
A 20-Year Retrospective Study of Children and Adolescents Treated by the Three-in-One Procedure for Patellar Realignment
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Baseline Variables
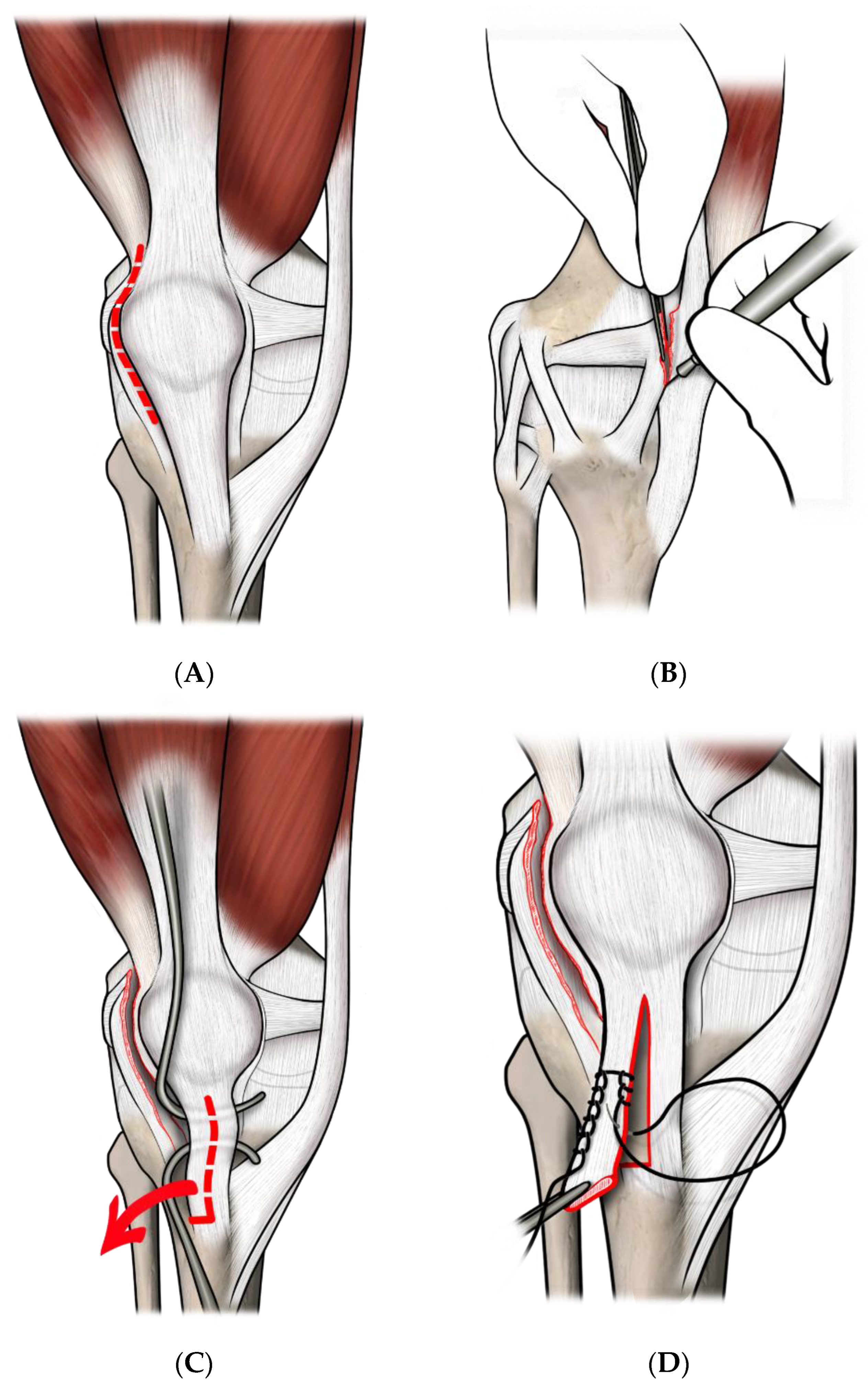
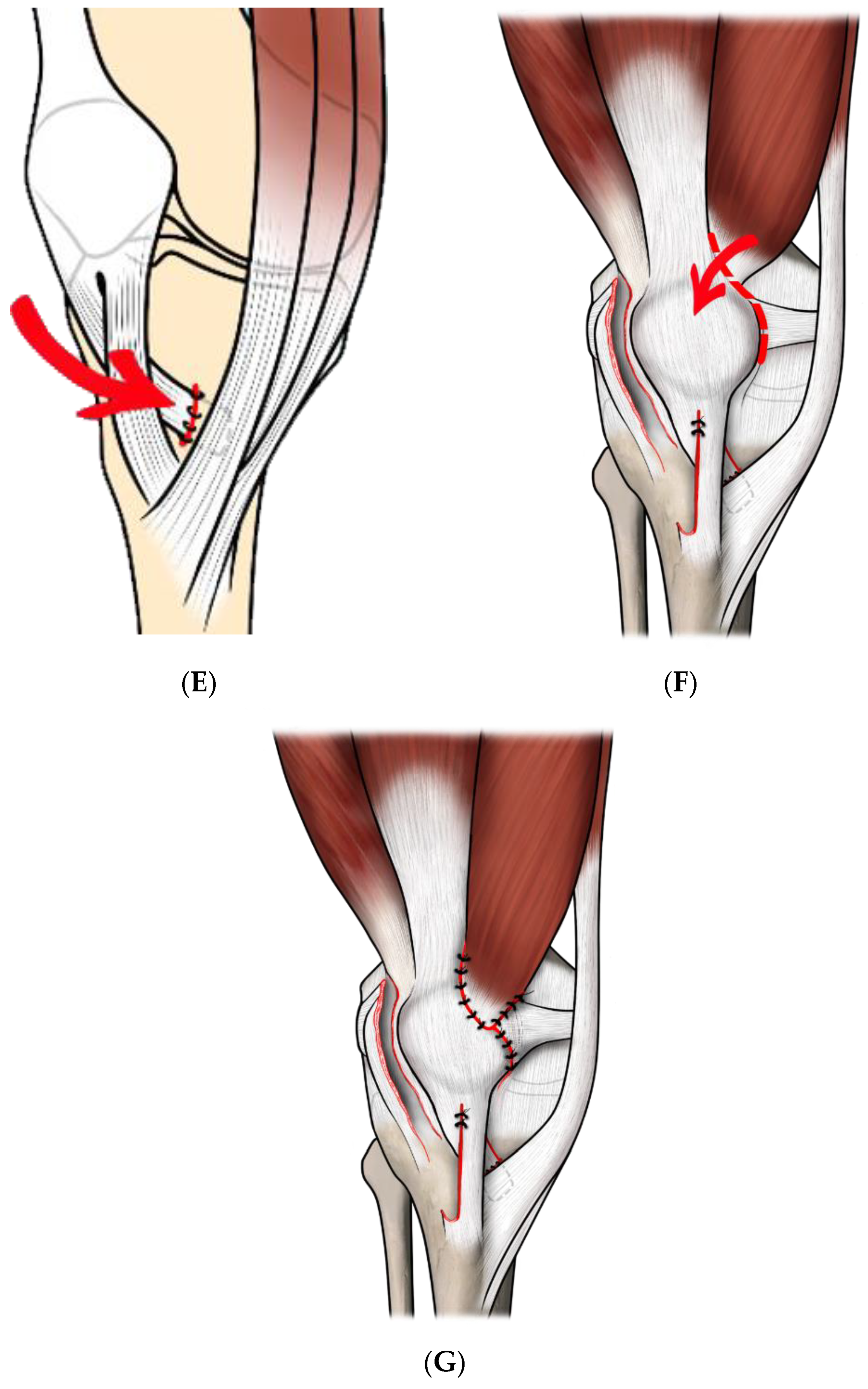
2.3. Surgical Technique
2.4. Post-Operative Management and Follow-Up
2.5. Data Analysis
3. Results
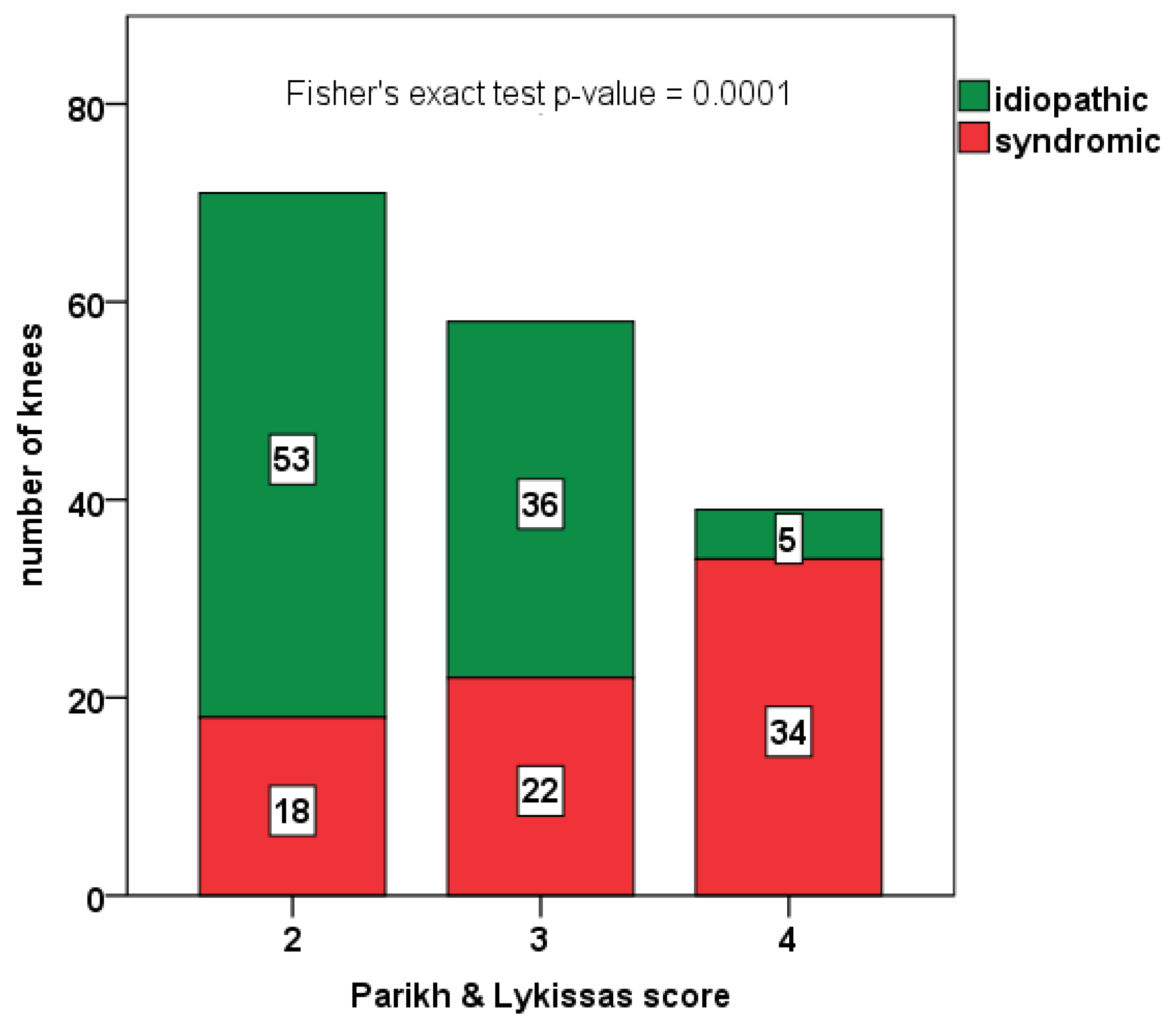
3.1. Demographics and Clinical/Radiographic Parameters at Baseline
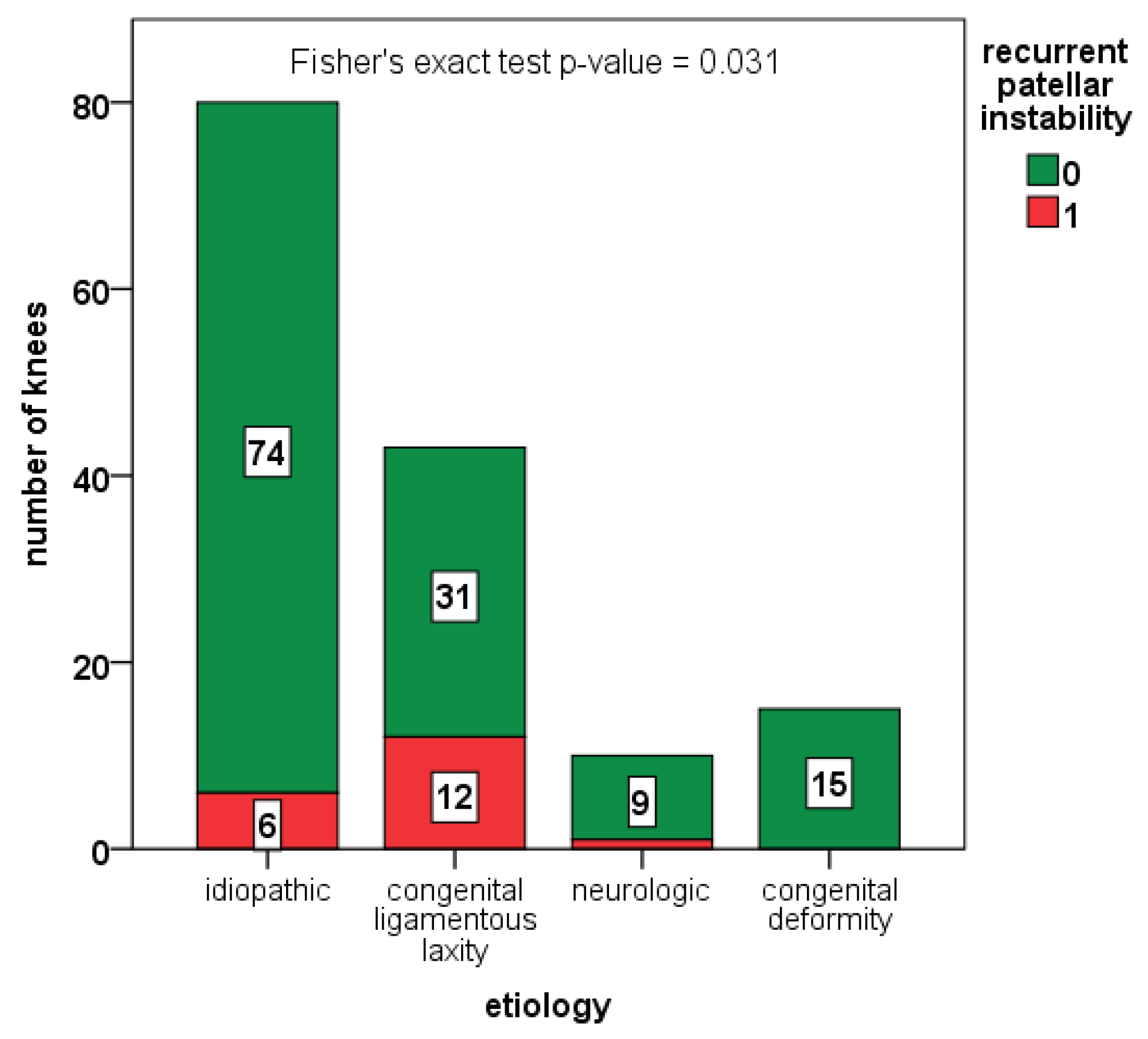
3.2. Complications and Rate of Redislocation
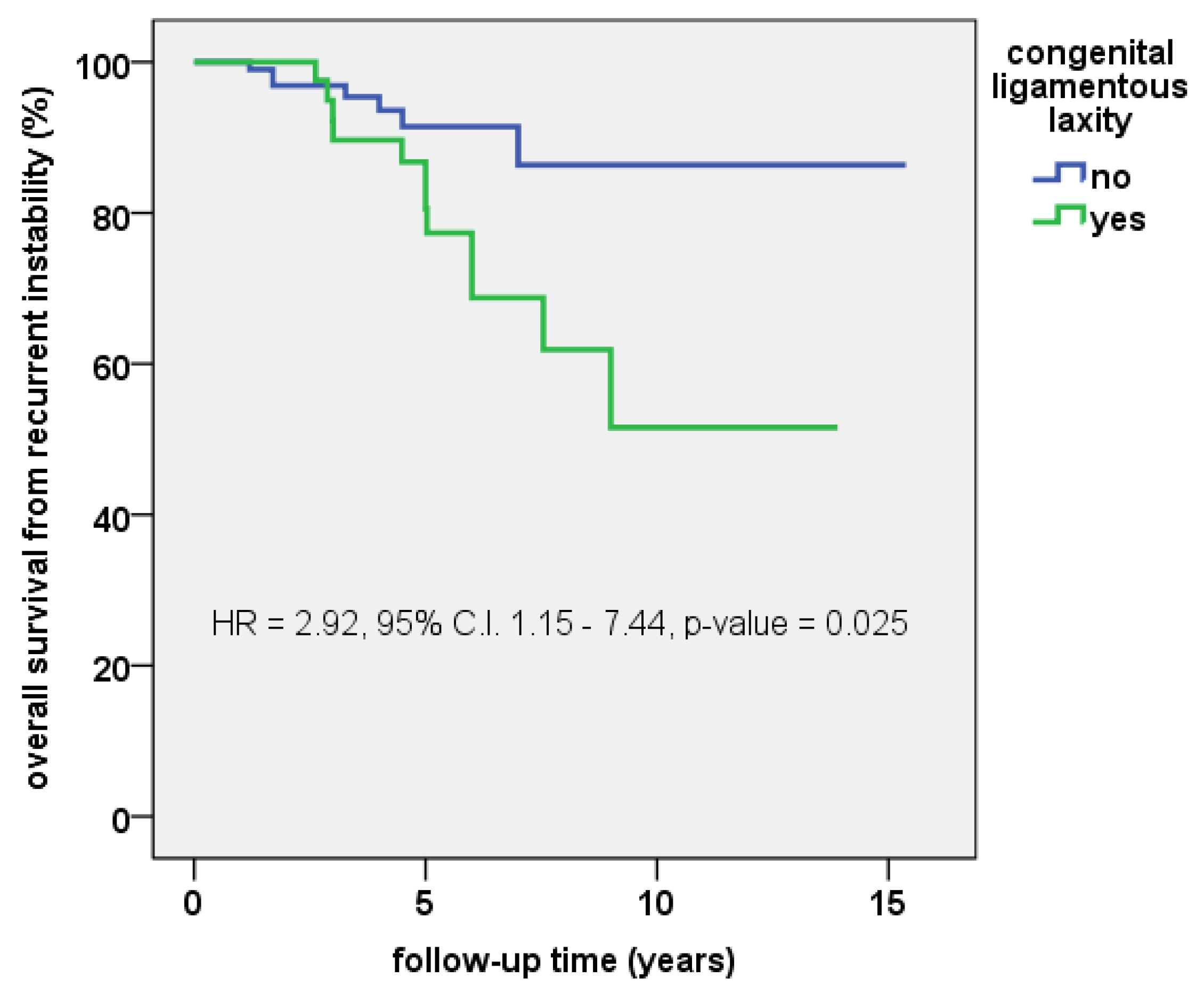
3.3. Survival Free from Redislocation
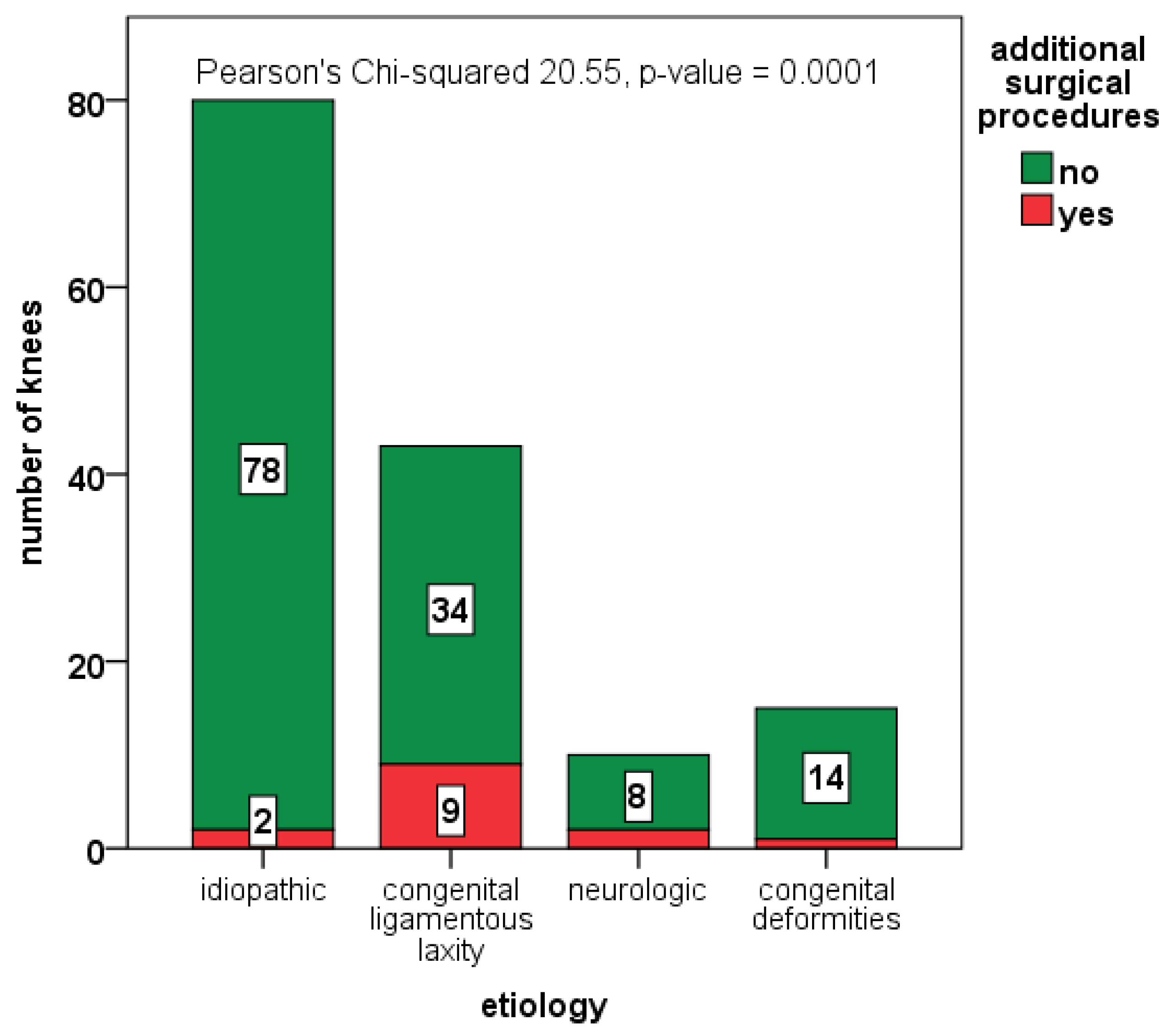
3.4. Additional Surgical Procedures
3.5. Clinical and Functional Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gravesen, K.S.; Kallemose, T.; Blønd, L.; Troelsen, A.; Barfod, K.W. High incidence of acute and recurrent patellar dislocations: A retrospective nationwide epidemiological study involving 24.154 primary dislocations. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.L.; Pareek, A.; Hewett, T.E.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. High rate of recurrent patellar dislocation in skeletally immature patients: A long-term population-based study. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- A Arendt, E.; Fithian, D.C.; Cohen, E. Current concepts of lateral patella dislocation. Clin. Sports Med. 2002, 21, 499–519. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.N.; Lykissas, M.G. Classification of Lateral Patellar Instability in Children and Adolescents. Orthop. Clin. N. Am. 2016, 47, 145–152. [Google Scholar] [CrossRef] [PubMed]
- DeJour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef]
- Schlichte, L.M.; Sidharthan, S.; Green, D.W.; Parikh, S.N. Pediatric Management of Recurrent Patellar Instability. Sports Med. Arthrosc. Rev. 2019, 27, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Dugdale, T.W.; Renshaw, T.S. Instability of the patellofemoral joint in Down syndrome. J. Bone Jt. Surg. 1986, 68, 405–413. [Google Scholar] [CrossRef]
- Chotel, F.; Bérard, J.; Raux, S. Patellar instability in children and adolescents. Orthop. Traumatol. Surg. Res. 2014, 100, S125–S137. [Google Scholar] [CrossRef] [Green Version]
- Hiemstra, L.A.; Kerslake, S.; LaFave, M.; Heard, S.M.; Buchko, G.M.L. Introduction of a classification system for patients with patellofemoral instability (WARPS and STAID). Knee Surg. Sports Traumatol. Arthrosc. 2013, 22, 2776–2782. [Google Scholar] [CrossRef]
- Sillanpää, P.J.; Salonen, E.; Pihlajamäki, H.; Mäenpää, H.M. Medial patellofemoral ligament avulsion injury at the patella: Classification and clinical outcome. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2414–2418. [Google Scholar] [CrossRef]
- Garin, C.; Chaker, M.; Dohin, B.; Kohler, R. Permanent, habitual dislocation and recurrent dislocation of the patella in children: Surgical management by patellar ligamentous transfer in 50 knees. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2007, 93, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Herring, J. Tachdjian’s Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Bitar, A.C.; Demange, M.; D’Elia, C.O.; Camanho, G.L. Traumatic patellar dislocation: Nonoperative treatment compared with MPFL reconstruction using patellar tendon. Am. J. Sports Med. 2011, 40, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Donell, S.; Song, F.; Hing, C. Surgical versus non-surgical interventions for treating patellar dislocation. Cochrane Database Syst. Rev. 2015, 2, CD008106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nwachukwu, B.U.; So, C.; Schairer, W.W.; Green, D.W.; Dodwell, E.R. Surgical versus conservative management of acute patellar dislocation in children and adolescents: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 760–767. [Google Scholar] [CrossRef]
- Pagliazzi, G.; Napoli, F.; Previtali, D.; Filardo, G.; Zaffagnini, S.; Candrian, C. A Meta-analysis of Surgical Versus Nonsurgical Treatment of Primary Patella Dislocation. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 2469–2481. [Google Scholar] [CrossRef] [PubMed]
- Beasley, L.S.; Vidal, A.F. Traumatic patellar dislocation in children and adolescents: Treatment update and literature review. Curr. Opin. Pediatr. 2004, 16, 29–36. [Google Scholar] [CrossRef]
- Pookarnjanamorakot, C.; Jaovisidha, S.; Apiyasawat, P. The patellar tilt angle: Correlation of MRI evaluation with anterior knee pain. J. Med. Assoc. Thail. 1998, 81, 958–963. [Google Scholar]
- Grelsamer, R.P.; Weinstein, C.H.; Gould, J.; Dubey, A. Patellar tilt: The physical examination correlates with MR imaging. Knee 2008, 15, 3–8. [Google Scholar] [CrossRef]
- Diederichs, G.; Issever, A.S.; Scheffler, S. MR Imaging of Patellar Instability: Injury Patterns and Assessment of Risk Factors. Radiographics 2010, 30, 961–981. [Google Scholar] [CrossRef] [Green Version]
- Steensen, R.N.; Bentley, J.C.; Trinh, T.Q.; Backes, J.R.; Wiltfong, R.E. The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: A magnetic resonance imaging study. Am. J. Sports Med. 2015, 43, 921–927. [Google Scholar] [CrossRef]
- Franco, B.A.F.M.; Sadigursky, D.; Daltro, G.D.C. Patellar position in patients with patellofemoral syndrome as characterized by anatomo-radiographic study. Rev. Bras. Ortop. 2018, 53, 410. [Google Scholar] [CrossRef] [PubMed]
- Vairo, G.L.; Moya-Angeler, J.; Siorta, M.A.; Anderson, A.H.; Sherbondy, P. Tibial Tubercle-Trochlear Groove Distance Is a Reliable and Accurate Indicator of Patellofemoral Instability. Clin. Orthop. Relat. Res. 2019, 477, 1450. [Google Scholar] [CrossRef] [PubMed]
- Bettuzzi, C.; Lampasi, M.; Magnani, M.; Donzelli, O. Surgical treatment of patellar dislocation in children with Down syndrome: A 3- to 11-year follow-up study. Knee Surg. Sports Traumatol. Arthrosc. 2008, 17, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Green, W.T. Recurrent dislocation of patella—Its surgical correction in growing child. J. Bone Jt. Surg. Am. Vol. 1965, 8, 1670. [Google Scholar]
- Fondren, F.B.; Goldner, J.L.; Bassett, F.H., 3rd. Recurrent dislocation of the patella treated by the modified Roux-Goldthwait procedure. A prospective study of forty-seven knees. J. Bone Jt. Surg. 1985, 67, 993–1005. [Google Scholar] [CrossRef]
- Kujala, U.M.; Jaakkola, L.H.; Koskinen, S.K.; Taimela, S.; Hurme, M.; Nelimarkka, O. Scoring of patellofemoral disorders. Arthrosc. J. Arthrosc. Relat. Surg. 1993, 9, 159–163. [Google Scholar] [CrossRef]
- Cerciello, S.; Corona, K.; Morris, B.J.; Visonà, E.; Maccauro, G.; Maffulli, N.; Ronga, M. Cross-cultural adaptation and validation of the Italian versions of the Kujala, Larsen, Lysholm and Fulkerson scores in patients with patellofemoral disorders. J. Orthop. Traumatol. 2018, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- Sillanpää, P.J.; Mäenpää, H.M.; Mattila, V.M.; Visuri, T.; Pihlajamäki, H. Arthroscopic surgery for primary traumatic patellar dislocation: A prospective, nonrandomized study comparing patients treated with and without acute arthroscopic stabilization with a median 7-year follow-up. Am. J. Sports Med. 2008, 36, 2301–2309. [Google Scholar] [CrossRef]
- Vavken, P.; Wimmer, M.D.; Camathias, C.; Quidde, J.; Valderrabano, V.; Pagenstert, G. Treating Patella Instability in Skeletally Immature Patients. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1410–1422. [Google Scholar] [CrossRef]
- Zhang, K.; Jiang, H.; Li, J.; Fu, W. Comparison Between Surgical and Nonsurgical Treatment for Primary Patellar Dislocations in Adolescents: A Systematic Review and Meta-analysis of Comparative Studies. Orthop. J. Sports Med. 2020, 8, 2325967120946446. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Ciuffreda, M.; Loppini, M.; Baldari, A.; Maffulli, N.; Denaro, V. Elmslie-Trillat, Maquet, Fulkerson, Roux Goldthwait, and Other Distal Realignment Procedures for the Management of Patellar Dislocation: Systematic Review and Quantitative Synthesis of the Literature. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 929–943. [Google Scholar] [CrossRef] [PubMed]
- Murray, I.R.; LaPrade, C.M.; Pullen, W.M.; Sherman, S.L. Medial Patellofemoral Ligament Repair or Medial Advancement: Is There a Role? Clin. Sports Med. 2022, 41, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Wilkens, O.E.; Hannink, G.; van de Groes, S.A.W. Recurrent patellofemoral instability rates after MPFL reconstruction techniques are in the range of instability rates after other soft tissue realignment techniques. Knee Surg. Sports Traumatol. Arthrosc. 2019, 28, 1919–1931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, S.Y.; Park, K.B.; Kim, B.R.; Park, H.W.; Kim, H.W. The ‘four-in-one’ procedure for habitual dislocation of the patella in children: Early results in patients with severe generalised ligamentous laxity and aplasis of the trochlear groove. J. Bone Jt. Surg. 2007, 89, 1645–1649. [Google Scholar] [CrossRef]
- Ruzzini, L.; Donati, F.; Russo, R.; Costici, P.F. Modified Roux-Goldthwait Procedure for Management of Patellar Dislocation in Skeletally Immature Patients with Down Syndrome. Indian J. Orthop. 2019, 53, 122–127. [Google Scholar] [CrossRef]
- Camathias, C.; Rutz, E.; Götze, M.; Brunner, R.; Vavken, P.; Gaston, M.S. Poor outcome at 7.5 years after Stanisavljevic quadriceps transposition for patello-femoral instability. Arch. Orthop. Trauma Surg. 2014, 134, 473–478. [Google Scholar] [CrossRef]
- Sever, R.; Fishkin, M.; Hemo, Y.; Wientroub, S.; Yaniv, M. Surgical Treatment of Congenital and Obligatory Dislocation of the Patella in Children. J. Pediatr. Orthop. 2019, 39, 436–440. [Google Scholar] [CrossRef]
- Imerci, A.; McDonald, T.C.; Rogers, K.J.; Thacker, M.M.; Atanda, A. Outcomes of medial patellofemoral ligament reconstruction and tibial tubercle osteotomy in syndromic adolescents with patellar dislocation. J. Clin. Orthop. Trauma 2022, 25, 101770. [Google Scholar] [CrossRef]
- Hire, J.M.; Parikh, S.N. 4-in-1 Quadricepsplasty for Fixed and Habitual Dislocation of Patella. Arthrosc. Tech. 2022, 11, e537–e544. [Google Scholar] [CrossRef]
- Ramos, O.; Burke, C.; Lewis, M.; Morrison, M.J.; Paley, D.; Nelson, S.C. Modified Langenskiöld procedure for chronic, recurrent, and congenital patellar dislocation. J. Child. Orthop. 2020, 14, 318–329. [Google Scholar] [CrossRef]
- Mo, Y.; Jing, Y.; Wang, D.; Paley, D.; Ning, B. Modified Langenskiöld procedure for congenital patella dislocations in pediatric patients. BMC Musculoskelet. Disord. 2022, 23, 241. [Google Scholar] [CrossRef] [PubMed]
- Marumo, K.; Fujii, K.; Tanaka, T.; Takeuchi, H.; Saito, H.; Koyano, Y. Surgical management of congenital permanent dislocation of the patella in nail patella syndrome by Stanisavljevic procedure. J. Orthop. Sci. 1999, 4, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Myers, P.; Williams, A.; Dodds, R.; Bülow, J. The three-in-one proximal and distal soft tissue patellar realignment procedure. Results, and its place in the management of patellofemoral instability. Am. J. Sports Med. 1999, 27, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Oliva, F.; Ronga, M.; Longo, U.G.; Testa, V.; Capasso, G.; Maffulli, N. The 3-in-1 Procedure for Recurrent Dislocation of the Patella in Skeletally Immature Children and Adolescents. Am. J. Sports Med. 2009, 37, 1814–1820. [Google Scholar] [CrossRef]
- Malecki, K.; Fabis, J.; Flont, P.; Lipczyk, Z.; Niedzielski, K. Preliminary results of two surgical techniques in the treatment of recurrent patellar dislocation: Medial patellofemoral ligament reconstruction versus combined technique of vastus medialis advancement, capsular plasty and Roux-Goldthwait procedure in treatment of recurrent patellar dislocation. Int. Orthop. 2016, 40, 1869–1874. [Google Scholar] [CrossRef]
- Frizziero, L.; Santi, G.; Liverani, A.; Napolitano, F.; Papaleo, P.; Maredi, E.; Gennaro, G.; Zarantonello, P.; Stallone, S.; Stilli, S.; et al. Computer-Aided Surgical Simulation for Correcting Complex Limb Deformities in Children. Appl. Sci. 2020, 10, 5181. [Google Scholar] [CrossRef]
- Frizziero, L.; Trisolino, G.; Santi, G.M.; Alessandri, G.; Agazzani, S.; Liverani, A.; Menozzi, G.C.; Di Gennaro, G.L.; Farella, G.M.G.; Abbruzzese, A.; et al. Computer-Aided Surgical Simulation through Digital Dynamic 3D Skeletal Segments for Correcting Torsional Deformities of the Lower Limbs in Children with Cerebral Palsy. Appl. Sci. 2022, 12, 7918. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parikh and Lykissas Classification Type/Subtype | Description |
|---|---|
| Type 1 | First patellar dislocation |
| A | With osteochondral fracture |
| B | Without osteochondral fracture |
| Type 2 | Recurrent patellar instability |
| A | Recurrent patellar subluxation |
| B | Recurrent (>2) patellar dislocation |
| Type 3 | Dislocatable patella |
| A | Passive patellar dislocation |
| B | Habitual patellar dislocation in flexion or extension |
| Type 4 | Dislocated patella |
| A | Reducible |
| B | Irreducible |
| Baseline Variable | Measurement | Value |
|---|---|---|
| Patients/Knees | Number (male/females) | 126/168 (46/80) |
| Age at treatment (years) | Mean ± SD (range) | 11.5 ± 3.7 (4.1–17.6) |
| BMI (kg/m2) | Mean ± SD (range) | 20.2 ± 4.3 (11.2–38.1) |
| BMI (percentile) | Median (IQR) | 74.5 (37.0–93.0) |
| Caton–Deschamps ratio | Mean ± SD (range) | 1.4 ± 0.4 (0.6–2.6) |
| Congruence angle (°) | Mean ± SD (range) | 39.1 ± 32.5 (2.6–128.4) |
| Patellar tilt (°) | Mean ± SD (range) | 26.1 ± 25.5 (0–127.3) |
| Sulcus angle (°) | Mean ± SD (range) | 149.0 ± 15.8 (111–180) |
| TT-TG distance (mm) | Mean ± SD (range) | 14.1 ± 8.1 (5–20.6) |
| HKA angle | Mean ± SD (range) | 7.6 ± 8.5 (−10.4 varus–+41.0 valgus) |
| Baseline Variable | Group | N | Mean ± SD | p-Value |
|---|---|---|---|---|
| Age at treatment (years) | Idiopathic | 94 | 12.6 ± 3.5 | 0.0001 * |
| Syndromic | 74 | 10.2 ± 3.6 | ||
| BMI | Idiopathic | 91 | 21.1 ± 4.4 | 0.002 * |
| Syndromic | 67 | 19.0 ± 4.0 | ||
| Caton–Deschamps ratio | Idiopathic | 47 | 1.4 ± 0.6 | 0.649 |
| Syndromic | 40 | 1.4 ± 0.4 | ||
| Congruence angle (°) | Idiopathic | 46 | 34.89 ± 29.9 | 0.172 |
| Syndromic | 34 | 44.9 ± 35.4 | ||
| Patellar tilt (°) | Idiopathic | 45 | 18.4 ± 11.7 | 0.001 * |
| Syndromic | 33 | 36.6 ± 34..3 | ||
| Sulcus angle (°) | Idiopathic | 47 | 148.7 ± 14.3 | 0.848 |
| Syndromic | 34 | 149.4 ± 17.9 | ||
| TT-TG distance (mm) | Idiopathic | 20 | 12.4 ± 5.5 | 0.884 |
| Syndromic | 13 | 12.7 ± 6.5 | ||
| HKA angle (°) | Idiopathic | 33 | 7.5 ± 7.0 | 0.943 |
| Syndromic | 36 | 7.7 ± 9.8 |
| Post-Operative Variable | Group | N | Mean ± SD | p-Value |
|---|---|---|---|---|
| Follow-up time (years) | Idiopathic | 79 | 4.2 ± 2.6 | 0.0001 * |
| Syndromic | 68 | 6.5 ± 3.3 | ||
| Kujala AKPS score | Idiopathic | 74 | 90.5 ± 13.1 | 0.001 * |
| Syndromic | 62 | 81.4 ± 18.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trisolino, G.; Depaoli, A.; Gallone, G.; Ramella, M.; Olivotto, E.; Zarantonello, P.; Stallone, S.; Persiani, V.; Casadei, G.; Rocca, G. A 20-Year Retrospective Study of Children and Adolescents Treated by the Three-in-One Procedure for Patellar Realignment. J. Clin. Med. 2023, 12, 702. https://doi.org/10.3390/jcm12020702
Trisolino G, Depaoli A, Gallone G, Ramella M, Olivotto E, Zarantonello P, Stallone S, Persiani V, Casadei G, Rocca G. A 20-Year Retrospective Study of Children and Adolescents Treated by the Three-in-One Procedure for Patellar Realignment. Journal of Clinical Medicine. 2023; 12(2):702. https://doi.org/10.3390/jcm12020702
Chicago/Turabian StyleTrisolino, Giovanni, Alessandro Depaoli, Giovanni Gallone, Marco Ramella, Eleonora Olivotto, Paola Zarantonello, Stefano Stallone, Valentina Persiani, Giacomo Casadei, and Gino Rocca. 2023. "A 20-Year Retrospective Study of Children and Adolescents Treated by the Three-in-One Procedure for Patellar Realignment" Journal of Clinical Medicine 12, no. 2: 702. https://doi.org/10.3390/jcm12020702