
Correlation of ENT Symptoms with Age, Sex, and Anti-SARS-CoV-2 Antibody Titer in Plasma
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Available online: https://covid19.who.int/ (accessed on 28 September 2022).
- El-Anwar, M.W.; Elzayat, S.; Fouad, Y.A. ENT manifestation in COVID-19 patients. Auris Nasus Larynx 2020, 47, 559–564. [Google Scholar] [CrossRef]
- El-Anwar, M.W.; Eesa, M.; Mansour, W.; Zake, L.G.; Hendawy, E. Analysis of Ear, Nose and Throat Manifestations in COVID-19 Patients. Int. Arch. Otorhinolaryngol. 2021, 25, e343–e348. [Google Scholar] [CrossRef]
- Zięba, N.; Lisowska, G.; Dadok, A.; Kaczmarek, J.; Stryjewska-Makuch, G.; Misiołek, M. Frequency and Severity of Ear-Nose-Throat (ENT) Symptoms during COVID-19 Infection. Medicina 2022, 58, 623. [Google Scholar] [CrossRef]
- Özçelik Korkmaz, M.; Eğilmez, O.K.; Özçelik, M.A.; Güven, M. Otolaryngological manifestations of hospitalised patients with confirmed COVID-19 infection. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1675–1685. [Google Scholar] [CrossRef] [PubMed]
- Song, K.H.; Kim, D.M.; Lee, H.; Ham, S.Y.; Oh, S.M.; Jeong, H.; Jung, J.; Kang, C.K.; Park, J.Y.; Kang, Y.M.; et al. Dynamics of viral load and anti-SARS-CoV-2 antibodies in patients with positive RT-PCR results after recovery from COVID-19. Korean J. Intern. Med. 2021, 36, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Abolghasemi, H.; Eshghi, P.; Cheraghali, A.M.; Imani Fooladi, A.A.; Bolouki Moghaddam, F.; Imanizadeh, S.; Moeini Maleki, M.; Ranjkesh, M.; Rezapour, M.; Bahramifar, A.; et al. Clinical efficacy of convalescent plasma for treatment of COVID-19 infections: Results of a multicenter clinical study. Transfus. Apher. Sci. Off. J. World Apher. Assoc. Off. J. Eur. Soc. Haemapheresis 2020, 59, 102875. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Pekosz, A.; Park, H.S.; Ursin, R.L.; Shapiro, J.R.; Benner, S.E.; Littlefield, K.; Kumar, S.; Naik, H.M.; Betenbaugh, M.J.; et al. Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population. J. Clin. Investig. 2020, 130, 6141–6150. [Google Scholar] [CrossRef]
- Uysal, E.B.; Gümüş, S.; Bektöre, B.; Bozkurt, H.; Gözalan, A. Evaluation of antibody response after COVID-19 vaccination of healthcare workers. J. Med. Virol. 2022, 94, 1060–1066. [Google Scholar] [CrossRef]
- Li, K.; Huang, B.; Wu, M.; Zhong, A.; Li, L.; Cai, Y.; Wang, Z.; Wu, L.; Zhu, M.; Li, J.; et al. Dynamic changes in anti-SARS-CoV-2 antibodies during SARS-CoV-2 infection and recovery from COVID-19. Nat. Commun. 2020, 11, 6044. [Google Scholar] [CrossRef]
- Skorek, A.; Jaźwińska-Curyłło, A.; Romanowicz, A.; Kwaśniewski, K.; Narożny, W.; Tretiakow, D. Assessment of anti-SARS-CoV-2 antibodies level in convalescents plasma. J. Med. Virol. 2022, 94, 1130–1137. [Google Scholar] [CrossRef]
- Weisberg, S.P.; Connors, T.J.; Zhu, Y.; Baldwin, M.R.; Lin, W.H.; Wontakal, S.; Szabo, P.A.; Wells, S.B.; Dogra, P.; Gray, J.; et al. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat. Immunol. 2021, 22, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Kritikos, A.; Gabellon, S.; Pagani, J.L.; Monti, M.; Bochud, P.Y.; Manuel, O.; Coste, A.; Greub, G.; Perreau, M.; Pantaleo, G.; et al. Anti-SARS-CoV-2 Titers Predict the Severity of COVID-19. Viruses 2021, 14, 1089. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, L.; Sang, L.; Ye, F.; Ruan, S.; Zhong, B.; Song, T.; Alshukairi, A.N.; Chen, R.; Zhang, Z.; et al. Kinetics of viral load and antibody response in relation to COVID-19 severity. J. Clin. Investig. 2020, 130, 5235–5244. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of April 26, 2021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef]
- Elibol, E. Otolaryngological symptoms in COVID-19. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1233–1236. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef]
- Heras, M.; Fernández-Reyes, M.J. Serum potassium concentrations: Importance of normokalaemia. Concentraciones séricas de potasio: Importancia de la normopotasemia. Med. Clin. 2017, 148, 562–565. [Google Scholar] [CrossRef]
- Zheng, Z.; Liu, C.; Shen, Y.; Xia, L.; Xiao, L.; Sun, Y.; Wang, H.; Chen, Z.; Wu, Y.; Shi, H.; et al. Serum Albumin Levels as a Potential Marker for the Predictive and Prognostic Factor in Sudden Sensorineural Hearing Loss: A Prospective Cohort Study. Front. Neurol. 2021, 12, 747561. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, A.C.; Goh, H.P.; Koh, D. Treatment of COVID-19: Old tricks for new challenges. Crit. Care 2020, 24, 91. [Google Scholar] [CrossRef]
- Johannesen, C.K.; St Martin, G.; Lendorf, M.E.; Gerred, P.; Fyfe, A.; Paton, R.S.; Thompson, C.; Molsted, S.; Kann, C.E.; Jensen, C.A.; et al. Prevalence and duration of anti-SARS-CoV-2 antibodies in healthcare workers. Dan. Med. J. 2022, 69, A11210843. [Google Scholar] [PubMed]
- Soo, Y.O.; Cheng, Y.; Wong, R.; Hui, D.S.; Lee, C.K.; Tsang, K.K.; Ng, M.H.; Chan, P.; Cheng, G.; Sung, J.J. Retrospective comparison of convalescent plasma with continuing high-dose methylprednisolone treatment in SARS patients. Clin. Microbiol. Infect. 2004, 10, 676–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, S.; Chung, C.R.; Ha, Y.E.; Han, T.H.; Ki, C.S.; Kang, E.S.; Park, J.K.; Peck, K.R.; Cho, D. Possible Transfusion-Related Acute Lung Injury Following Convalescent Plasma Transfusion in a Patient With Middle East Respiratory Syndrome. Ann. Lab. Med. 2016, 36, 393–395. [Google Scholar] [CrossRef]
- Tsuchida, T.; Hirose, M.; Inoue, Y.; Kunishima, H.; Otsubo, T.; Matsuda, T. Relationship between changes in symptoms and antibody titers after a single vaccination in patients with Long COVID. J. Med. Virol. 2022, 94, 3416–3420. [Google Scholar] [CrossRef] [PubMed]




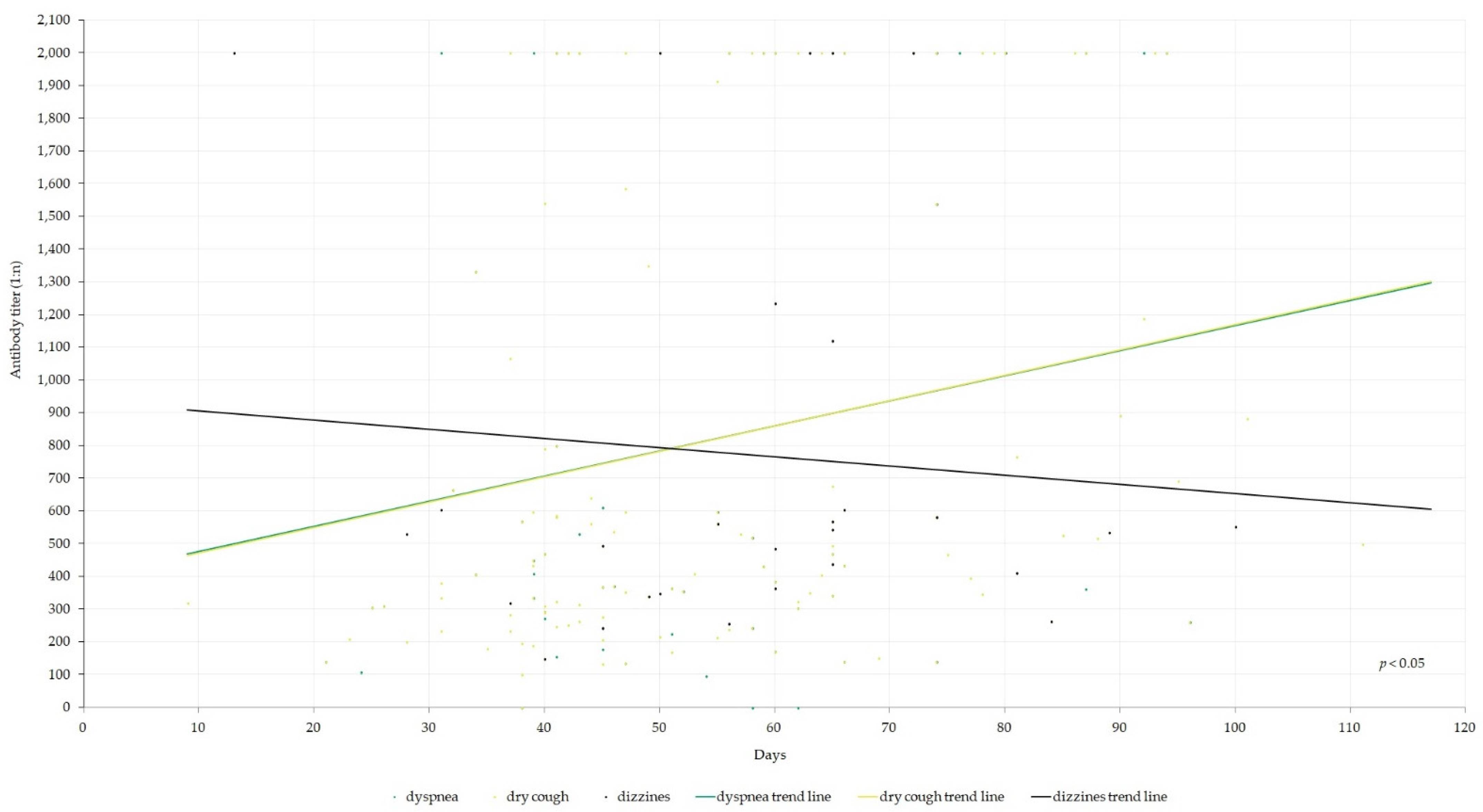{kind=link}
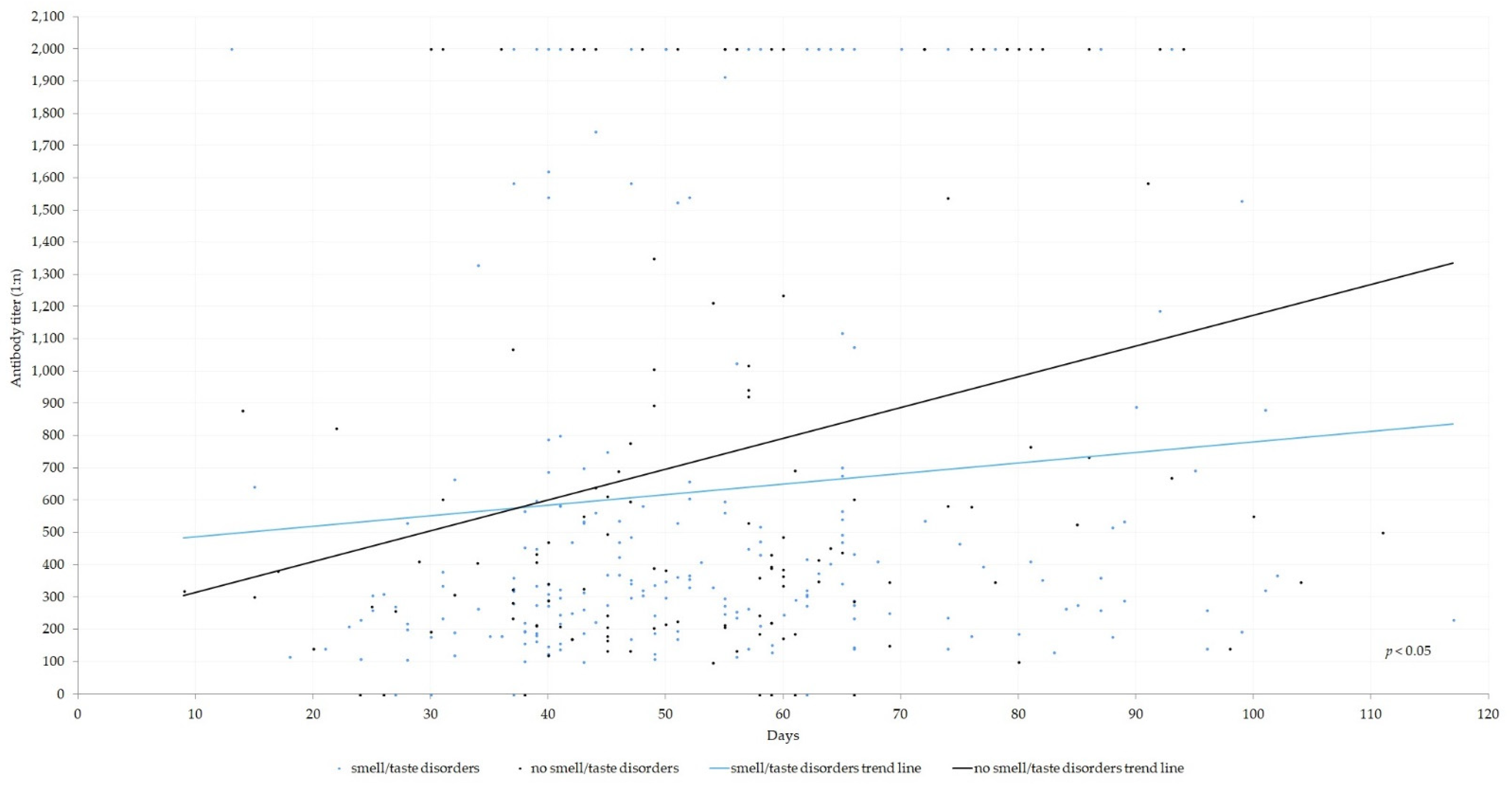{kind=link}
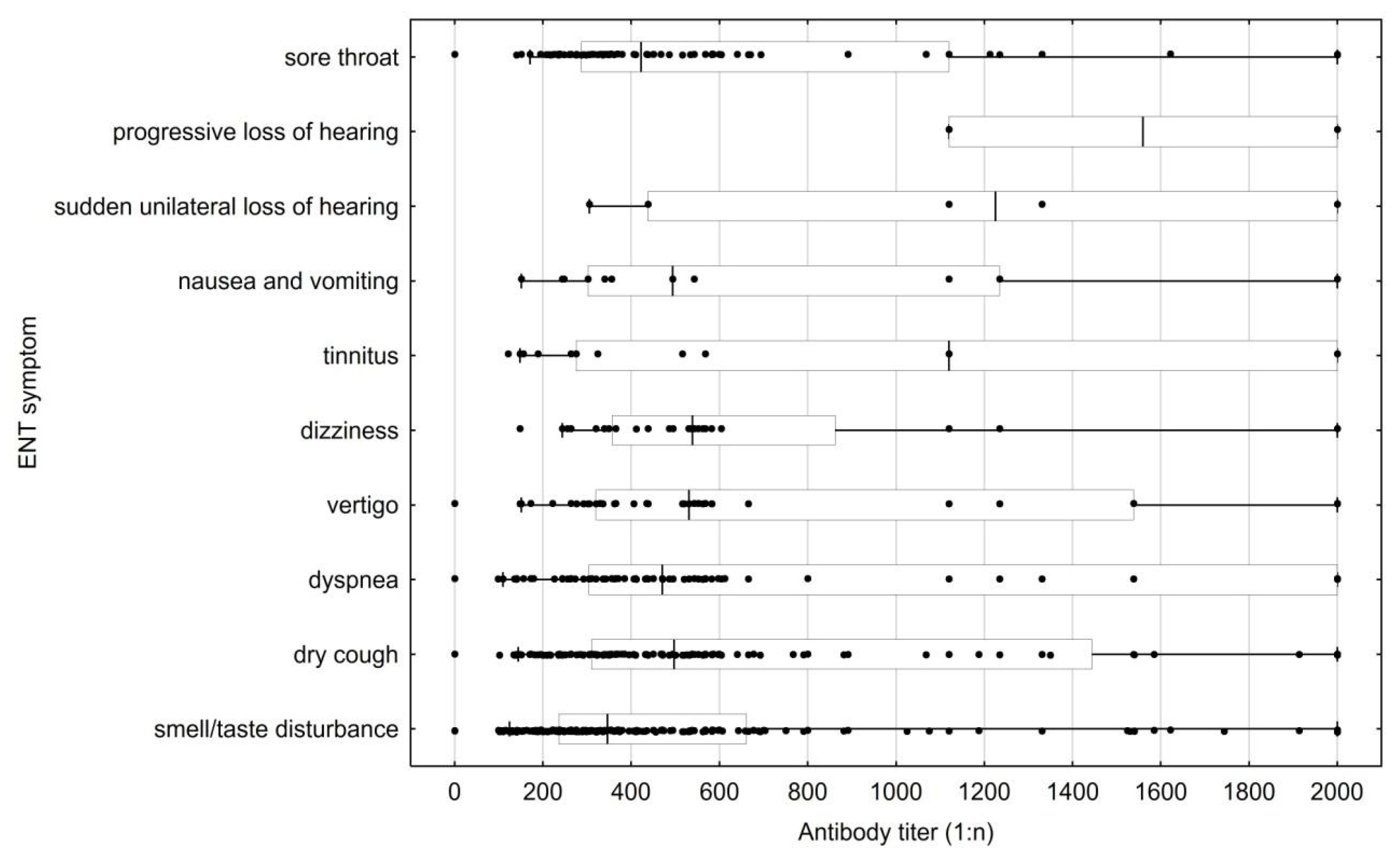{kind=link}
| Index | N |
|---|---|
| Mean age (95% CI) | 39.80 (38.79–40.81) |
| Gender | |
| Male | 302 |
| Female | 44 |
| Antibody titer | |
| <1:368.5 (male:female ratio) | 6:1 |
| >1:368.5 (male:female ratio) | 9:1 |
| Clinical information | |
| Hypertension | 9 (only males) |
| Familial hypercholesterolemia | 1 (only females) |
| No comorbidities (male:female ratio) | 7:1 |
| Ethnicity | |
| Polish (%) | 346 (100%) |
| ENT Symptom | <1:368.5 (N = 173) | >1:368.5 (N = 173) | p Value | Cohen’s h | Males (N = 302) | Females (N = 44) | p Value | Cohen’s h | Age < 39.8 (N = 167) | Age > 39.8 (N = 179) | p Value | Cohen’s h |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| smell/taste disturbance | 117 | 99 | 0.046 a | 0.215 | 184 | 32 | 0.131 a | 0.252 | 119 | 97 | 0.001 a | 0.355 |
| dry cough | 51 | 89 | <0.0001 a | 0.452 | 125 | 15 | 0.357 a | 0.151 | 65 | 75 | 0.573 a | 0.061 |
| sore throat | 39 | 47 | 0.32 a | 0.107 | 72 | 14 | 0.253 a | 0.178 | 38 | 48 | 0.382 a | 0.094 |
| dyspnea | 30 | 52 | 0.005 a | 0.302 | 72 | 10 | 0.871 a | 0.026 | 45 | 37 | 0.17 a | 0.148 |
| vertigo | 15 | 26 | 0.067 a | 0.198 | 37 | 4 | 0.544 a | 0.103 | 19 | 22 | 0.793 a | 0.028 |
| dizziness | 8 | 20 | 0.018 a | 0.26 | 26 | 2 | 0.554 b | 0.166 | 15 | 13 | 0.558 a | 0.063 |
| tinnitus | 8 | 13 | 0.26 a | 0.122 | 19 | 2 | 1 b | 0.077 | 8 | 13 | 0.336 a | 0.104 |
| nausea and vomiting | 6 | 7 | 0.786 a | 0.03 | 10 | 3 | 0.221 b | 0.162 | 6 | 7 | 0.885 a | 0.017 |
| sudden unilateral loss of hearing | 1 | 5 | 0.215 b | 0.189 | 6 | 0 | 1 b | 0.283 | 2 | 4 | 0.686 b | 0.081 |
| progressive loss of hearing | 0 | 2 | 0.499 b | 0.215 | 2 | 0 | 1 b | 0.163 | 1 | 1 | 1 b | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwaśniewska, A.; Kwaśniewski, K.; Skorek, A.; Tretiakow, D.; Jaźwińska-Curyłło, A.; Burduk, P. Correlation of ENT Symptoms with Age, Sex, and Anti-SARS-CoV-2 Antibody Titer in Plasma. J. Clin. Med. 2023, 12, 610. https://doi.org/10.3390/jcm12020610
Kwaśniewska A, Kwaśniewski K, Skorek A, Tretiakow D, Jaźwińska-Curyłło A, Burduk P. Correlation of ENT Symptoms with Age, Sex, and Anti-SARS-CoV-2 Antibody Titer in Plasma. Journal of Clinical Medicine. 2023; 12(2):610. https://doi.org/10.3390/jcm12020610
Chicago/Turabian StyleKwaśniewska, Aleksandra, Krzysztof Kwaśniewski, Andrzej Skorek, Dmitry Tretiakow, Anna Jaźwińska-Curyłło, and Paweł Burduk. 2023. "Correlation of ENT Symptoms with Age, Sex, and Anti-SARS-CoV-2 Antibody Titer in Plasma" Journal of Clinical Medicine 12, no. 2: 610. https://doi.org/10.3390/jcm12020610