
Is Thrombocytopenia an In-Hospital Mortality Risk Factor among Patients with Acute Ischemic Stroke? A Propensity Score-Matched Analysis from the MIMIC-IV Database
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
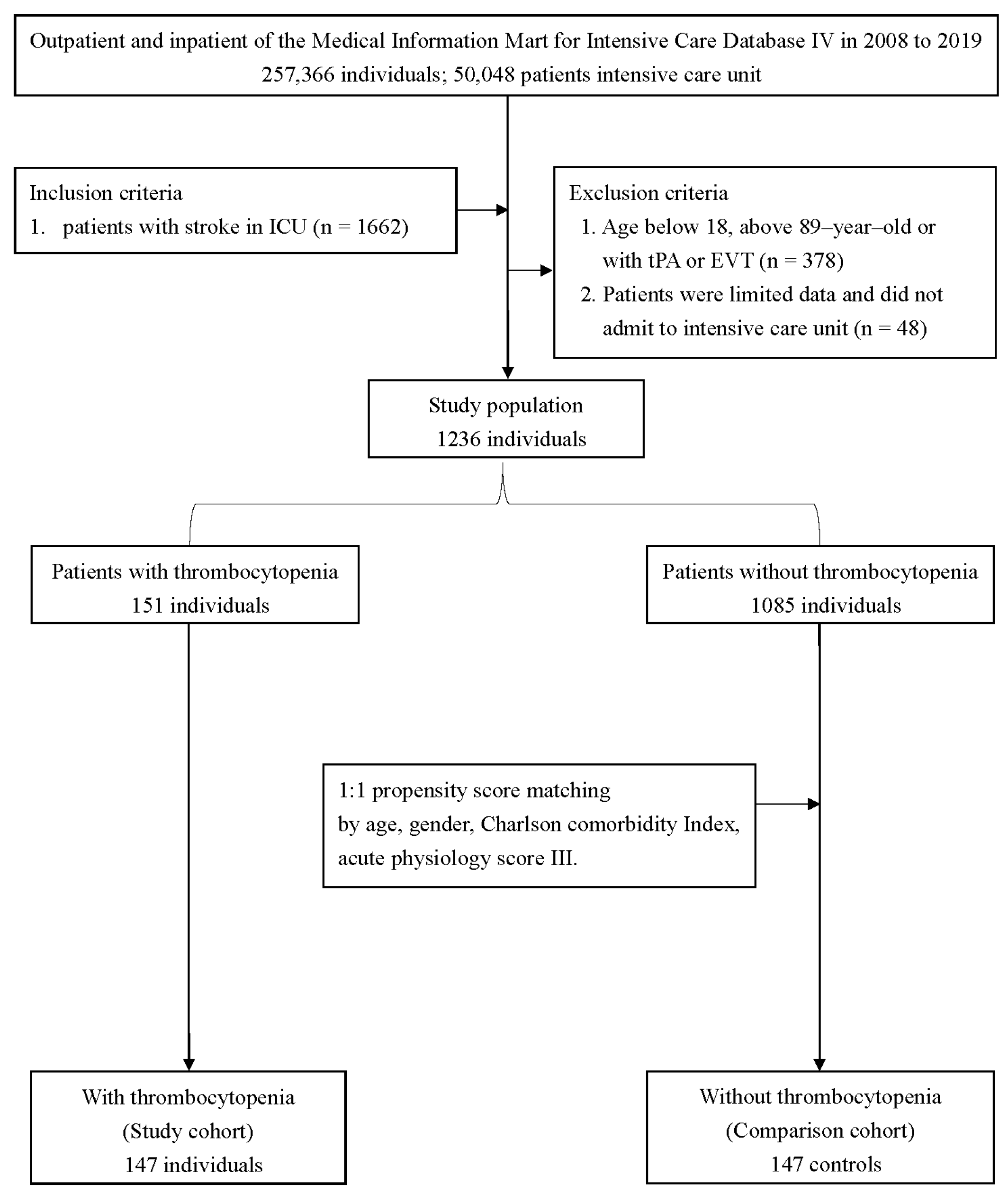
2.1. Study Population and Data Source
2.2. Study Population and Variable Extraction
2.3. Definition of Thrombocytopenia and Outcome Measurement
2.4. Statistical Analysis
3. Results
Main Text
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIS | Acute ischemic stroke |
| APS III | Acute physiology score III; BIDMC, Beth Israel Deaconess Medical Center |
| BUN | Blood urea nitrogen |
| CCI | Charlson comorbidity index |
| CPD | Chronic obstructive pulmonary disease |
| CI | Confidence interval |
| EVT | Endovascular thrombectomy |
| Hgb | Hemoglobin |
| HR | Hazard ratio |
| ICH | Intracerebral hemorrhage |
| ICU | Intensive care unit |
| INR | International normalized ratio |
| MIMIC | Multiparameter Intelligent Monitoring in Intensive Care |
| MSS | Multicenter Stroke Survey |
| NIHSS | National Institute of Health Stroke Scale |
| NOACs | Novel oral anticoagulants |
| OR | Odds ratio |
| PSM | Propensity score matching |
| PEG | Percutaneous endoscopic gastrostomy |
| PEJ | Percutaneous endoscopic jejunostomy |
| PVD | Peripheral vascular disease |
| SIRS | Systemic inflammatory response syndrome |
| SMD | Standardized mean difference |
| SOFA | Sequential organ failure assessment |
| TOAST | Trial of Org10172 in Acute Stroke Treatment |
| TP | Thrombocytopenia |
| tPA | Tissue plasminogen activator |
| WBC | White blood cell |
References
- Whisnant, J.P.; Basford, J.R.; Bernstein, E.F.; Cooper, E.S.; Dyken, M.L.; Easton, J.D.; Little, J.R.; Marler, J.R.; Millikan, C.H.; Petito, C.K.; et al. Special report from the National Institute of Neurological Disorders and Stroke. Classification of cerebrovascular diseases III. Stroke 1990, 21, 637–676. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.V.; Khatri, P. Stroke. Lancet 2020, 396, 129–142. [Google Scholar] [CrossRef]
- Pham, X.; Ray, J.; Neto, A.S.; Laing, J.; Perucca, P.; Kwan, P.; O’Brien, T.J.; Udy, A.A. Association of Neurocritical Care Services With Mortality and Functional Outcomes for Adults With Brain Injury: A Systematic Review and Meta-analysis. JAMA Neurol. 2022, 79, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Thachil, J.; Warkentin, T.E. How do we approach thrombocytopenia in critically ill patients? Br. J. Haematol. 2017, 177, 27–38. [Google Scholar] [PubMed]
- Furlan, J.C.; Fang, J.; Silver, F.L. Outcomes after acute ischemic stroke in patients with thrombocytopenia or thrombocytosis. J. Neurol. Sci. 2016, 362, 198–203. [Google Scholar] [CrossRef]
- Sico, J.J.; Phipps, M.S.; Concato, J.; Wells, C.K.; Lo, A.C.; Nadeau, S.E.; Williams, L.S.; Peixoto, A.J.; Gorman, M.; Boice, J.L.; et al. Thrombocytopenia and in-hospital mortality risk among ischemic stroke patients. J. Stroke Cerebrovasc. Dis. 2013, 22, e99–e102. [Google Scholar] [CrossRef]
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L.; et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N. Engl. J. Med. 2013, 368, 893–903. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Dai, Q.; Ye, R.; Zi, W.; Liu, Y.; Wang, H.; Zhu, W.; Ma, M.; Yin, Q.; Li, M.; et al. Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST): An open-label, randomised controlled trial. Lancet Neurol. 2020, 19, 115–122. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [Green Version]
- Hanley, D.F.; Lane, K.; McBee, N.; Ziai, W.; Tuhrim, S.; Lees, K.R.; Dawson, J.; Gandhi, D.; Ullman, N.; Mould, W.A.; et al. Thrombolytic removal of intraventricular haemorrhage in treatment of severe stroke: Results of the randomised, multicentre, multiregion, placebo-controlled CLEAR III trial. Lancet 2017, 389, 603–611. [Google Scholar] [CrossRef]
- Brown, D.L.; Levine, D.A.; Albright, K.; Kapral, M.K.; Leung, L.Y.; Reeves, M.J.; Sico, J.; Strong, B.; Whiteley, W.N.; American Heart Association Stroke Council. Benefits and Risks of Dual Versus Single Antiplatelet Therapy for Secondary Stroke Prevention: A Systematic Review for the 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack. Stroke 2021, 52, e468–e479. [Google Scholar] [CrossRef]
- Hankey, G.J. Secondary stroke prevention. Lancet Neurol. 2014, 13, 178–194. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.E.; Stone, D.J.; Celi, L.A.; Pollard, T.J. The MIMIC Code Repository: Enabling reproducibility in critical care research. J. Am. Med. Inf. Assoc. 2018, 25, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Zarychanski, R.; Houston, D.S. Assessing thrombocytopenia in the intensive care unit: The past, present, and future. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 660–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Thomas, M.R.; Storey, R.F. The role of platelets in inflammation. Thromb. Haemost. 2015, 114, 449–458. [Google Scholar] [PubMed]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Elkind, M.S.; Panageas, K.S.; DeAngelis, L.M. Risk of Arterial Thromboembolism in Patients with Cancer. J. Am. Coll. Cardiol. 2017, 70, 926–938. [Google Scholar] [CrossRef] [PubMed]
- Jhou, H.J.; Yang, L.Y.; Chen, P.H.; Lee, C.H. Endovascular therapy for acute ischemic stroke in patients with active malignancy: A meta-analysis with trial sequential analysis. J. Neurointerv. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Shimizu, M.; Kohara, S.; Takizawa, S.; Kitagawa, Y.; Takagi, S. Appearance of WBC-platelet complex in acute ischemic stroke, predominantly in atherothrombotic infarction. J. Atheroscler. Thromb. 2012, 19, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiteley, W.N.; Slot, K.B.; Fernandes, P.; Sandercock, P.; Wardlaw, J. Risk factors for intracranial hemorrhage in acute ischemic stroke patients treated with recombinant tissue plasminogen activator: A systematic review and meta-analysis of 55 studies. Stroke 2012, 43, 2904–2909. [Google Scholar] [CrossRef]
- Ntaios, G.; Papavasileiou, V.; Michel, P.; Tatlisumak, T.; Strbian, D. Predicting functional outcome and symptomatic intracranial hemorrhage in patients with acute ischemic stroke: A glimpse into the crystal ball? Stroke 2015, 46, 899–908. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.; van der Lugt, A.; De Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Propensity-Matched Pairs | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | TP Group | Non-TP Group | p Value | SMD | TP Group | Non-TP Group | p Value | SMD |
| (n = 151) | (n = 1085) | (n = 147) | (n = 147) | |||||
| Age (years) | 70.5 ± 12.8 | 68.4 ± 14.4 | 0.088 | 0.154 | 70.3 ± 12.9 | 70.6 ± 13.7 | 0.833 | 0.025 |
| Gender (Female), n | 47 (31.1%) | 529 (48.8%) | <0.001 | 0.366 | 47 (32.0%) | 50 (34.0%) | 0.710 | 0.043 |
| Race, n | 0.580 # | 0.163 | 0.538 # | 0.268 | ||||
| White | 92 (60.9%) | 728 (67.1%) | 92 (62.6%) | 102 (69.4%) | ||||
| Black | 19 (12.6%) | 98 (9.0%) | 17 (11.6%) | 9 (6.1%) | ||||
| Asian | 5 (3.3%) | 27 (2.5%) | 5 (3.4%) | 4 (2.7%) | ||||
| Other | 35 (23.12%) | 232 (21.4%) | 33 (22.4%) | 32 (21.8%) | ||||
| Comorbidities, n | ||||||||
| CCI | 7.3 ± 2.5 | 6.7 ± 2.7 | 0.010 | 0.228 | 7.3 ± 2.6 | 7.3 ± 2.9 | 1.000 | <0.001 |
| Diabetes Mellitus | ||||||||
| Without chronic complication | 37 (24.5%) | 310 (28.6%) | 0.297 | 0.092 | 37 (25.2%) | 47 (32.0%) | 0.197 | 0.151 |
| With chronic complication | 92 (8.5%) | 13 (8.6%) | 0.957 | 0.005 | 12 (8.2%) | 10 (6.8%) | 0.658 | 0.052 |
| Coronary artery disease | 18 (11.9%) | 137 (12.6%) | 0.806 | 0.022 | 18 (12.2%) | 16 (10.9%) | 0.715 | 0.043 |
| Congestive heart failure | 29 (19.2%) | 196 (18.1%) | 0.734 | 0.029 | 27 (18.4%) | 23 (15.6%) | 0.535 | 0.072 |
| PVD | 18 (11.9%) | 129 (11.9%) | 0.991 | 0.001 | 17 (11.6%) | 25 (17.0%) | 0.182 | 0.156 |
| CPD | 21 (13.9%) | 198 (18.2%) | 0.190 | 0.118 | 20 (13.6%) | 34 (23.1%) | 0.035 | 0.248 |
| Liver Disease | ||||||||
| Mild | 11 (7.3%) | 26 (2.4%) | 0.003 # | 0.229 | 11 (7.5%) | 4 (2.7%) | 0.064 | 0.218 |
| Moderate to severe | 5 (3.3%) | 2 (0.2%) | <0.001 # | 0.240 | 5 (3.4%) | 0 (0.0%) | 0.060 # | 0.265 |
| Chronic kidney disease | 37 (24.5%) | 145 (13.4%) | <0.001 | 0.287 | 34 (23.1%) | 21 (14.3%) | 0.052 | 0.228 |
| Malignancy | 20 (13.2%) | 63 (5.8%) | 0.001 | 0.255 | 20 (13.6%) | 13 (8.8%) | 0.196 | 0.151 |
| Atrial fibrillation | 69 (45.7%) | 371 (34.2%) | 0.006 | 0.236 | 66 (44.9%) | 60 (40.8%) | 0.480 | 0.083 |
| Laboratory Parameters | ||||||||
| WBC (109/L) | 9.0 ± 5.5 | 10.4 ± 4.4 | <0.001 | 0.285 | 8.9 ± 5.5 | 10.8 ± 4.6 | 0.002 | 0.366 |
| Hgb (g/dL) | 12.0 ± 2.5 | 12.5 ± 2.1 | 0.010 | 0.209 | 12.0 ± 2.5 | 12.5 ± 2.2 | 0.106 | 0.190 |
| Platelet (109/L) | 120.2 ± 28.3 | 246.1 ± 87.2 | <0.001 | 1.943 | 119.8 ± 28.4 | 237.2 ± 71.2 | <0.001 | 2.167 |
| Creatinine (mEq/L) | 1.4 ± 1.5 | 1.0 ± 0.8 | <0.001 | 0.305 | 1.4 ± 1.5 | 1.1 ± 0.5 | 0.013 | 0.292 |
| BUN (mg/dL) | 23.2 ± 15.4 | 18.6 ± 11.5 | <0.001 | 0.345 | 23.1 ± 15.5 | 19.8 ± 9.2 | 0.027 | 0.260 |
| Sodium (mmol/L) | 140.0 ± 4.2 | 139.3 ± 3.9 | 0.054 | 0.163 | 140.0 ± 4.2 | 139.4 ± 4.9 | 0.219 | 0.144 |
| Potassium (mmol/L) | 4.1 ± 0.7 | 4.1 ± 0.6 | 0.686 | 0.033 | 4.1 ± 0.7 | 4.0 ± 0.6 | 0.226 | 0.141 |
| Bilirubin (mg/dL) | 0.8 ± 0.6 | 0.6 ± 0.5 | 0.001 | 0.361 | 0.8 ± 0.6 | 0.6 ± 0.5 | 0.039 | 0.338 |
| INR | 1.4 ± 1.2 | 1.2 ± 0.4 | <0.001 | 0.207 | 1.4 ± 1.2 | 1.3 ± 0.4 | 0.216 | 0.157 |
| HAS-BLED score | 3.9 ± 1.0 | 3.7 ± 0.9 | 0.003 | 0.254 | 3.9 ± 1.0 | 3.7 ± 0.9 | 0.051 | 0.229 |
| APS III | 44.8 ± 21.0 | 38.2 ± 19.1 | <0.001 | 0.328 | 43.5 ± 19.8 | 44.5 ± 20.2 | 0.671 | 0.050 |
| ICU mortality, n | 16 (10.6%) | 81 (7.5%) | 0.180 | 0.109 | 14 (9.5%) | 14 (9.5%) | 1.000 | <0.001 |
| ICU length of stay, day | 5.0 ± 5.3 | 4.1 ± 4.9 | 0.035 | 0.179 | 4.9 ± 5.3 | 4.0 ± 4.7 | 0.159 | 0.165 |
| In-hospital mortality, n | 27 (17.9%) | 136 (12.5%) | 0.069 | 0.149 | 25 (17.0%) | 22 (15.0%) | 0.633 | 0.056 |
| Hospital length of stay, day | 8.9 ± 9.4 | 7.8 ± 9.2 | 0.169 | 0.118 | 8.6 ± 8.3 | 8.1 ± 9.1 | 0.635 | 0.055 |
| Intracranial hemorrhage, n | 17 (11.3%) | 105 (9.7%) | 0.542 | 0.052 | 14 (9.5%) | 13 (8.8%) | 0.840 | 0.024 |
| PEG/PEJ tube placement, n | 15 (9.9%) | 122 (11.2%) | 0.631 | 0.043 | 14 (9.5%) | 19 (12.9%) | 0.356 | 0.108 |
| With Thrombocytopenia Versus without Thrombocytopenia | ||||
|---|---|---|---|---|
| Before PSM−Univariate | After PSM−Univariate | |||
| Outcomes | Crude HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value |
| ICU Mortality | 1.26 (0.60–2.61) | 0.540 | 0.83 (0.40–1.75) | 0.629 |
| In-hospital Mortality | 1.20 (0.69–2.10) | 0.521 | 1.06 (0.60–1.88) | 0.845 |
| Outcomes | Crude OR (95% CI) | p value | Adjusted OR (95% CI) | p value |
| Intracerebral Hemorrhage | 1.08 (0.55–2.12) | 0.833 | 1.09 (0.49–2.40) | 0.840 |
| PEG/PEJ tube placement | 0.64 (0.30–1.37) | 0.250 | 0.71 (0.34–1.47) | 0.357 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-R.; Yang, L.-Y.; Lee, C.-H.; Chang, S.-H.; Chen, P.-H.; Jhou, H.-J. Is Thrombocytopenia an In-Hospital Mortality Risk Factor among Patients with Acute Ischemic Stroke? A Propensity Score-Matched Analysis from the MIMIC-IV Database. J. Clin. Med. 2023, 12, 580. https://doi.org/10.3390/jcm12020580
Wang Y-R, Yang L-Y, Lee C-H, Chang S-H, Chen P-H, Jhou H-J. Is Thrombocytopenia an In-Hospital Mortality Risk Factor among Patients with Acute Ischemic Stroke? A Propensity Score-Matched Analysis from the MIMIC-IV Database. Journal of Clinical Medicine. 2023; 12(2):580. https://doi.org/10.3390/jcm12020580
Chicago/Turabian StyleWang, Yan-Ru, Li-Yu Yang, Cho-Hao Lee, Shu-Hao Chang, Po-Huang Chen, and Hong-Jie Jhou. 2023. "Is Thrombocytopenia an In-Hospital Mortality Risk Factor among Patients with Acute Ischemic Stroke? A Propensity Score-Matched Analysis from the MIMIC-IV Database" Journal of Clinical Medicine 12, no. 2: 580. https://doi.org/10.3390/jcm12020580