± 0.250 | |
| F2 | 8 | 0.9778 ± 0.144 | |
| F3 | 23 | 1.261 ± 0.458 | |
| F4 (Liver cirrhosis) | 68 | 1.505 ± 0.432 | |
| Variable | AsAGP | Liver Stiffness | ||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| Age (years) | 0.075 | NS | 0.119 | 0.087 |
| AST (IU/L) | 0.227 | 0.001 | 0.436 | <0.001 |
| ALT (IU/L) | 0.160 | 0.021 | 0.404 | <0.001 |
| Total bilirubin (mg/dL) | 0.102 | NS | 0.139 | 0.047 |
| Albumin (g/dL) | −0.112 | NS | −0.153 | 0.029 |
| Liver stiffness (kPa) | 0.436 | <0.001 | - | - |
| AsAGP (μg/mL) | - | - | 0.436 | <0.001 |
| CHB Patients Versus Healthy Controls | CHB Patients with LC Versus Healthy Controls | CHB Patients Versus CHB Patients with LC | |
|---|---|---|---|
| AUC (95% CI) | 0.624 (0.528–0.720) | 0.821 (0.751–0.890) | 0.765 (0.682–0.848) |
| Optimal cut-off (μg/mL) | 0.933 | 1.036 | 1.260 |
| Sensitivity | 75.7% | 83.8% | 81.4% |
| Specificity | 55.9% | 67.6% | 67.5% |
| Variables | Healthy Controls Versus | CHB Patients Versus | ||||
|---|---|---|---|---|---|---|
| CHB Patients with LC | CHB Patients with LC | |||||
| Univariate | Stepwise Logistic Regression | Univariate | Stepwise Logistic Regression | |||
| p-Value | OR | p-Value | p-Value | OR | p-Value | |
| Age | 0.03 | 0.341 | ||||
| Male gender | <0.001 | 0.629 | ||||
| Hypertension | - | 0.77 | ||||
| Diabetes | - | 0.045 | ||||
| AST | <0.001 | <0.001 | ||||
| ALT | <0.001 | 1.17 | <0.001 | 0.011 | ||
| GGT | <0.001 | 0.001 | 1.012 | 0.038 | ||
| Total bilirubin | 0.236 | 0.012 | ||||
| Albumin | 0.013 | 0.043 | 0.047 | 0.019 | ||
| Platelet | <0.001 | 0.97 | <0.001 | <0.001 | 0.984 | <0.001 |
| AsAGP | <0.001 | 54.514 | <0.001 | <0.001 | 11.898 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Bae, S.; Kim, J.H.; Kwak, M.; Jeon, S.Y.; Kim, T.; Yim, S.Y.; Lee, Y.-S.; Jung, Y.K.; Seo, Y.S.; et al. Diagnostic Efficacy of Serum Asialo α1-Acid Glycoprotein Levels for Advanced Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Compared to That in Healthy Subjects: A Prospective Study. J. Clin. Med. 2023, 12, 712. https://doi.org/10.3390/jcm12020712
Lee Y, Bae S, Kim JH, Kwak M, Jeon SY, Kim T, Yim SY, Lee Y-S, Jung YK, Seo YS, et al. Diagnostic Efficacy of Serum Asialo α1-Acid Glycoprotein Levels for Advanced Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Compared to That in Healthy Subjects: A Prospective Study. Journal of Clinical Medicine. 2023; 12(2):712. https://doi.org/10.3390/jcm12020712
Chicago/Turabian StyleLee, Yoonseok, Seryun Bae, Ji Hoon Kim, Minjung Kwak, So Yeon Jeon, Taehyung Kim, Sun Young Yim, Young-Sun Lee, Young Kul Jung, Yeon Seok Seo, and et al. 2023. "Diagnostic Efficacy of Serum Asialo α1-Acid Glycoprotein Levels for Advanced Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Compared to That in Healthy Subjects: A Prospective Study" Journal of Clinical Medicine 12, no. 2: 712. https://doi.org/10.3390/jcm12020712