

Soluble Vascular Cell Adhesion Molecule-1 as an Inflammation-Related Biomarker of Coronary Slow Flow
 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Coronary Angiography and TFC
2.3. Seattle Angina Questionnaire (SAQ)
2.4. Echocardiography
2.5. Detection of sVCAM-1, IL-6, and TNF-α
2.6. Statistical Analysis
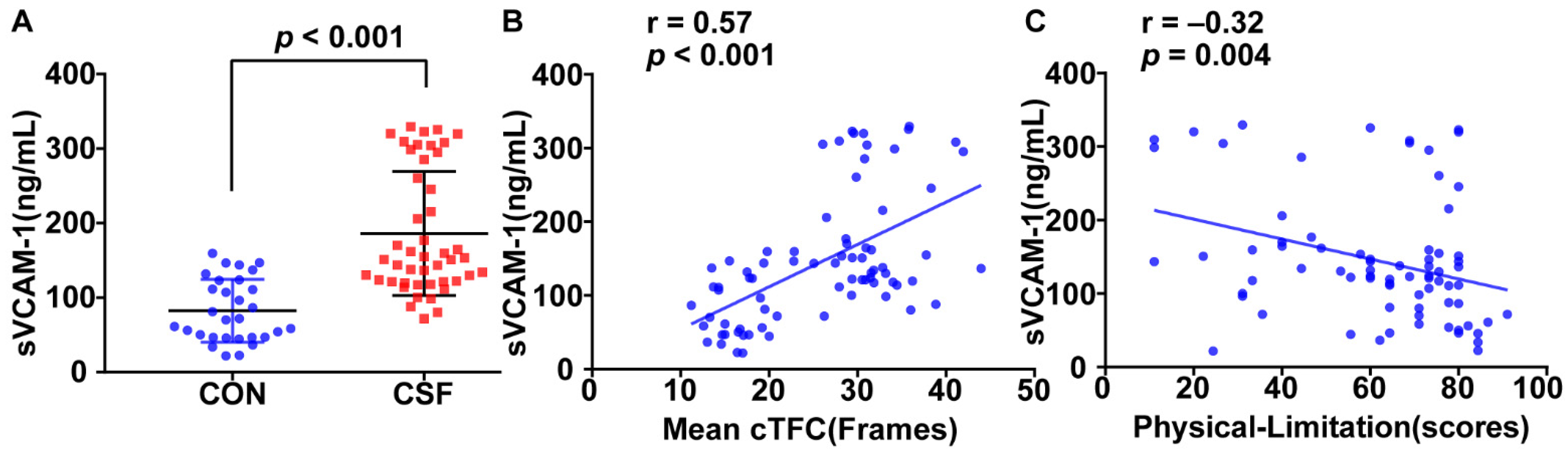
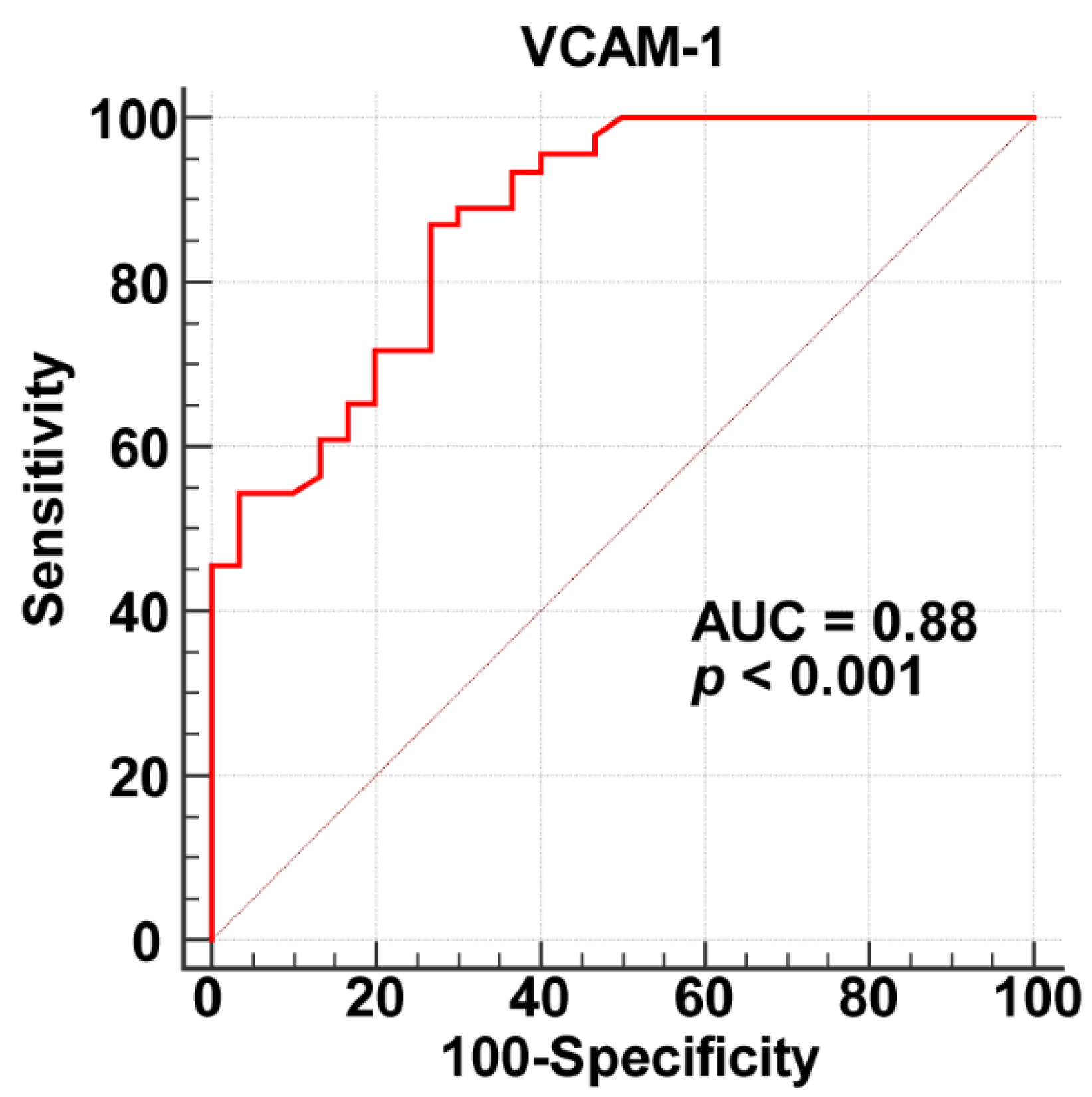
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tambe, A.A.; Demany, M.A.; Zimmerman, H.A.; Mascarenhas, E. Angina pectoris and slow flow velocity of dye in coronary arteries—A new angiographic finding. Am. Heart J. 1972, 84, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, Y.; Li, J.; Li, G.; Kong, F.; Mu, L.; Jia, D.; Li, Y.; Yang, J.; Ma, C. Incremental Value of Three-dimensional Speckle-tracking Echocardiography for Evaluating Left Ventricular Systolic Function in Patients with Coronary Slow Flow. Curr. Probl. Cardiol. 2021, 47, 100928. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ma, C.; Zhang, Y.; Guan, Z.; Liu, S.; Li, Y.; Yang, J. Assessment of left and right ventricular diastolic and systolic functions using two-dimensional speckle-tracking echocardiography in patients with coronary slow-flow phenomenon. PLoS ONE 2015, 10, e0117979. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Zong, Z.; Zhu, Q.; Wang, Y.; Li, X.; Zhang, C.; Ma, C.; Xue, Y. The lncRNA MALAT1 participates in regulating coronary slow flow endothelial dysfunction through the miR-181b-5p-MEF2A-ET-1 axis. Vascul. Pharmacol. 2021, 138, 106841. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Wang, S.; Huang, X.; Zhao, C.; Wang, Y.; Li, X.; Jia, D.; Ma, C. Understanding the pathogenesis of coronary slow flow: Recent advances. Trends Cardiovasc. Med. 2022, S1050-1738(22)00142-6, Epub ahead of print. [Google Scholar] [CrossRef]
- Chalikias, G.; Tziakas, D. Slow Coronary Flow: Pathophysiology, Clinical Implications, and Therapeutic Management. Angiology 2021, 72, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Zhao, C.; Wang, Y.; Li, X.; Xue, Y.; Ma, C. LncRNA NEAT1 Promote Inflammatory Responses in Coronary Slow Flow Through Regulating miR-148b-3p/ICAM-1 Axis. J. Inflamm. Res. 2021, 14, 2445–2463. [Google Scholar] [CrossRef]
- Roshanravan, N.; Shabestari, A.N.; Alamdari, N.M.; Ostadrahimi, A.; Separham, A.; Parvizi, R.; Jafarabadi, M.A.; Ghodrat, M.; Akbarzadeh, M.; Naemi, M.; et al. A novel inflammatory signaling pathway in patients with slow coronary flow: NF-kappaB/IL-1beta/nitric oxide. Cytokine 2021, 143, 155511. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, Y.; Huang, Z.; Wu, F.; Li, N.; Liang, C. Association between impaired cutaneous microvascular endothelial function and lectin-like oxidized low-density lipoprotein receptor-1 in patients with coronary slow flow. Microvasc. Res. 2020, 129, 103984. [Google Scholar] [CrossRef]
- Niu, H.; Wei, Z.; Zhang, Y.; He, J.; Jia, D. Atorvastatin improves coronary flow and endothelial function in patients with coronary slow flow. Exp. Ther. Med. 2018, 15, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Kayapinar, O.; Ozde, C.; Kaya, A. Relationship Between the Reciprocal Change in Inflammation-Related Biomarkers (Fibrinogen-to-Albumin and hsCRP-to-Albumin Ratios) and the Presence and Severity of Coronary Slow Flow. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619835383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willeit, K.; Pechlaner, R.; Willeit, P.; Skroblin, P.; Paulweber, B.; Schernthaner, C.; Toell, T.; Egger, G.; Weger, S.; Oberhollenzer, M.; et al. Association Between Vascular Cell Adhesion Molecule 1 and Atrial Fibrillation. JAMA Cardiol. 2017, 2, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Moccetti, F.; Brown, E.; Xie, A.; Packwood, W.; Qi, Y.; Ruggeri, Z.; Shentu, W.; Chen, J.; Lopez, J.A.; Lindner, J.R. Myocardial Infarction Produces Sustained Proinflammatory Endothelial Activation in Remote Arteries. J. Am. Coll Cardiol. 2018, 72, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Arends, C.M.; Liman, T.G.; Strzelecka, P.M.; Kufner, A.; Lowe, P.; Huo, S.; Stein, C.M.; Piper, S.K.; Tilgner, M.; Sperber, P.S.; et al. Associations of clonal haematopoiesis with recurrent vascular events and death in patients with incident ischemic stroke. Blood 2022, 2022017661, Epub ahead of print. [Google Scholar] [CrossRef]
- Chyrchel, B.; Kruszelnicka, O.; Surdacki, A. Endothelial biomarkers and platelet reactivity on ticagrelor versus clopidogrel in patients after acute coronary syndrome with and without concomitant type 2 diabetes: A preliminary observational study. Cardiovasc. Diabetol. 2022, 21, 249. [Google Scholar] [CrossRef]
- Gibson, C.M.; Cannon, C.P.; Daley, W.L.; Dodge, J.T., Jr.; Alexander, B., Jr.; Marble, S.J.; McCabe, C.H.; Raymond, L.; Fortin, T.; Poole, W.K.; et al. TIMI frame count: A quantitative method of assessing coronary artery flow. Circulation 1996, 93, 879–888. [Google Scholar] [CrossRef]
- Yao, G.H.; Deng, Y.; Liu, Y.; Xu, M.J.; Zhang, C.; Deng, Y.B.; Ren, W.D.; Li, Z.A.; Tang, H.; Zhang, Q.B.; et al. Echocardiographic measurements in normal chinese adults focusing on cardiac chambers and great arteries: A prospective, nationwide, and multicenter study. J. Am. Soc. Echocardiogr. 2015, 28, 570–579. [Google Scholar] [CrossRef]
- Wang, Y.H.; Kang, Y.Q.; Jin, X.Y.; Meng, P.P.; Guan, Z.Y.; Jia, D.L.; Gao, M.Y.; Ma, C.Y. Reference values of the carotid elastic modulus using shear wave elastography and arterial stiffness change in coronary slow flow. Eur. J. Radiol. 2022, 157, 110582. [Google Scholar] [CrossRef]
- Li, M.; Su, H.; Jiang, M.; Zuo, Z.; Su, Z.; Hao, L.; Yang, J.; Zhang, Z.; Wang, H.; Kong, X. Predictive value of thrombolysis in myocardial infarction frame count for coronary microvascular dysfunction evaluated with an angiography-derived index of microcirculatory resistance in patients with coronary slow flow. Quant Imaging Med. Surg. 2022, 12, 4942–4952. [Google Scholar] [CrossRef]
- Spertus, J.A.; Winder, J.A.; Dewhurst, T.A.; Deyo, R.A.; Prodzinski, J.; McDonell, M.; Fihn, S.D. Development and evaluation of the Seattle Angina Questionnaire: A new functional status measure for coronary artery disease. J. Am. Coll Cardiol. 1995, 25, 333–341. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Cannon, R.O., 3rd. Microvascular angina and the continuing dilemma of chest pain with normal coronary angiograms. J. Am. Coll Cardiol. 2009, 54, 877–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanar, H.S.; Arsan, A.; Kup, A.; Kanar, B.G.; Tanyildiz, B.; Akaslan, D.; Uslu, A.; Sadic, B.O. Comparison of subfoveal choroidal thickness and retinal nerve fiber layer thickness in patients with coronary slow flow phenomenon and microvascular angina: Optical coherence tomography based study. Photodiagnosis. Photodyn. Ther. 2021, 33, 102189. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zou, R.; Shi, W.; Zhou, N.; Chen, S.; Zhou, H.; Chen, X.; Wu, Y. SGLT2 inhibitor dapagliflozin reduces endothelial dysfunction and microvascular damage during cardiac ischemia/reperfusion injury through normalizing the XO-SERCA2-CaMKII-coffilin pathways. Theranostics 2022, 12, 5034–5050. [Google Scholar] [CrossRef]
- Kozakova, M.; Morizzo, C.; Goncalves, I.; Natali, A.; Nilsson, J.; Palombo, C. Cardiovascular organ damage in type 2 diabetes mellitus: The role of lipids and inflammation. Cardiovasc. Diabetol. 2019, 18, 61. [Google Scholar] [CrossRef] [Green Version]
- Paulus, W.J.; Tschope, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Su, Q.; Yang, H.; Li, L. Circulating miRNA-155 as a Potential Biomarker for Coronary Slow Flow. Dis. Markers 2018, 2018, 6345284. [Google Scholar] [CrossRef]
- Akbar, N.; Braithwaite, A.T.; Corr, E.M.; Koelwyn, G.J.; van Solingen, C.; Cochain, C.; Saliba, A.E.; Corbin, A.; Pezzolla, D.; Moller Jorgensen, M.; et al. Rapid neutrophil mobilisation by VCAM-1+ endothelial extracellular vesicles. Cardiovasc Res. 2022, cvac012, Epub ahead of print. [Google Scholar] [CrossRef]
- Kong, D.H.; Kim, Y.K.; Kim, M.R.; Jang, J.H.; Lee, S. Emerging Roles of Vascular Cell Adhesion Molecule-1 (VCAM-1) in Immunological Disorders and Cancer. Int. J. Mol. Sci. 2018, 19, 1057. [Google Scholar] [CrossRef] [Green Version]
- Troncoso, M.F.; Ortiz-Quintero, J.; Garrido-Moreno, V.; Sanhueza-Olivares, F.; Guerrero-Moncayo, A.; Chiong, M.; Castro, P.F.; Garcia, L.; Gabrielli, L.; Corbalan, R.; et al. VCAM-1 as a predictor biomarker in cardiovascular disease. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166170. [Google Scholar] [CrossRef]
- Llibre, J.M.; Lopez Cortes, L.F.; Aylott, A.; Wynne, B.; Matthews, J.; Van Solingen-Ristea, R.; Vandermeulen, K.; van Wyk, J.; Kahl, L.P. Brief Report: Evaluation of Inflammation and Atherogenesis Biomarkers Through 148 Weeks Postswitch to Dolutegravir and Rilpivirine in SWORD-1/SWORD-2. J. Acquir. Immune. Defic. Syndr. 2022, 91, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Turhan, H.; Saydam, G.S.; Erbay, A.R.; Ayaz, S.; Yasar, A.S.; Aksoy, Y.; Basar, N.; Yetkin, E. Increased plasma soluble adhesion molecules; ICAM-1, VCAM-1, and E-selectin levels in patients with slow coronary flow. Int. J. Cardiol. 2006, 108, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Spertus, J.A.; Arnold, S.V. The Evolution of Patient-Reported Outcomes in Clinical Trials and Management of Patients With Coronary Artery Disease: 20 Years With the Seattle Angina Questionnaire. JAMA Cardiol. 2018, 3, 1035–1036. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CSF (n = 46) | Controls (n = 30) | p Value | |
|---|---|---|---|
| Demographics | |||
| Age (yrs) | 56.11 ± 11.39 | 56.67 ± 8.30 | 0.82 |
| Male (n(%)) | 25 (54.3) | 12(40.0) | 0.22 |
| Body mass index (kg/m2) | 25.63 ± 5.68 | 25.90 ± 3.41 | 0.82 |
| Medical history | |||
| Smoking (n (%)) | 10 (21.7) | 6 (20.0) | 0.86 |
| Hypertension (n (%)) | 20 (43.5) | 9 (30.0) | 0.24 |
| Diabetes mellitus (n (%)) | 5 (10.9) | 3 (10.0) | 0.90 |
| Family history of myocardial infarction | 7 (15.2) | 7 (23.3) | 0.37 |
| Laboratory values | |||
| Triglycerides (mmol/L) | 1.62 ± 0.97 | 1.74 ± 0.75 | 0.57 |
| Total cholesterol (mmol/L) | 4.44 ± 1.00 | 4.73 ± 1.07 | 0.25 |
| LDL cholesterol (mmol/L) | 2.86 ± 0.82 | 3.06 ± 0.94 | 0.33 |
| HDL cholesterol (mmol/L) | 1.09 ± 0.26 | 1.16 ± 0.36 | 0.31 |
| Fasting blood glucose (mmol/L) | 5.58 ± 1.58 | 5.68 ± 1.72 | 0.81 |
| Red blood cell count (1012/L) | 4.61 ± 0.35 | 4.42 ± 0.37 | 0.10 |
| Red cell distribution width (%) | 13.03 ± 0.34 | 12.94 ± 0.29 | 0.24 |
| Platelet count (109/L) | 222.45 ± 38.88 | 220.85 ± 46.87 | 0.33 |
| Platelet distribution width (%) | 11.82 ± 1.37 | 12.09 ± 1.70 | 0.48 |
| Medications | |||
| Aspirin (n (%)) | 10 (21.7) | 6 (20.0) | 0.86 |
| ACEI/ARB (n (%)) | 20 (43.4) | 11 (36.7) | 0.55 |
| β-Blockers (n (%)) | 24 (52.2) | 14 (46.7) | 0.64 |
| Calcium channel blocker (n (%)) | 12 (26.1) | 6 (20.0) | 0.54 |
| Statin (n (%)) | 34 (73.9) | 19 (63.3) | 0.33 |
| Nitrates (n (%)) | 33 (71.7) | 20 (66.7) | 0.64 |
| TFC | |||
| cLAD | 30.61 ± 5.97 | 16.26 ± 4.10 | <0.001 |
| LCX | 40.00 ± 6.97 | 19.63 ± 3.53 | <0.001 |
| RCA | 25.04 ± 8.24 | 13.73 ± 5.01 | <0.001 |
| Mean | 31.89 ± 4.46 | 16.54 ± 2.79 | <0.001 |
| Vessel involved | |||
| 1-vessel (n (%)) | 12 (26.09) | ||
| 2-vessel (n (%)) | 23 (50.00) | ||
| 3-vessel (n (%)) | 11 (23.91) |
| CSF (n = 46) | Controls (n = 30) | p Value | |
|---|---|---|---|
| Physical limitation | 56.76 ± 21.84 | 68.65 ± 16.30 | 0.008 |
| Angina stability | 68.48 ± 33.10 | 68.52 ± 22.57 | 0.99 |
| Angina frequency | 74.57 ± 21.57 | 79.09 ± 19.00 | 0.40 |
| Treatment satisfaction | 75.06 ± 17.80 | 79.96 ± 11.72 | 0.18 |
| Quality of life | 51.45 ± 26.89 | 51.51 ± 17.36 | 0.99 |
| CSF (n = 46) | Controls (n = 30) | p Value | |
|---|---|---|---|
| LV end-diastolic diameter (mm) | 47.20 ± 3.86 | 47.10 ± 3.18 | 0.92 |
| LV end-systolic diameter (mm) | 27.74 ± 3.12 | 26.90 ± 2.63 | 0.27 |
| LV end-diastolic volume (mL) | 87.62 ± 21.50 | 84.00 ± 20.51 | 0.50 |
| LV end-systolic volume (mL) | 31.24 ± 7.64 | 30.75 ± 8.53 | 0.81 |
| LV ejection fraction (%) | 64.16 ± 2.71 | 63.50 ± 2.95 | 0.36 |
| LV GLS (%) | −17.22 ± 2.23 | −18.46 ± 2.37 | 0.04 |
| LA volume index (mL/m2) | 27.91 ± 8.51 | 31.95 ± 10.37 | 0.16 |
| mitral E (cm/s) | 59.76 ± 11.22 | 67.77 ± 13.36 | 0.01 |
| mitral A (cm/s) | 72.51 ± 15.14 | 67.54 ± 13.11 | 0.17 |
| mitral E/A | 0.87 ± 0.31 | 1.05 ± 0.32 | 0.03 |
| mitral e’ (cm/s) | 7.43 ± 2.19 | 7.88 ± 1.91 | 0.41 |
| mitral E/e’ | 8.47 ± 2.52 | 8.42 ± 1.86 | 0.92 |
| TR V (m/s) | 2.30 ± 0.46 | 2.09 ± 0.62 | 0.24 |
| RV basal diameter (mm) | 28.94 ± 4.22 | 28.49 ± 5.38 | 0.71 |
| RV fractional area change (%) | 46.78 ± 6.56 | 48.84 ± 6.37 | 0.18 |
| TAPSE (mm) | 25.03 ± 4.32 | 23.00 ± 4.91 | 0.09 |
| tricuspid E/A | 1.21 ± 0.38 | 1.36 ± 0.32 | 0.10 |
| tricuspid S’ (cm/s) | 11.72 ± 2.43 | 11.29 ± 1.68 | 0.45 |
| tricuspid E/e’ | 6.47 ± 1.69 | 5.95 ± 1.56 | 0.23 |
| Variables | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | |||||
| β [95% CI] | p Value | β [95% CI] | p Value | β [95% CI] | p Value | |
| Physical Limitation | −0.07 [−0.17–0.02] | 0.13 | ||||
| Mitral E | −0.15 [−0.30–0.01] | 0.07 | ||||
| Mitral E/A | −3.23 [−9.53–3.08] | 0.31 | ||||
| TAPSE | 0.44 [0.00–0.88] | 0.05 | ||||
| LV GLS | 0.88 [0.02–1.75] | 0.045 | 0.40 [−0.35–1.15] | 0.29 | −0.06 [−0.85–0.74] | 0.89 |
| IL-6 | 0.06 [0.02–0.10] | 0.002 | −0.05 [−0.11–0.02] | 0.17 | −0.06 [−0.13–0.00] | 0.06 |
| TNF-α | 3.20 [0.27–6.13] | 0.03 | −2.73 [−6.50–1.04] | 0.15 | −2.97 [−6.79–0.86] | 0.13 |
| sVCAM-1 | 0.06 [0.04–0.07] | <0.001 | 0.08 [0.05–0.11] | <0.001 | 0.09 [0.06–0.12] | <0.001 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR [95% CI] | p Value | OR [95% CI] | p Value | OR [95% CI] | p Value | |
| Age | 0.99 [0.93–1.04] | 0.58 | 0.93 [0.86–1.01] | 0.10 | 0.94 [0.79–1.11] | 0.48 |
| Sex | 0.29 [0.09–0.90] | 0.03 | 0.34 [0.07–1.78] | 0.20 | 0.84 [0.04–19.64] | 0.91 |
| BMI | 0.99 [0.89–1.09] | 0.79 | 1.02 [0.90–1.16] | 0.79 | 1.11 [0.93–1.32] | 0.26 |
| Physical Limitation | 0.95 [0.92–0.98] | 0.003 | 0.94 [0.90–0.98] | 0.003 | 0.95 [0.88–1.02] | 0.16 |
| Mitral E | 0.93 [0.86–1.01] | 0.09 | 0.95 [0.83–1.09] | 0.46 | ||
| Mitral E/A | 0.36 [0.01–10.35] | 0.55 | 0.13 [0.00–76.76] | 0.53 | ||
| TAPSE | 1.16 [0.97–1.40] | 0.11 | 1.37 [0.96–1.96] | 0.08 | ||
| LV GLS | 1.17 [0.84–1.61] | 0.35 | 1.24 [0.73–2.10] | 0.43 | ||
| IL-6 | 0.95 [0.90–1.01] | 0.10 | ||||
| TNF-α | 0.41 [0.01–12.44] | 0.61 | ||||
| sVCAM-1 | 1.07 [1.03–1.11] | 0.001 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Q.; Zhao, C.; Wang, Y.; Mu, L.; Li, X.; Qi, Y.; Yang, J.; Ma, C. Soluble Vascular Cell Adhesion Molecule-1 as an Inflammation-Related Biomarker of Coronary Slow Flow. J. Clin. Med. 2023, 12, 543. https://doi.org/10.3390/jcm12020543
Zhu Q, Zhao C, Wang Y, Mu L, Li X, Qi Y, Yang J, Ma C. Soluble Vascular Cell Adhesion Molecule-1 as an Inflammation-Related Biomarker of Coronary Slow Flow. Journal of Clinical Medicine. 2023; 12(2):543. https://doi.org/10.3390/jcm12020543
Chicago/Turabian StyleZhu, Qing, Cuiting Zhao, Yonghuai Wang, Lixin Mu, Xinxin Li, Yiqiu Qi, Jun Yang, and Chunyan Ma. 2023. "Soluble Vascular Cell Adhesion Molecule-1 as an Inflammation-Related Biomarker of Coronary Slow Flow" Journal of Clinical Medicine 12, no. 2: 543. https://doi.org/10.3390/jcm12020543