
Polyorchidism: An Up-to-Date Systematic Review

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Assessment
- Review articles and conference abstracts;
- Incomplete or impossible to extract data;
- Or research performed on animals.
2.3. Data Extraction
2.4. Study Endpoints
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
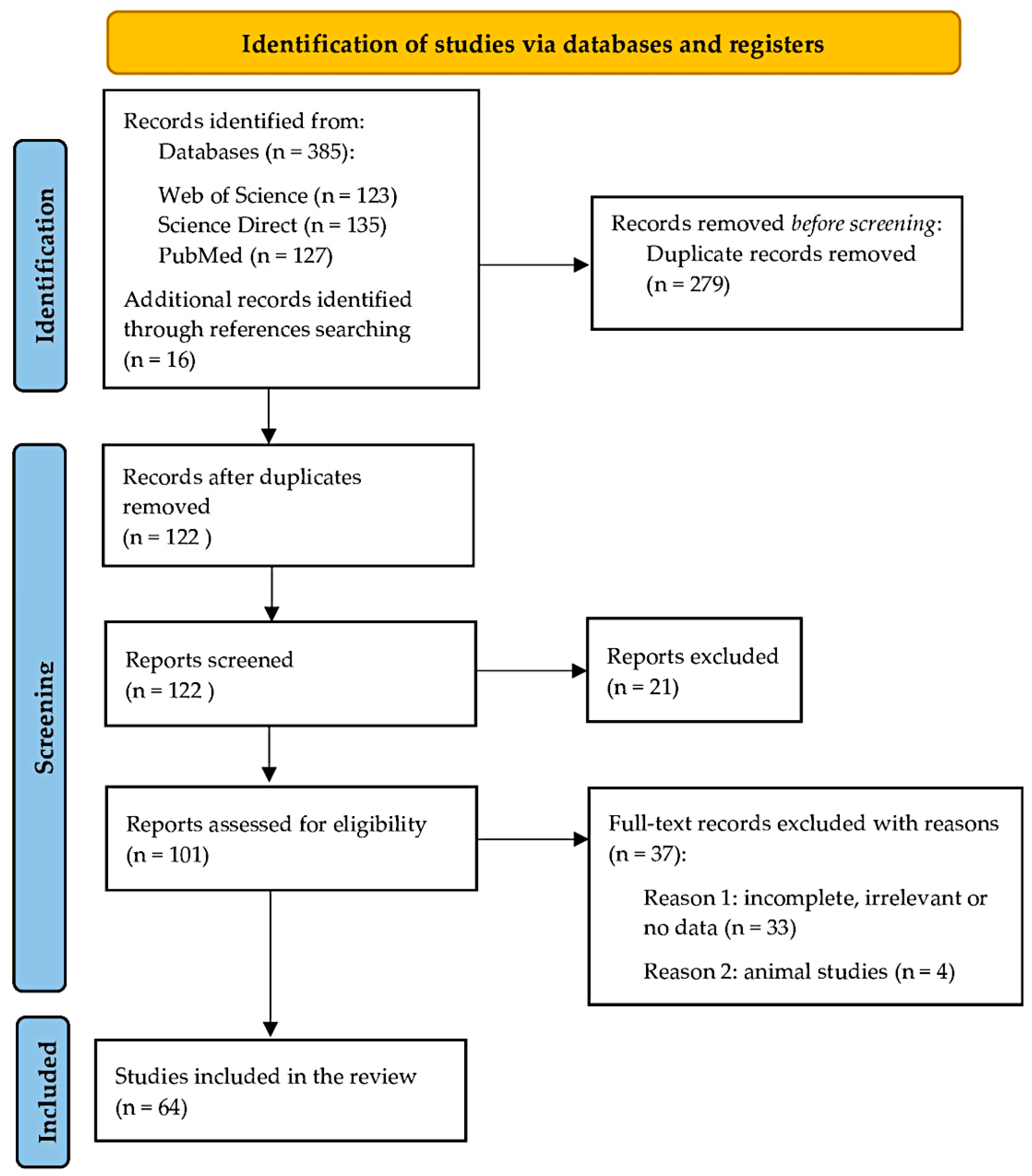
3.1. Study Identification
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
3.4. Prevalence of Polyorchidism and Localization of the SNT
3.5. Types of Polyorchidism
3.6. Radiological Examinations of the SNT
3.7. Conditions and Symptoms Associated with Polyorchidism
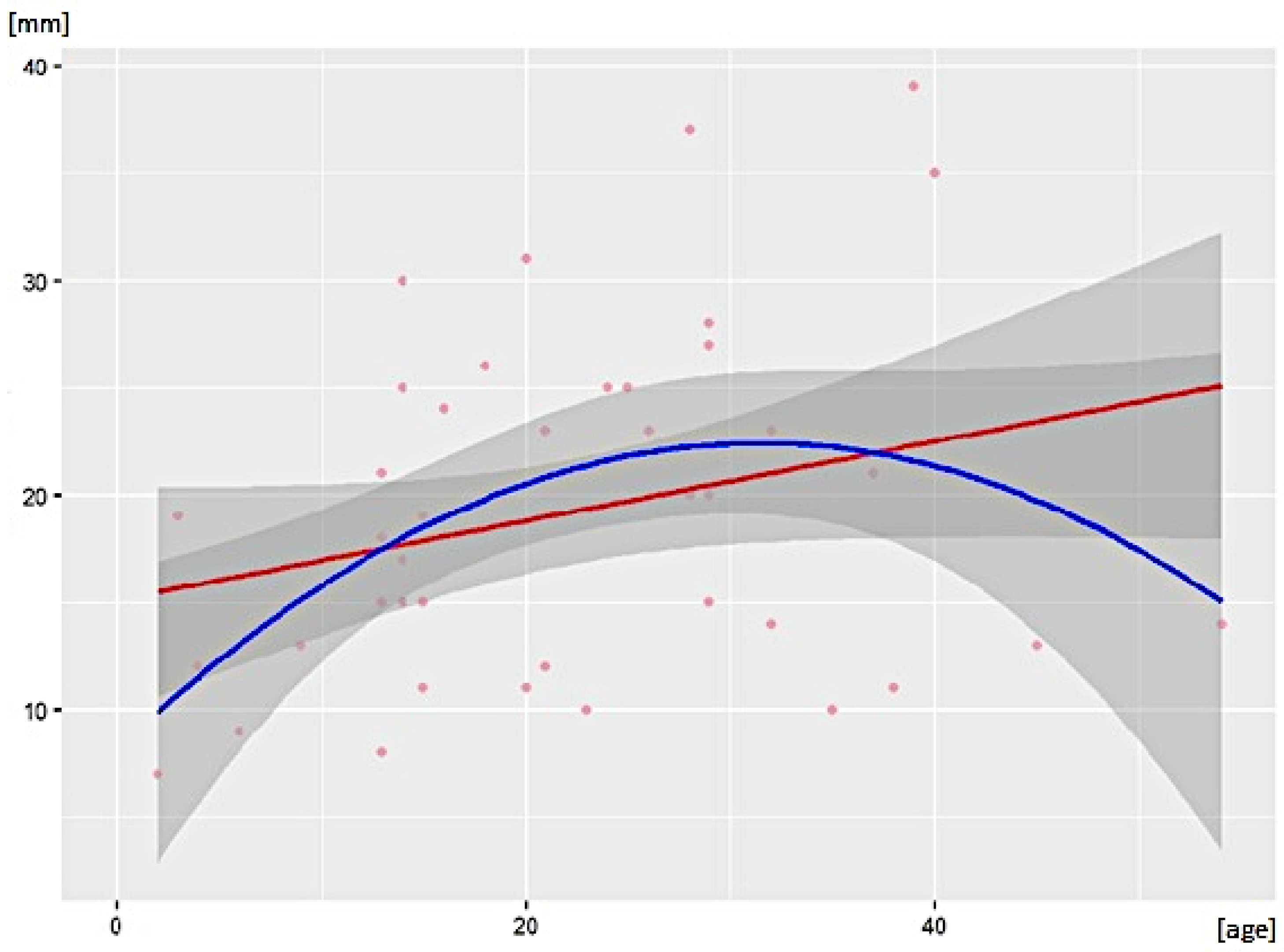
3.8. Size of the SNT
3.9. Type of Treatment
3.10. Tetraorchidism and Pentaorchidism
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uğuz, S.; Gürağaç, A.; Demirer, Z.; Yilmaz, S.; Aydur, E. Bilateral polyorchidism with ipsilateral two undescended testes: A rare congenital anomaly. Andrologia 2017, 49, e12643. [Google Scholar] [CrossRef] [PubMed]
- Lawrentschuk, N.; MacGregor, R.J. Polyorchidism: A case report and review of the literature. ANZ J. Surg. 2004, 74, 1130–1132. [Google Scholar] [CrossRef] [PubMed]
- Bergholz, R.; Wenke, K. Polyorchidism: A Meta-Analysis. J. Urol. 2009, 182, 2422–2427. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; McKenzie, J.E. Introduction to preferred reporting items for systematic reviews and meta-analyses 2020 and implications for research synthesis methodologists. Res. Synth. Methods 2022, 13, 156–163. [Google Scholar] [CrossRef]
- Bergholz, R.; Koch, B.; Spieker, T.; Lohse, K. Polyorchidism: A case report and classification. J. Pediatr. Surg. 2007, 42, 1933–1935. [Google Scholar] [CrossRef]
- Henry, B.M.; Tomaszewski, K.A.; Walocha, J.A. Methods of Evidence-Based Anatomy: A guide to conducting systematic reviews and meta-analysis of anatomical studies. Ann. Anat. 2016, 205, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandalia, U.; Pakdemirli, E. A case of triorchidism. Radiol. Case Rep. 2020, 15, 1643–1645. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, S. Case report of a rare variant of polyorchidism. J. Pediatr. Surg. Case Rep. 2016, 5, 30–31. [Google Scholar] [CrossRef] [Green Version]
- Alamsahebpour, A.; Hidas, G.; Kaplan, A.; McAleer, I.M. Bilateral Polyorchidism with Diffuse Microlithiasis: A Case Report of an Adolescent with 4 Testes. Urology 2013, 82, 1421–1423. [Google Scholar] [CrossRef]
- Ibrahim, H.; Roberts, M.J.; Hussey, D. Quadruple Orchidopexy for Torsion Testis in an Adolescent with Polyorchidism: A Case Report. Urology 2016, 87, 196–199. [Google Scholar] [CrossRef]
- Ojili, V.; Shanbhogue, K.P.; Doherty, G.P. An unusual case of polyorchidism with three homolateral testes and contralateral anorchia. Eur. J. Radiol. Extra 2009, 72, e129–e131. [Google Scholar] [CrossRef]
- Leodoro, B.; Beasley, S.; Stringer, M. Polyorchidism with presumed contralateral intrauterine testicular torsion. Int. J. Surg. Case Rep. 2014, 5, 865–867. [Google Scholar] [CrossRef] [Green Version]
- Haley, M.J.; Arkovitz, M.S. Polyorchidism in a child with imperforate anus. J. Pediatr. Surg. 2008, 43, 1548–1550. [Google Scholar] [CrossRef]
- Repetto, P.; Ceccarelli, P.; Bianchini, A.; Durante, V.; Biondini, D.; Cacciari, A. Three small testes in left hemiscrotum: A rarer caseof polyorchidism. J. Pediatr. Surg. 2010, 45, e21–e23. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, A.; Tuncel, S.A.; Hamarat, M. Polyorchidism: Color Doppler ultrasonography and magnetic resonance imaging findings. Clin. Imaging 2013, 37, 189–191. [Google Scholar] [CrossRef]
- Méndez-Gallart, R.; Estevez-Martínez, E.; Rodríguez-Barca, P.; García-Palacios, M.; Bautista-Casasnovas, A. Incomplete unilateral polyorchidism (bilobed testicle) mimicking testicular tumour. J. Pediatr. Surg. 2012, 47, 2140–2142. [Google Scholar] [CrossRef] [PubMed]
- Sarma, S.K.; Ranjit, P. Polyorchidism: A rare congenital anomaly. Eur. J. Radiol. Extra 2008, 66, e29–e31. [Google Scholar] [CrossRef]
- Ozturk, E.; Mutlu, H.; Erdem, I.; Sildiroglu, H.O. Polyorchidism: Report of a case and review of the literature. Eur. J. Radiol. Extra 2006, 58, 93–95. [Google Scholar] [CrossRef]
- Ferro, F.; Iacobelli, B. Polyorchidism and torsion. A lesson from 2 cases. J. Pediatr. Surg. 2005, 40, 1662–1664. [Google Scholar] [CrossRef]
- Spranger, R.; Gunst, M.; Kühn, M. Polyorchidism: A strange anomaly with unsuspected properties. J. Urol. 2002, 168, 198. [Google Scholar] [CrossRef]
- Tigabie, W.; Belachew, D. Triorchidism: Unilateral double atrophic undescended testis in Tertiary Specialized Hospital, Ethiopia. J. Pediatr. Surg. Case Rep. 2020, 61, 101633. [Google Scholar] [CrossRef]
- Bayissa, B.B.; Tesfaye, D. Triorchidism; an incidental finding at inguinal hernia repair: A case report. Int. J. Surg. Case Rep. 2020, 77, 813–815. [Google Scholar] [CrossRef] [PubMed]
- Cohen, T.; Agard, H.; Parekh, N.; Clark, C. Management of Bilateral Undescended Bilobed Testes and Review of the Literature. Urology 2017, 110, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Boussaffa, H.; Naouar, S.; Ati, N.; Amri, M.; Ben Khelifa, B.; Salem, B.; El Kamel, R. Neoplasm of a supernumerary undescended testis: A case report and review of the literature. Int. J. Surg. Case Rep. 2018, 53, 345–347. [Google Scholar] [CrossRef]
- Myers, A.; Morganstern, B.; Fine, R. A Unique Case of Pentaorchidism. Urology 2017, 104, 196–197. [Google Scholar] [CrossRef]
- Kumar, B.; Sharma, C.; Sinha, D. Supernumerary testis: A case report and review of literature. J. Pediatr. Surg. 2008, 43, E9–E10. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, A.H. A Case Report: Triorchidism; is a Rare Mistaken Cause for Extra Testicular Neoplasm. Urol. Case Rep. 2015, 3, 89–91. [Google Scholar] [CrossRef] [Green Version]
- Aldughiman, A.W.; El-Tholoth, H.S.; Alsunbul, A.; Badawy, E.; Alelaiwai, A. Management of polyorchidism in a prepubertal boy: A case report and literature review. Urol. Ann. 2020, 12, 385–387. [Google Scholar] [CrossRef]
- Ojaghzadeh, D.; Mahmoudpour, M.; Ezzati, N.; Milani, A.A. Polyorchidism in ultrasound examination: A case report. Andrologia 2021, 53, e13832. [Google Scholar] [CrossRef]
- Zahirian, M.T.; Mohseni, R.H.; Zandian, H.; Hosseinkhani, A. Five testicles in the genital area of a thirteen-month-old baby: A case report. BMC Urol. 2020, 20, 128. [Google Scholar] [CrossRef]
- Fonseca-Sosa, F.K. Polyorchidism and inguinoscrotal hernia. Case presentation. Poliorquidismo y hernia inguinoescrotal. presentación de un caso. Arch Esp Urol. 2019, 72, 616–618. [Google Scholar]
- Nepal, S.P.; Nakasato, T.; Naoe, M.; Shimoyama, H.; Ogawa, Y.; Fuji, K.; Maeda, Y.; Morita, J.; Oshinomi, K.; Matsui, Y.; et al. Management of right-sided polyorchidism with torsion: A case report with literature review. Urol. Sci. 2019, 30, 191. [Google Scholar] [CrossRef]
- Özman, O.; Yener, S.; Selçuk, B.; Önal, B. Polyorchidism: A Case Report and Review of the Literature. J. Urol. Surg. 2018, 5, 211–213. [Google Scholar] [CrossRef]
- Kealey, J.; Yao, H.H.; Grummet, J. Acute scrotum-Torsion of the third testicle! Urol. Case Rep. 2018, 20, 92–93. [Google Scholar] [CrossRef] [PubMed]
- Lustig, D.B.; Martin, K.; Nasr, A. Management of supernumerary testis: A rare case of polyorchidism in a 2-year-old boy. Ann. Pediatr. Surg. 2017, 13, 225–227. [Google Scholar] [CrossRef]
- Gune, A.R.; Gune, R.P. Triorchidism: A rare case report. Afr. J. Urol. 2021, 27, 15. [Google Scholar] [CrossRef]
- Di Cosmo, G.; Silvestri, T.; Bucci, S.; Bertolotto, M.; Trombetta, C. A singular case of polyorchidism. Arch. Ital. di Urol. e Androl. 2016, 88, 333–334. [Google Scholar] [CrossRef] [Green Version]
- Bhandarwar, A.H.; Gandhi, S.S.; Patel, C.B.; Wagh, A.N.; Gawli, V.; Jain, N.A. Triorchidism: Presenting as Undescended Testis in a Case of Indirect Inguinal Hernia. Clin. Pr. 2016, 6, 786. [Google Scholar] [CrossRef] [Green Version]
- Rafailidis, V.; Arvaniti, M.; Rafailidis, D.; Sfoungaris, D. Multiparametric ultrasound findings in a patient with polyorchidism. Ultrasound 2017, 25, 177–181. [Google Scholar] [CrossRef]
- Balasar, M.; Sönmez, M.G.; Oltulu, P.; Kandemir, A.; Kılıç, M.; Göger, Y.E.; Pişkin, M.M. Polyorchidism; unilateral, one atrophic undescended double testicles. Urol. Ann. 2017, 9, 208–210. [Google Scholar] [CrossRef]
- Celik, O.; Budak, S.; Cakmak, O.; Tarhan, H.; Yalbuzdag, O.N.; Peker, A.; Ilbey, Y.O. Triorchidism: A rare genital abnormality. Asian J. Androl. 2014, 16, 923–924. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.P.; Sreejayan, M.P. Management of supernumerary testis in an adult: Case report and review. Andrologia 2011, 43, 149–152. [Google Scholar] [CrossRef]
- Arlen, A.M.; Holzman, S.A.; Weiss, A.D.; Garola, R.E.; Cerwinka, W.H. Functional supernumerary testis in a child with testicular torsion and review of polyorchidism. Pediatr. Surg. Int. 2014, 30, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Jakhere, S.G.; Saifi, S.A.; Ranwaka, A.A. Supernumerary testis: Imaging appearance of a rare entity. Indian J. Urol. 2014, 30, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Belba, A.; Riversi, V.; Mari, F.; Cellesi, E.; Ponchietti, R. Triorchidism: Genetic and imaging evaluation in an adult male. Arch. Ital. Urol. Androl. 2014, 86, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Sağlam, H.S.; Önol, F.F.; Avcı, E.; Erguven, A. Report of a boy with polyorchidism and a review of current knowledge regarding this unusual anomaly. Turk. J. Urol. 2013, 39, 119–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chintamani, J.; Nyapathy, V.; Chauhan, A.; Krishnamurthy, U. Supernumerary Testis. J. Radiol. Case Rep. 2009, 3, 29–32. [Google Scholar] [CrossRef]
- Hassan, A.; El-Mogy, S.; Mostafa, T. Triorchidism: A case report and review of similar conditions. Andrologia 2008, 40, 265–269. [Google Scholar] [CrossRef]
- Khedis, M.; Nohra, J.; Dierickx, L.; Walschaerts, M.; Soulié, M.; Thonneau, P.F.; Plante, P.; Huyghe, E. Polyorchidism: Presentation of 2 Cases, Review of the Literature and a New Management Strategy. Urol. Int. 2008, 80, 98–101. [Google Scholar] [CrossRef]
- Rajbabu, K.; Morel, J.; Thompson, P.; Sidhu, P.S. Multi-cystic (rete testis) supernumerary testis in polyorchidism with underlying microlithiasis: Ultrasound features. Australas. Radiol. 2007, 51, B56–B58. [Google Scholar] [CrossRef] [PubMed]
- Bhogal, R.H.; Palit, A.; Prasad, K.K. Conservative management of polyorchidism in a young man: A case report and review of literature. Pediatr. Surg. Int. 2007, 23, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Nane, I.; Özkan, L.; Ander, H. Inguinal orchiectomy for the extra testis with suspected tumor in a polyorchidic patient: A case report. Int. Urol. Nephrol. 2007, 39, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Deveci, S.; Aygün, C.; Agildere, A.M.; Ozkardes, H. Bilateral double by testis: Evaluation magnetic resonance imaging. Int. J. Urol. 2004, 11, 813–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danrad, R.; Ashker, L.; Smith, W. Polyorchidism: Imaging may denote reproductive potential of accessory testicle. Pediatr. Radiol. 2004, 34, 492–494. [Google Scholar] [CrossRef]
- de Buys Roessingh, A.S.; El Ghoneimi, A.; Enezian, G.; Aigrain, Y. Triorchidism and testicular torsion in a child. J. Pediatr. Surg. 2003, 38, E13–E14. [Google Scholar] [CrossRef]
- Chung, T.-J.; Yao, W.-J. Sonographic features of polyorchidism. J. Clin. Ultrasound 2002, 30, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Schafer, E.S. The Sonographic Appearance of Polyorchidism: A Multiple Case Report. J. Diagn. Med Sonogr. 2019, 35, 499–503. [Google Scholar] [CrossRef]
- Duymuş, M.; Menzilcioğlu, M.S.; Çetinçakmak, M.; Avcu, S. A Rare Case of Polyorchidism: Four Testes. Pol. J. Radiol. 2016, 81, 39–41. [Google Scholar] [CrossRef] [Green Version]
- Ghose, A.; Rodrigues, G.; Izawa, J. Two primary seminomas in a patient with polyorchidism. Can. Urol. Assoc. J. 2007, 1, 285–287. [Google Scholar] [CrossRef] [Green Version]
- Topsakal, K.; Ak, H.; Yumurtas, N. Polyorchidism with varicocele: A case report and review of literature. Andrologia 2012, 44, 829–832. [Google Scholar] [CrossRef]
- Balawender, K.; Wiatr, T.; Wawrzyniak, A.; Orkisz, S. Management of Incidental Finding of Triorchidism Diagnosed during Routine Hernia Repair. Res. Rep. Urol. 2021, ume 13, 127–131. [Google Scholar] [CrossRef]
- Nikolic, O.; Stankov, M.; Popov, M.; Dajko, S.T.; Golusin, Z. Supernumerary testicle presented as an extra scrotal lump. J. Ultrasound 2022, 25, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Beiko, D.; MacNeily, A.E. Torsion of bilobed testis and biopsy-proven ipsilateral supernumerary testis in an adolescent. Can. Urol. Assoc. J. 2010, 4, E67–E70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Carli, C.; Guerra, L.; Leonard, M. Bilobed testicle in children: Diagnosis and management. Can. Urol. Assoc. J. 2009, 3, E87–E88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haffar, A.; Crigger, C.; Goldinger, M.; Jaffe, T. Two halves of a whole: Bilobed testis case report and implications in management of a rare condition. Urol. Case Rep. 2021, 38, 101737. [Google Scholar] [CrossRef]
- Halliday, L.J. Management of a bilobed testicle in a 12-year-old boy. J. Surg. Case Rep. 2013, 2013, rjt112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajbafzadeh, A.-M.; Ghahestani, S.M.; Zamani, M.M.; Kajbafzadeh, M.; Kia, M.M. A Novel Approach in Eight Polyorchidism Cases: Vasoepidydimal or Epididymo-epididymal Approximation in Single Vas Deferens Duplicated Testis. Urology 2012, 79, 1346–1349. [Google Scholar] [CrossRef]
- Jackson, D.F.; Bronson, M.A.; Neff, W.G. Polyorchidism. J. Diagn. Med. Sonogr. 2005, 21, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Lip, S.Z.L.; Murchison, L.E.D.; Cullis, P.; Govan, L.; Carachi, R. A meta-analysis of the risk of boys with isolated cryptorchidism developing testicular cancer in later life. Arch. Dis. Child. 2013, 98, 20–26. [Google Scholar] [CrossRef]
- Giwercman, A.; Grindsted, J.; Hansen, B.; Jensen, O.M.; Skakkebaek, N.E. Testicular Cancer Risk in Boys with Maldescended Testis: A Cohort Study. J. Urol. 1987, 138, 1214–1216. [Google Scholar] [CrossRef]
- Paniagua, R.; Martín, A.; Nistal, M.; Amat, P. Testicular involution in elderly men: Comparison of histologic quantitative studies with hormone patterns. Fertil. Steril. 1987, 47, 671–679. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year of Publ. | Age | # of SNT | SNT Localization | SNT Laterality | US | MRI | Treatment Options | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Observation | Orchidopexy | Orchidectomy | ||||||||
| Mandalia [7] | 2020 | 13 | 1 | S | L | Y | Y | Y | - | - |
| Chowdhary [8] | 2016 | 1 | 1 | E | L | N | N | - | Y | - |
| Alamsahebpour [9] | 2013 | 13 | 2 | S | L & R | Y | N | Y | - | |
| Ibrahim [10] | 2016 | 13 | 2 | S | L & R | Y | N | - | Y | - |
| Vijayanadh [11] | 2009 | 37 | 1 | E | R | Y | Y | Y | - | - |
| Leodoro [12] | 2014 | 2 | 1 | S | R | Y | N | - | Y | - |
| Haley [13] | 2008 | 1 | 1 | E | R | N | N | - | - | Y |
| Repetto [14] | 2010 | 2 | 2 | S | L | Y | Y | Y | - | |
| Arslanoglu [15] | 2012 | 20 | 1 | S | L | Y | Y | - | - | Y |
| Méndez-Gallart [16] | 2012 | 4 | 1 | S | L | Y | N | - | - | Y |
| Sarma [17] | 2008 | 16 | 1 | S | L | Y | N | Y | - | |
| Bergholz [5] | 2007 | 6 | 1 | E | R | N | N | - | - | Y |
| Ersin [18] | 2006 | 21 | 1 | S | L | Y | Y | Y | - | - |
| Ferro [19] | 2005 | 12 | 1 | S | L | Y | N | - | Y | - |
| Spranger [20] | 2002 | 23 | 2 | S | L & R | Y | Y | Y | - | - |
| Tigabie [21] | 2020 | 4 | 1 | E | L | Y | N | - | - | Y |
| Bayissa [22] | 2020 | 43 | 1 | E | R | N | N | - | - | Y |
| Cohen [23] | 2017 | 1 | 2 | S | L & R | Y | N | - | Y | - |
| Boussaffa [24] | 2018 | 41 | 1 | S | R | N | N | - | - | Y |
| Myers [25] | 2017 | 14 | 3 | S | 2L & R | Y | Y | Y | - | - |
| Kumar [26] | 2008 | 3 | 1 | E | L | Y | Y | - | Y | - |
| Abduljabbar [27] | 2015 | 25 | 1 | S | L | Y | Y | Y | - | - |
| Aldughiman [28] | 2020 | 14 | 1 | S | L | Y | Y | Y | - | - |
| Ojaghzadeh [29] | 2020 | 18 | 1 | S | R | Y | Y | Y | - | - |
| Moghadam [30] | 2020 | 1 | 3 | E | 2L & R | Y | N | - | Y | - |
| Fonseca-Sosa [31] | 2019 | 32 | 1 | E | R | Y | N | - | Y | - |
| Nepal [32] | 2019 | 21 | 1 | S | R | Y | Y | - | Y | - |
| Özman [33] | 2018 | 29 | 1 | S | L | Y | Y | Y | - | - |
| Kealey [34] | 2018 | 29 | 1 | S | L | Y | N | - | Y | - |
| Ben Lustig [35] | 2017 | 2 | 1 | E | L | N | N | - | Y | - |
| Gune [36] | 2021 | 28 | 1 | S | L | Y | N | Y | - | - |
| Di Cosmo [37] | 2016 | 45 | 1 | S | R | Y | N | - | - | Y |
| Bhandarwar [38] | 2016 | 24 | 1 | E | L | N | N | - | - | Y |
| Rafailidis [39] | 2017 | 15 | 1 | S | L | Y | Y | - | - | - |
| Uğuz [1] | 2016 | 20 | 2 | S & E | L & R | Y | Y | - | - | Y |
| Balasar [40] | 2017 | 4 | 1 | E | L | N | N | - | - | Y |
| Celik [41] | 2014 | 28 | 1 | S | L | Y | Y | Y | - | Y |
| Nayak [42] | 2011 | 20 | 1 | S | L | N | N | - | Y | - |
| Arlen [43] | 2014 | 14 | 1 | S | L | Y | N | - | Y | - |
| Jakhere [44] | 2014 | 52 | 1 | S | L | Y | Y | Y | - | - |
| Belba [45] | 2014 | 54 | 1 | S | L | Y | Y | Y | - | - |
| Sağlam [46] | 2013 | 14 | 1 | S | L | Y | Y | Y | - | - |
| Lawrentschuk [2] | 2004 | 15 | 1 | S | R | Y | N | - | Y | - |
| Chintamani [47] | 2009 | 13 | 1 | S | L | Y | Y | Y | - | - |
| Hassan [48] | 2008 | 32 | 1 | S | R | Y | Y | Y | - | - |
| Khedis [49] | 2008 | 47 | 2 | S | L & R | Y | N | - | - | Y |
| Rajbabu [50] | 2007 | 37 | 1 | S | L | Y | N | Y | - | - |
| Bhogal [51] | 2007 | 15 | 1 | S | R | Y | Y | Y | - | - |
| Nane [52] | 2007 | 29 | 1 | S | L | Y | Y | - | - | Y |
| Deveci [53] | 2004 | 26 | 1 | S | L | Y | Y | Y | - | - |
| Danrad [54] | 2004 | 9 | 1 | S | L | Y | Y | Y | - | - |
| Roessingh [55] | 2003 | 14 | 1 | S | R | N | N | - | Y | - |
| Spranger [20] | 2002 | 23 | 1 | S | L & R | Y | Y | Y | - | - |
| Chung [56] | 2001 | 35 | 2 | S | L | Y | Y | Y | - | - |
| Schafer [57] | 2018 | 38 | 1 | S | L | Y | N | Y | - | - |
| Duymuş [58] | 2016 | 40 | 2 | S | L | Y | Y | Y | - | - |
| Ghose [59] | 2007 | 39 | 1 | E | R | Y | Y | - | - | Y |
| Topsakal [60] | 2011 | 20 | 1 | S | R | Y | Y | - | Y | - |
| Balawender [61] | 2021 | 29 | 1 | E | R | Y | N | - | - | Y |
| Nikolic [62] | 2021 | 28 | 1 | E | R | Y | Y | - | - | Y |
| Beiko [63] | 2010 | 13 | 1 | S | L | Y | N | - | Y | - |
| De Carli [64] | 2009 | 3 | 1 | S | L | Y | N | Y | - | - |
| Haffar [65] | 2021 | 39 | 1 | S | L | Y | N | Y | - | - |
| Halliday [66] | 2013 | 12 | 1 | S | L | Y | N | Y | - | - |
| Study | Risk of Bias | |||||
|---|---|---|---|---|---|---|
| Objective(s) and Subject Characteristics | Study Design | Methodology Characterisation | Descriptive Anatomy | Reporting of Results | ||
| Mandalia [7] | 2020 | High | Low | High | Low | Low |
| Chowdhary [8] | 2016 | High | Low | High | Low | Low |
| Alamsahebpour [9] | 2013 | High | Low | High | Low | Low |
| Ibrahim [10] | 2016 | High | Low | High | Low | Low |
| Vijayanadh [11] | 2009 | High | Low | High | Low | Low |
| Leodoro [12] | 2014 | High | Low | High | High | Low |
| Haley [13] | 2008 | High | High | High | Low | Low |
| Repetto [14] | 2010 | High | Low | High | Low | Low |
| Arslanoglu [15] | 2012 | Low | Low | High | Low | Low |
| Méndez-Gallart [16] | 2012 | Low | Low | High | Low | Low |
| Sarma [17] | 2008 | High | Low | High | Low | Low |
| Bergholz [5] | 2007 | High | Low | High | Low | Low |
| Ersin [18] | 2006 | High | High | Low | High | Low |
| Ferro [19] | 2005 | High | Low | High | Low | Low |
| Spranger [20] | 2002 | High | Low | High | Low | Low |
| Tigabie [21] | 2020 | High | Low | High | Low | Low |
| Bayissa [22] | 2020 | Low | Low | High | Low | Low |
| Cohen [23] | 2017 | High | Low | High | High | Low |
| Boussaffa [24] | 2018 | High | Low | Low | Low | Low |
| Myers [25] | 2017 | High | High | High | Low | Low |
| Kumar [26] | 2008 | High | Low | High | Low | Low |
| Abduljabbar [27] | 2015 | High | Low | High | Low | Low |
| Aldughiman [28] | 2020 | High | Low | High | Low | Low |
| Ojaghzadeh [29] | 2020 | High | Low | High | Low | Low |
| Moghadam [30] | 2020 | High | Low | High | Low | Low |
| Fonseca-Sosa [31] | 2019 | High | Low | High | Low | Low |
| Nepal [32] | 2019 | High | Low | High | Low | Low |
| Özman [33] | 2018 | Low | Low | High | Low | Low |
| Kealey [34] | 2018 | High | Low | High | Low | Low |
| Ben Lustig [35] | 2017 | High | Low | High | Low | Low |
| Gune [36] | 2021 | High | Low | High | Low | Low |
| Di Cosmo [37] | 2016 | High | Low | High | Low | Low |
| Bhandarwar [38] | 2016 | High | Low | High | High | Low |
| Rafailidis [39] | 2017 | Low | Low | High | Low | Low |
| Uğuz [1] | 2016 | High | Low | High | Low | Low |
| Balasar [40] | 2017 | High | Low | High | Low | Low |
| Celik [41] | 2014 | High | Low | High | Low | Low |
| Nayak [42] | 2011 | High | Low | High | Low | Low |
| Arlen [43] | 2014 | High | Low | Low | Low | Low |
| Jakhere [44] | 2014 | High | Low | Low | Low | Low |
| Belba [45] | 2014 | High | Low | High | Low | Low |
| Sağlam [46] | 2013 | High | Low | High | High | Low |
| Lawrentschuk [2] | 2004 | High | Low | High | Low | Low |
| Chintamani [47] | 2009 | High | Low | High | Low | Low |
| Hassan [48] | 2008 | High | Low | High | Low | Low |
| Khedis [49] | 2008 | High | Low | High | Low | Low |
| Rajbabu [50] | 2007 | High | Low | High | Low | Low |
| Bhogal [51] | 2007 | High | Low | High | Low | Low |
| Nane [52] | 2007 | High | Low | High | Low | Low |
| Deveci [53] | 2004 | High | Low | High | Low | Low |
| Danrad [54] | 2004 | High | Low | High | Low | Low |
| Roessingh [55] | 2003 | High | Low | High | Low | Low |
| Spranger [20] | 2002 | High | Low | High | Low | Low |
| Chung [56] | 2001 | High | Low | High | Low | Low |
| Schafer [57] | 2018 | High | Low | High | Low | Low |
| Duymuş [58] | 2016 | High | Low | High | Low | Low |
| Ghose [59] | 2007 | High | Low | Low | Low | Low |
| Topsakal [60] | 2011 | Low | Low | High | Low | Low |
| Balawender [61] | 2021 | High | Low | High | Low | Low |
| Nikolic [62] | 2021 | High | Low | High | Low | Low |
| Beiko [63] | 2010 | High | Low | High | High | Low |
| De Carli [64] | 2009 | High | Low | High | Low | Low |
| Haffar [65] | 2021 | High | Low | High | Low | Low |
| Halliday [66] | 2013 | High | Low | High | Low | Low |
| SNT Position | Surgery | Observation | Chi2 Test p-Value |
|---|---|---|---|
| Scrotal, no. of patients (%) | 18 (33) | 25 (45) | <0.001 df 1 |
| Non-scrotal, no. of patients (%) | 12 (22) | 0 (0) |
| SNT Position | Surgical Treatment | Observation | Chi2 Test p-Value |
|---|---|---|---|
| Scrotum, no. of patients (%) | 4 (13) | 11 (33) | <0.001 df 1 |
| Ectopic, no. of patients (%) | 13 (42) | 4 (13) |
| B | s.e. | p | |
|---|---|---|---|
| Variables in the linear regression model | |||
| Constans | 15.11 | 2.59 | <0.001 |
| Age | 0.18 | 0.10 | <0.10 |
| Variables in the quadratic regression model | |||
| Constans | 8.11 | 4.07 | <0.10 |
| Age | 0.91 | 0.35 | <0.05 |
| Age-squared | -0.01 | 0.01 | <0.05 |
| SNT Position | Orchidopexy | Orchidectomy | Chi2 Test p-Value |
|---|---|---|---|
| Scrotal, no. of patients (%) | 10 (59) | 7 (41) | 0.071 |
| Non-scrotal, no. of patients (%) | 3 (25) | 9 (75) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balawender, K.; Wawrzyniak, A.; Kobos, J.; Golberg, M.; Żytkowski, A.; Zarzecki, M.; Walocha, J.; Bonczar, M.; Dubrowski, A.; Mazurek, A.; et al. Polyorchidism: An Up-to-Date Systematic Review. J. Clin. Med. 2023, 12, 649. https://doi.org/10.3390/jcm12020649
Balawender K, Wawrzyniak A, Kobos J, Golberg M, Żytkowski A, Zarzecki M, Walocha J, Bonczar M, Dubrowski A, Mazurek A, et al. Polyorchidism: An Up-to-Date Systematic Review. Journal of Clinical Medicine. 2023; 12(2):649. https://doi.org/10.3390/jcm12020649
Chicago/Turabian StyleBalawender, Krzysztof, Agata Wawrzyniak, Józef Kobos, Michał Golberg, Andrzej Żytkowski, Michał Zarzecki, Jerzy Walocha, Michał Bonczar, Andrzej Dubrowski, Agata Mazurek, and et al. 2023. "Polyorchidism: An Up-to-Date Systematic Review" Journal of Clinical Medicine 12, no. 2: 649. https://doi.org/10.3390/jcm12020649