
Association between Experimental Pain Measurements and the Central Sensitization Inventory in Patients at Least 3 Months after COVID-19 Infection: A Cross-Sectional Pilot Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Protocol
2.3. Self-Reported Questionnaires
2.4. Experimental Pain Measurements
2.5. Statistical Analysis
3. Results
3.1. Demographic Statistics
3.2. Symptoms of Central Sensitization, Functionality, and Disability
3.3. Experimental Pain Measurements
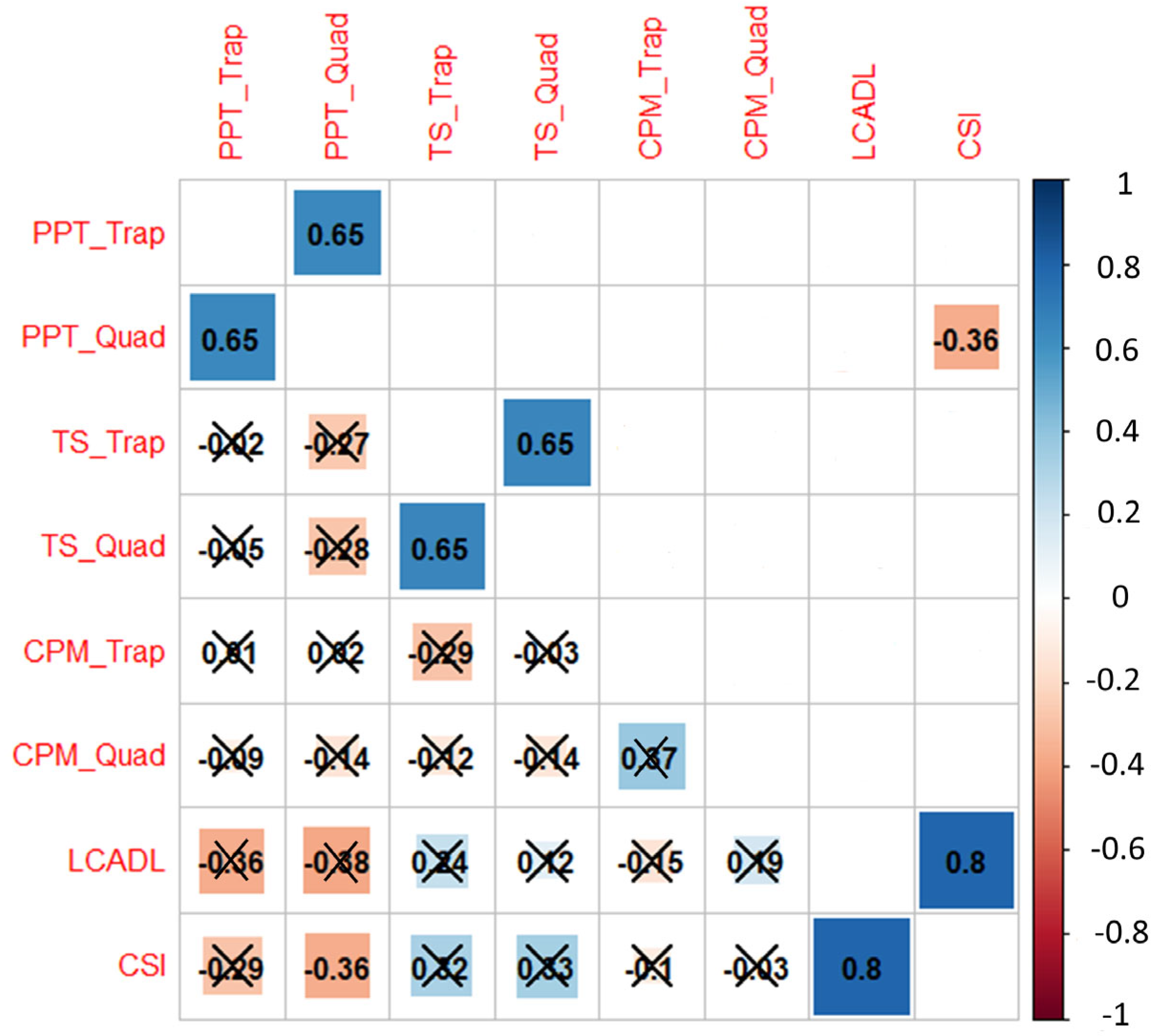
3.4. Associations between Self-Reported and Experimental Measurements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, D.Y.; Shinde, S.K.; Lone, S.; Palem, R.R.; Ghodake, G.S. COVID-19 Pandemic: Public Health Risk Assessment and Risk Mitigation Strategies. J. Pers. Med. 2021, 11, 1243. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Saikia, D.; Bankar, M.; Saurabh, M.K.; Singh, H.; Varikasuvu, S.R.; Maharshi, V. Efficacy of COVID-19 vaccines: A systematic review and network meta-analysis of phase 3 randomized controlled trials. Pharmacol. Rep. 2022, 10, 321. [Google Scholar] [CrossRef] [PubMed]
- VIPER Group COVID19 Vaccine Tracker Team. COVID19 Vaccine Tracker. Available online: https://covid19.trackvaccines.org/ (accessed on 10 November 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Del Valle, N.C.A.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. Long-COVID in children and adolescents: A systematic review and meta-analyses. Sci. Rep. 2022, 12, 9950. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months after COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Carfi, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Moens, M.; Duarte, R.V.; De Smedt, A.; Putman, K.; Callens, J.; Billot, M.; Roulaud, M.; Rigoard, P.; Goudman, L. Health-related quality of life in persons post-COVID-19 infection in comparison to normative controls and chronic pain patients. Front. Public Health 2022, 10, 991572. [Google Scholar] [CrossRef]
- Salari, N.; Khodayari, Y.; Hosseinian-Far, A.; Zarei, H.; Rasoulpoor, S.; Akbari, H.; Mohammadi, M. Global prevalence of chronic fatigue syndrome among long COVID-19 patients: A systematic review and meta-analysis. BioPsychoSoc. Med. 2022, 16, 21. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19): Post COVID-19 Condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition?gclid=Cj0KCQiA37KbBhDgARIsAIzce14fsUS4hL4RdKOXZ6qNRx_LD6BH9EvsFQq2MFLBNx7MFF1HLGhCAkUaAgPBEALw_wcB (accessed on 10 November 2022).
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Aaron, L.A.; Buchwald, D. A review of the evidence for overlap among unexplained clinical conditions. Ann. Intern. Med. 2001, 134, 868–881. [Google Scholar] [CrossRef]
- Yunus, M.B. Editorial review: An update on central sensitivity syndromes and the issues of nosology and psychobiology. Curr. Rheumatol. Rev. 2015, 11, 70–85. [Google Scholar] [CrossRef]
- Bierle, D.M.; Aakre, C.A.; Grach, S.L.; Salonen, B.R.; Croghan, I.T.; Hurt, R.T.; Ganesh, R. Central Sensitization Phenotypes in Post Acute Sequelae of SARS-CoV-2 Infection (PASC): Defining the Post COVID Syndrome. J. Prim. Care Community Health 2021, 12, 21501327211030826. [Google Scholar] [CrossRef] [PubMed]
- Sukocheva, O.A.; Maksoud, R.; Beeraka, N.M.; Madhunapantula, S.V.; Sinelnikov, M.; Nikolenko, V.N.; Neganova, M.E.; Klochkov, S.G.; Kamal, M.A.; Staines, D.R.; et al. Analysis of post COVID-19 condition and its overlap with myalgic encephalomyelitis/chronic fatigue syndrome. J. Adv. Res. 2022, 40, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L.; Bateman, L. Will COVID-19 Lead to Myalgic Encephalomyelitis/Chronic Fatigue Syndrome? Front. Med. 2020, 7, 606824. [Google Scholar] [CrossRef]
- Bourke, J.H.; Wodehouse, T.; Clark, L.V.; Constantinou, E.; Kidd, B.L.; Langford, R.; Mehta, V.; White, P.D. Central sensitisation in chronic fatigue syndrome and fibromyalgia; a case control study. J. Psychosom. Res. 2021, 150, 110624. [Google Scholar] [CrossRef] [PubMed]
- Goudman, L.; De Smedt, A.; Noppen, M.; Moens, M. Is Central Sensitisation the Missing Link of Persisting Symptoms after COVID-19 Infection? J. Clin. Med. 2021, 10, 5594. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Parás-Bravo, P.; Ferrer-Pargada, D.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Nijs, J.; Arendt-Nielsen, L.; Herrero-Montes, M. Sensitization symptoms are associated with psychological and cognitive variables in COVID-19 survivors exhibiting post-COVID pain. Pain Pract. 2022, 23, 23–31. [Google Scholar] [CrossRef]
- Nijs, J.; Huysmans, E. Clinimetrics: The Central Sensitisation Inventory: A useful screening tool for clinicians, but not the gold standard. J. Physiother. 2022, 68, 207. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D. The role of quantitative sensory testing in the prediction of chronic pain. Pain 2019, 160 (Suppl. S1), S66–S69. [Google Scholar] [CrossRef]
- Curatolo, M.; Arendt-Nielsen, L.; Petersen-Felix, S. Central hypersensitivity in chronic pain: Mechanisms and clinical implications. Phys. Med. Rehabil. Clin. N. Am. 2006, 17, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Weaver, K.R.; Griffioen, M.A.; Klinedinst, N.J.; Galik, E.; Duarte, A.C.; Colloca, L.; Resnick, B.; Dorsey, S.G.; Renn, C.L. Quantitative Sensory Testing across Chronic Pain Conditions and Use in Special Populations. Front. Pain Res. 2021, 2, 779068. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain Off. J. Am. Pain Soc. 2013, 14, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Vargas, A.I.; Neblett, R.; Nijs, J.; Chiarotto, A.; Kregel, J.; van Wilgen, C.P.; Pitance, L.; Knezevic, A.; Gatchel, R.J.; Mayer, T.G.; et al. Establishing Central Sensitization-Related Symptom Severity Subgroups: A Multicountry Study Using the Central Sensitization Inventory. Pain Med. 2020, 21, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Kregel, J.; Vuijk, P.J.; Descheemaeker, F.; Keizer, D.; van der Noord, R.; Nijs, J.; Cagnie, B.; Meeus, M.; van Wilgen, P. The Dutch Central Sensitization Inventory (CSI): Factor Analysis, Discriminative Power, and Test-Retest Reliability. Clin. J. Pain 2016, 32, 624–630. [Google Scholar] [CrossRef]
- Pitance, L.; Piraux, E.; Lannoy, B.; Meeus, M.; Berquin, A.; Eeckhout, C.; Dethier, V.; Robertson, J.; Roussel, N. Cross cultural adaptation, reliability and validity of the French version of the central sensitization inventory. Man. Ther. 2016, 25, e83–e84. [Google Scholar] [CrossRef]
- Corsi, G.; Nava, S.; Barco, S. A novel tool to monitor the individual functional status after COVID-19: The Post-COVID-19 Functional Status (PCFS) scale. G. Ital. Cardiol. 2020, 21, 757. [Google Scholar] [CrossRef]
- Klok, F.A.; Boon, G.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Muller, J.P.; Goncalves, P.A.; Fontoura, F.F.; Mattiello, R.; Florian, J. Applicability of the London Chest Activity of Daily Living scale in patients on the waiting list for lung transplantation. J. Bras. Pneumol. 2013, 39, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Garrod, R.; Bestall, J.C.; Paul, E.A.; Wedzicha, J.A.; Jones, P.W. Development and validation of a standardized measure of activity of daily living in patients with severe COPD: The London Chest Activity of Daily Living scale (LCADL). Respir. Med. 2000, 94, 589–596. [Google Scholar] [CrossRef]
- Coppieters, I.; Ickmans, K.; Cagnie, B.; Nijs, J.; De Pauw, R.; Noten, S.; Meeus, M. Cognitive Performance Is Related to Central Sensitization and Health-related Quality of Life in Patients with Chronic Whiplash-Associated Disorders and Fibromyalgia. Pain Physician 2015, 18, E389–E401. [Google Scholar] [PubMed]
- Mertens, M.G.; Hermans, L.; Crombez, G.; Goudman, L.; Calders, P.; Van Oosterwijck, J.; Meeus, M. Comparison of five conditioned pain modulation paradigms and influencing personal factors in healthy adults. Eur. J. Pain 2021, 25, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Ekholm, J.; Hansson, P. Pressure pain thresholds in different tissues in one body region. The influence of skin sensitivity in pressure algometry. Scand. J. Rehabil. Med. 1999, 31, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Pas, R.; Brouns, R.; De Win, J.; Hatem, S.M.; Meeus, M.; Ickmans, K.; van Hooff, R.J.; Nijs, J. Cerebral Blood Flow and Heart Rate Variability in Chronic Fatigue Syndrome: A Randomized Cross-Over Study. Pain Physician 2018, 21, E13–E24. [Google Scholar] [CrossRef]
- Cathcart, S.; Winefield, A.H.; Rolan, P.; Lushington, K. Reliability of temporal summation and diffuse noxious inhibitory control. Pain Res. Manag. 2009, 14, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Moont, R.; Pud, D.; Sprecher, E.; Sharvit, G.; Yarnitsky, D. ‘Pain inhibits pain’ mechanisms: Is pain modulation simply due to distraction? Pain 2010, 150, 113–120. [Google Scholar] [CrossRef]
- Yarnitsky, D.; Bouhassira, D.; Drewes, A.M.; Fillingim, R.B.; Granot, M.; Hansson, P.; Landau, R.; Marchand, S.; Matre, D.; Nilsen, K.B.; et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur. J. Pain 2015, 19, 805–806. [Google Scholar] [CrossRef]
- Staud, R.; Craggs, J.G.; Robinson, M.E.; Perlstein, W.M.; Price, D.D. Brain activity related to temporal summation of C-fiber evoked pain. Pain 2007, 129, 130–142. [Google Scholar] [CrossRef] [Green Version]
- Coppieters, I.; De Pauw, R.; Kregel, J.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M. Differences Between Women with Traumatic and Idiopathic Chronic Neck Pain and Women without Neck Pain: Interrelationships among Disability, Cognitive Deficits, and Central Sensitization. Phys. Ther. 2017, 97, 338–353. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C. The kappa statistic in reliability studies: Use, interpretation, and sample size requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef]
- Uddin, Z.; MacDermid, J.C. Quantitative Sensory Testing in Chronic Musculoskeletal Pain. Pain Med. 2016, 17, 1694–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppieters, I.; Cagnie, B.; Nijs, J.; van Oosterwijck, J.; Danneels, L.; De Pauw, R.; Meeus, M. Effects of Stress and Relaxation on Central Pain Modulation in Chronic Whiplash and Fibromyalgia Patients Compared to Healthy Controls. Pain Physician 2016, 19, 119–130. [Google Scholar] [PubMed]
- Meeus, M.; Van Oosterwijck, J.; Ickmans, K.; Baert, I.; Coppieters, I.; Roussel, N.; Struyf, F.; Pattyn, N.; Nijs, J. Interrelationships between pain processing, cortisol and cognitive performance in chronic whiplash-associated disorders. Clin. Rheumatol. 2015, 34, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Kregel, J.; Schumacher, C.; Dolphens, M.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M.; Coppieters, I. Convergent Validity of the Dutch Central Sensitization Inventory: Associations with Psychophysical Pain Measures, Quality of Life, Disability, and Pain Cognitions in Patients with Chronic Spinal Pain. Pain Pract. 2018, 18, 777–787. [Google Scholar] [CrossRef]
- Gervais-Hupé, J.; Pollice, J.; Sadi, J.; Carlesso, L.C. Validity of the central sensitization inventory with measures of sensitization in people with knee osteoarthritis. Clin. Rheumatol. 2018, 37, 3125–3132. [Google Scholar] [CrossRef]
- Coronado, R.A.; George, S.Z. The Central Sensitization Inventory and Pain Sensitivity Questionnaire: An exploration of construct validity and associations with widespread pain sensitivity among individuals with shoulder pain. Musculoskelet. Sci. Pract. 2018, 36, 61–67. [Google Scholar] [CrossRef]
- Hendriks, E.; Voogt, L.; Lenoir, D.; Coppieters, I.; Ickmans, K. Convergent Validity of the Central Sensitization Inventory in Chronic Whiplash-Associated Disorders; Associations with Quantitative Sensory Testing, Pain Intensity, Fatigue, and Psychosocial Factors. Pain Med. 2020, 21, 3401–3412. [Google Scholar] [CrossRef]
- Kosińska, B.; Tarnacka, B.; Turczyn, P.; Gromadzka, G.; Malec-Milewska, M.; Janikowska-Hołowenko, D.; Neblett, R. Psychometric validation of the Polish version of the Central Sensitization Inventory in subjects with chronic spinal pain. BMC Neurol. 2021, 21, 483. [Google Scholar] [CrossRef]
- Akeda, K.; Yamada, J.; Takegami, N.; Fujiwara, T.; Murata, K.; Kono, T.; Sudo, T.; Imanishi, T.; Asanuma, Y.; Kurata, T.; et al. Evaluation of Central Sensitization Inventory in Patients Undergoing Elective Spine Surgery in a Multicenter Study. Glob. Spine J. 2021, 21925682211047473. [Google Scholar] [CrossRef]
- Holm, L.A.; Nim, C.G.; Lauridsen, H.H.; Filtenborg, J.B.; O’Neill, S.F. Convergent validity of the central sensitization inventory and experimental testing of pain sensitivity. Scand. J. Pain 2022, 22, 597–613. [Google Scholar] [CrossRef]
- Çalik Kütükcü, E.; Çakmak, A.; Kinaci, E.; Uyaroğlu, O.A.; Yağli, N.V.; Güven, G.S.; Sağlam, M.; Özişik, L.; Başaran, N.Ç.; Ince, D.I. Reliability and validity of the Turkish version of Post-COVID-19 Functional Status Scale. Turk. J. Med. Sci. 2021, 51, 2304–2310. [Google Scholar] [CrossRef]
- Ganesh, R.; Grach, S.L.; Ghosh, A.K.; Bierle, D.M.; Salonen, B.R.; Collins, N.M.; Joshi, A.Y.; Boeder, N.D., Jr.; Anstine, C.V.; Mueller, M.R.; et al. The Female-Predominant Persistent Immune Dysregulation of the Post-COVID Syndrome. Mayo Clin. Proc. 2022, 97, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.A.; Rice, A.S.C.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Nijs, J.; Neblett, R.; Polli, A.; Moens, M.; Goudman, L.; Patil, M.S.; Knaggs, R.D.; Pickering, G.; Arendt-Nielsen, L. Phenotyping Post-COVID Pain as a Nociceptive, Neuropathic, or Nociplastic Pain Condition. Biomedicines 2022, 10, 2562. [Google Scholar] [CrossRef] [PubMed]
- Moens, M.; Jansen, J.; De Smedt, A.; Roulaud, M.; Billot, M.; Laton, J.; Rigoard, P.; Goudman, L. Acceptance and Commitment Therapy to Increase Resilience in Chronic Pain Patients: A Clinical Guideline. Medicina 2022, 58, 499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Physician PCFS Score | |||||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | ||
| Patient PCFS score | 0 | 2 | 1 | 0 | 0 | 0 | 0 |
| 1 | 0 | 4 | 2 | 1 | 0 | 0 | |
| 2 | 0 | 1 | 7 | 7 | 0 | 0 | |
| 3 | 0 | 0 | 5 | 9 | 0 | 0 | |
| 4 | 0 | 0 | 0 | 1 | 1 | 0 | |
| 5 | 0 | 0 | 0 | 0 | 0 | 0 |
| Variable | Level | Total Sample (n = 42) | CSI Score < 40/100 (n = 15) | CSI Score ≥ 40/100 (n = 27) |
|---|---|---|---|---|
| Sex | Male/Female | 28.6%/71.4% | 46.7%/53.3% | 18.5%/81.5% |
| Age (years) | 48 (SD: 12) | 49 (SD: 15) | 48 (SD: 11) | |
| Time since COVID-19 (days) | 190.5 (Q1–Q3: 117–360) | 184 (Q1–Q3: 96–200) | 212 (Q1–Q3: 127–387) | |
| PPT Trapezius | 4.37 (Q1–Q3: 3.12–5.60) | 5.21 (Q1–Q3: 3.89–7.22) | 3.96 (Q1–Q3: 2.82–5.05) | |
| PPT Quadriceps | 4.43 (Q1–Q3: 3.40–6.49) | 6.21 (Q1–Q3: 3.82–9.13) | 4.33 (Q1–Q3: 3.28–5.88) | |
| TS Trapezius | 3 (Q1–Q3: 1.25–4) | 3 (Q1–Q3: 1.5–3) | 4 (Q1–Q3: 1.5–5) | |
| TS Quadriceps | 4 (Q1–Q3: 2–5) | 3 (Q1–Q3: 2.5–4) | 4 (Q1–Q3: 2–5.5) | |
| CPM Trapezius | 1.17 (Q1–Q3: 0.53–1.75) | 1.36 (Q1–Q3: 0.90–1.75) | 0.94 (Q1–Q3: 0.50–1.57) | |
| CPM Quadriceps | 1.30 (Q1–Q3: 0.58–2.24) | 0.89 (Q1–Q3: 0.47–1.87) | 1.52 (Q1–Q3: 0.77–2.31) | |
| LCADL | 22/75 (Q1–Q3: 17.25–27.50 | 15 (Q1–Q3: 15–17.5) | 25 (Q1–Q3: 22.5–32.5) | |
| PCFS patient | Grade 0 | 9.5% | 26.7% | 0.0% |
| Grade 1 | 16.7% | 33.3% | 7.4% | |
| Grade 2 | 35.7% | 26.7% | 40.7% | |
| Grade 3 | 33.3% | 13.3% | 44.4% | |
| Grade 4 | 4.8% | 0.0% | 7.4% | |
| PCFS physician | Grade 0 | 4.8% | 13.3% | 0.0% |
| Grade 1 | 14.3% | 33.3% | 3.7% | |
| Grade 2 | 33.3% | 26.7% | 37.0% | |
| Grade 3 | 42.8% | 20.0% | 55.5% | |
| Grade 4 | 2.4% | 0.0% | 3.7% | |
| Unknown | 2.4% | 6.7% | 0.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goudman, L.; De Smedt, A.; Roggeman, S.; Fernández-de-las-Peñas, C.; Hatem, S.M.; Schiltz, M.; Billot, M.; Roulaud, M.; Rigoard, P.; Moens, M. Association between Experimental Pain Measurements and the Central Sensitization Inventory in Patients at Least 3 Months after COVID-19 Infection: A Cross-Sectional Pilot Study. J. Clin. Med. 2023, 12, 661. https://doi.org/10.3390/jcm12020661
Goudman L, De Smedt A, Roggeman S, Fernández-de-las-Peñas C, Hatem SM, Schiltz M, Billot M, Roulaud M, Rigoard P, Moens M. Association between Experimental Pain Measurements and the Central Sensitization Inventory in Patients at Least 3 Months after COVID-19 Infection: A Cross-Sectional Pilot Study. Journal of Clinical Medicine. 2023; 12(2):661. https://doi.org/10.3390/jcm12020661
Chicago/Turabian StyleGoudman, Lisa, Ann De Smedt, Stijn Roggeman, César Fernández-de-las-Peñas, Samar M. Hatem, Marc Schiltz, Maxime Billot, Manuel Roulaud, Philippe Rigoard, and Maarten Moens. 2023. "Association between Experimental Pain Measurements and the Central Sensitization Inventory in Patients at Least 3 Months after COVID-19 Infection: A Cross-Sectional Pilot Study" Journal of Clinical Medicine 12, no. 2: 661. https://doi.org/10.3390/jcm12020661