
Does Surgical Resection Significantly Prolong the Long-Term Survival of Patients with Oligometastatic Pancreatic Ductal Adenocarcinoma? A Cross-Sectional Study Based on 18 Registries

Abstract
:1. Background
2. Methods
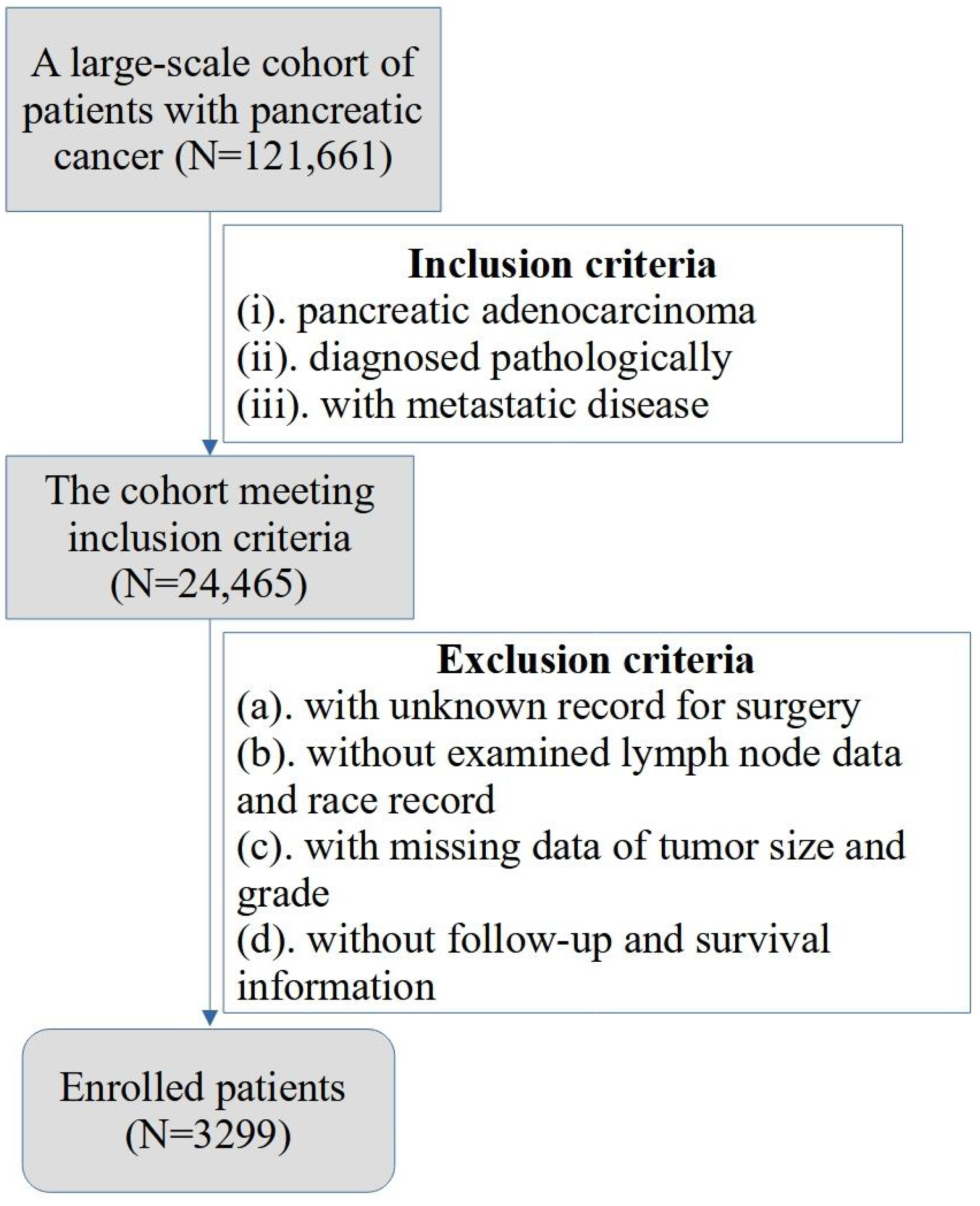
2.1. Patients and Study Design
2.2. Covariates and Outcomes
2.3. Statistical Analysis
3. Results
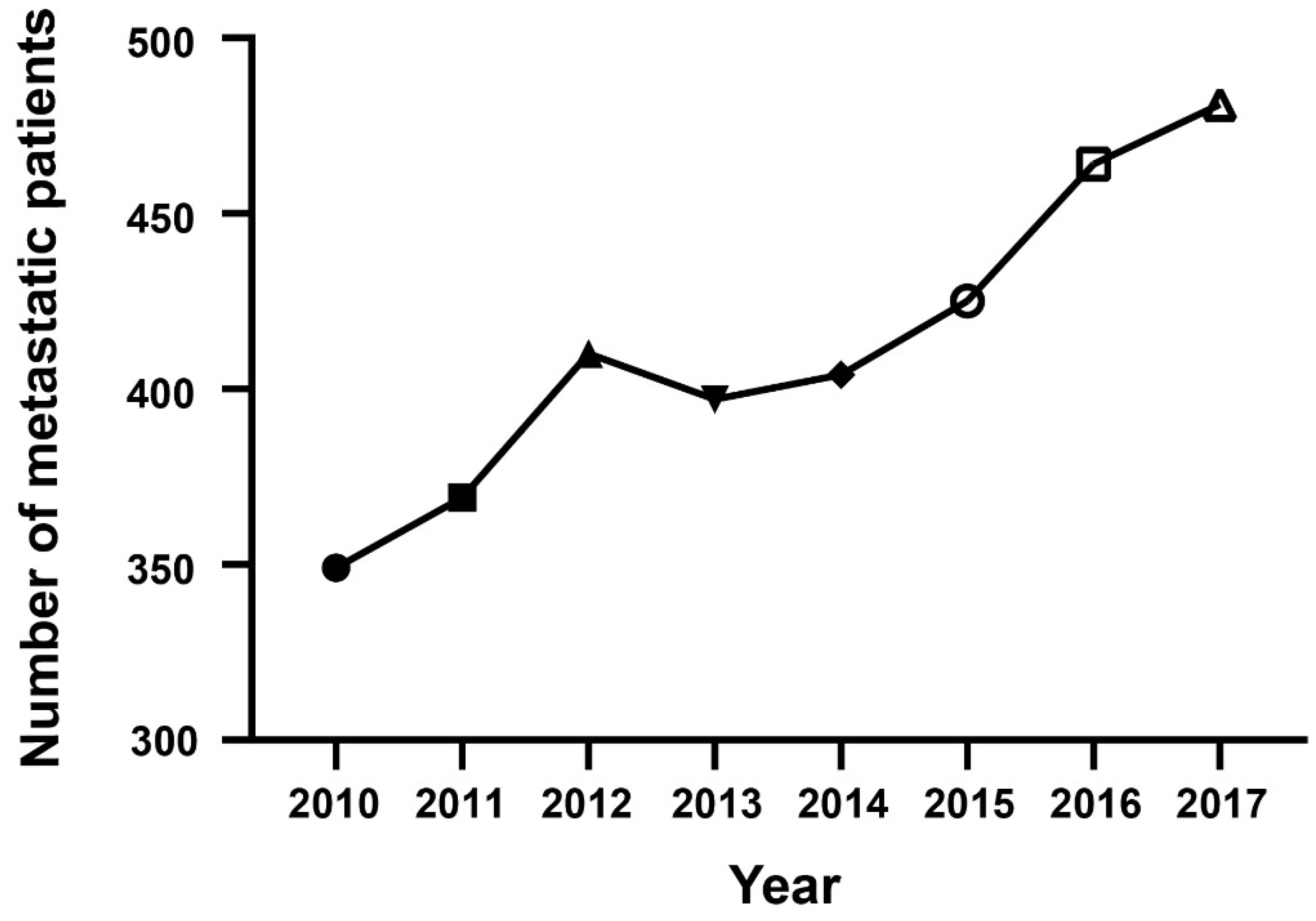
3.1. Epidemiological Trend of mPDAC Patient Number
3.2. Baseline Characteristics
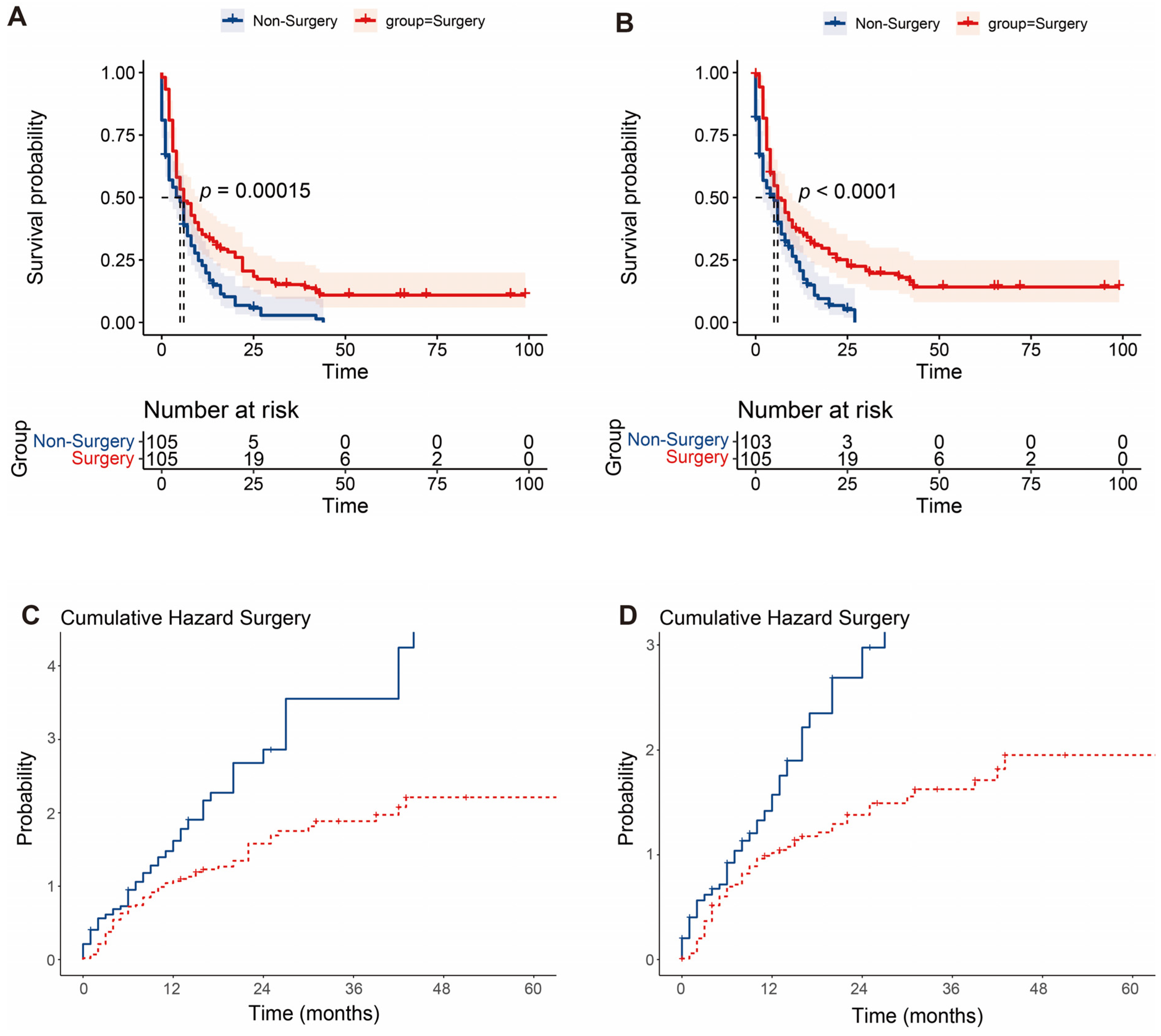
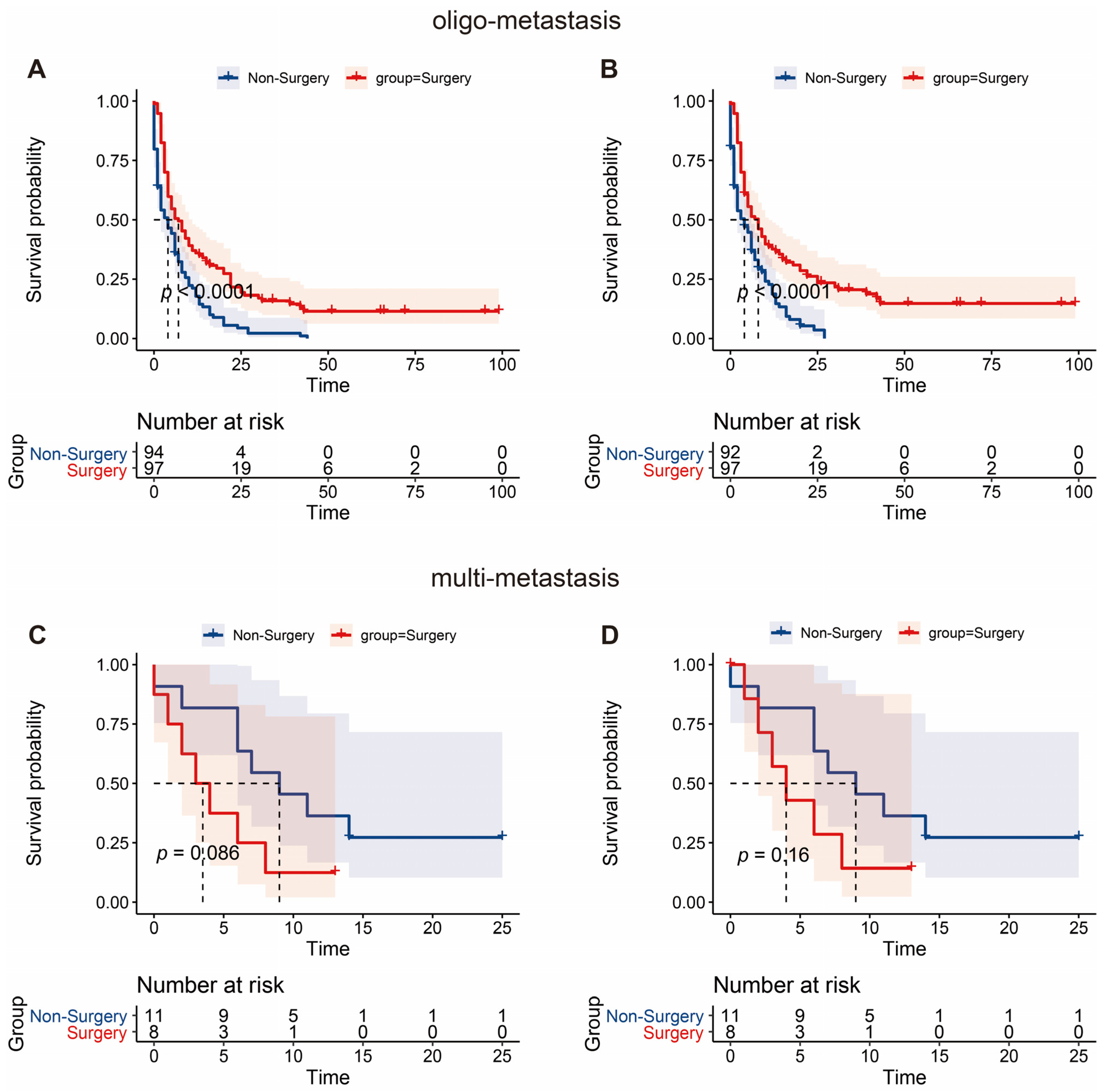
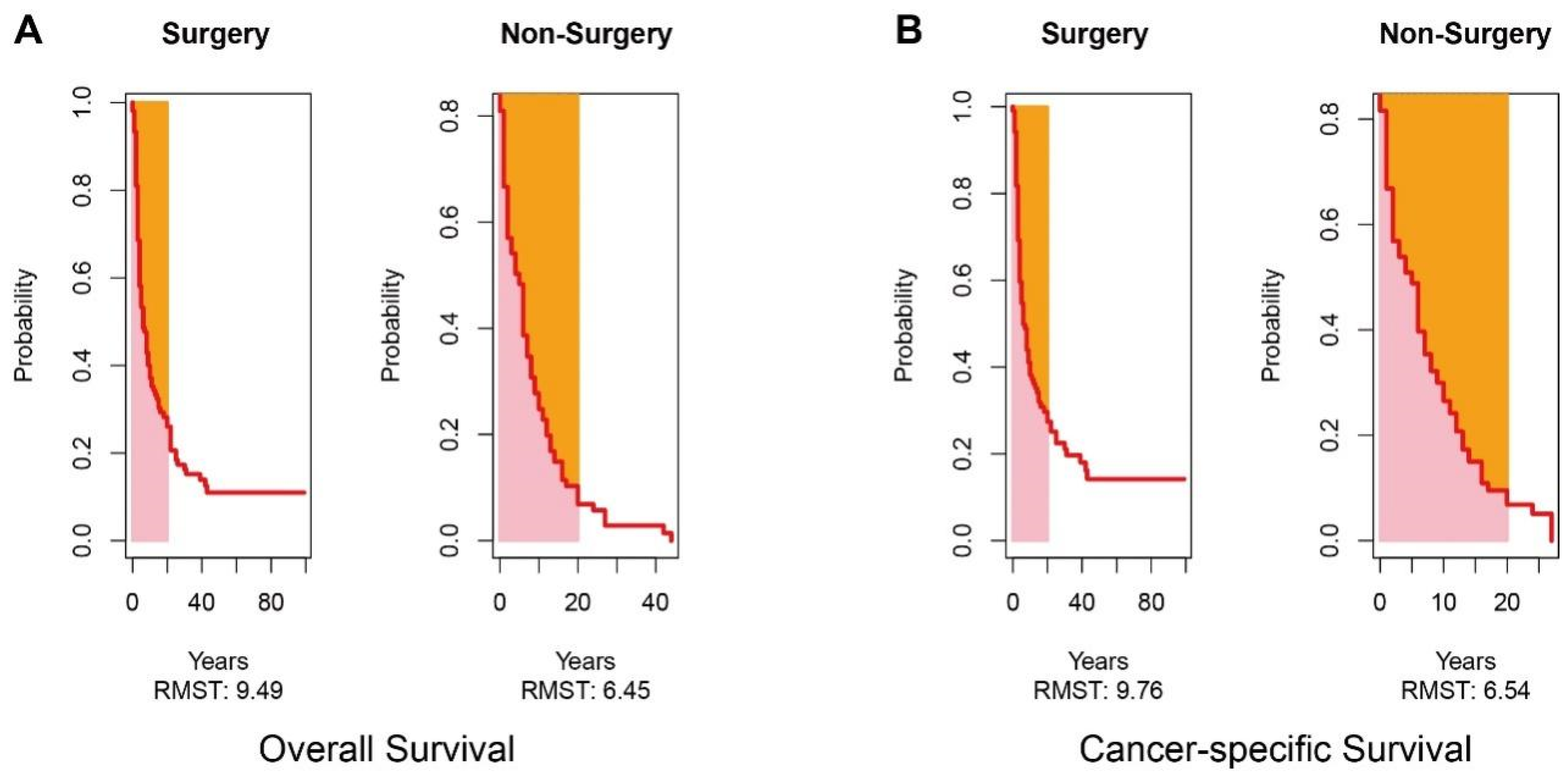
3.3. Long-Term Survival Analysis
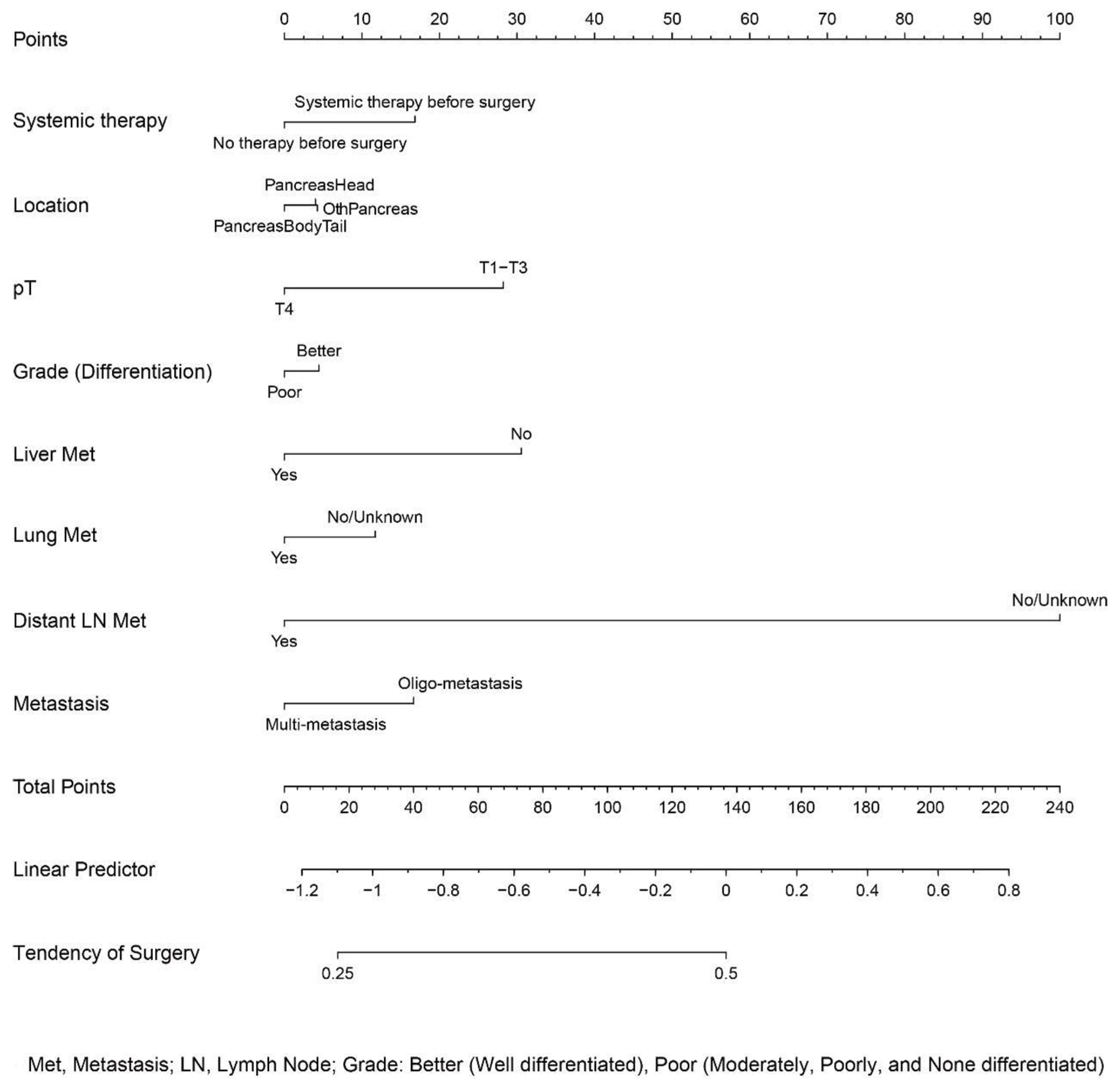
3.4. Development of a Nomogram Predicting Surgery
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheema, A.R.; O’Reilly, E.M. Management of Metastatic Pancreatic Adenocarcinoma. Surg. Clin. N. Am. 2016, 96, 1391–1414. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Li, D.; Xie, K.; Wolff, R.; Abbruzzese, J.L. Pancreatic cancer. Lancet 2004, 363, 1049–1057. [Google Scholar] [CrossRef]
- Brachi, G.; Bussolino, F.; Ciardelli, G.; Mattu, C. Nanomedicine for Imaging and Therapy of Pancreatic Adenocarcinoma. Front. Bioeng. Biotechnol. 2019, 7, 307. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Asbun, H.; Bain, A.; Behrman, S.W.; Benson, A.B., III; Binder, E.; Cardin, D.B.; Cha, C.; et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 1028–1061. [Google Scholar] [CrossRef] [Green Version]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. S5), v56–v68. [Google Scholar] [CrossRef]
- Tol, J.A.; Gouma, D.J.; Bassi, C.; Dervenis, C.; Montorsi, M.; Adham, M.; Andrén-Sandberg, A.; Asbun, H.J.; Bockhorn, M.; Büchler, M.W.; et al. Definition of a standard lymphadenectomy in surgery for pancreatic ductal adenocarcinoma: A consensus statement by the International Study Group on Pancreatic Surgery (ISGPS). Surgery 2014, 156, 591–600. [Google Scholar] [CrossRef]
- Vohra, N.A.; Brinkley, J.; Kachare, S.; Muzaffar, M. Primary tumor resection in metastatic breast cancer: A propensity-matched analysis, 1988–2011 SEER data base. Breast J. 2018, 24, 549–554. [Google Scholar] [CrossRef]
- Warschkow, R.; Güller, U.; Tarantino, I.; Cerny, T.; Schmied, B.M.; Thuerlimann, B.; Joerger, M. Improved Survival After Primary Tumor Surgery in Metastatic Breast Cancer: A Propensity-adjusted, Population-based SEER Trend Analysis. Ann. Surg. 2016, 263, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Coffey, M.R.; Bachman, K.C.; Worrell, S.G.; Argote-Greene, L.M.; Linden, P.A.; Towe, C.W. Palliative Surgery Outcomes for Patients with Esophageal Cancer: An National Cancer Database Analysis. J. Surg. Res. 2021, 267, 229–234. [Google Scholar] [CrossRef]
- Rosen, S.A.; Buell, J.F.; Yoshida, A.; Kazsuba, S.; Hurst, R.; Michelassi, F.; Millis, J.M.; Posner, M.C. Initial presentation with stage IV colorectal cancer: How aggressive should we be? Arch. Surg. 2000, 135, 530–534. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Xu, Z.; Ma, Y.; Chen, H.; Wang, D.; Deng, X.; Cheng, D.; Xie, J.; Jin, J.; Zhan, X.; et al. Surgical resection of metastatic pancreatic cancer: Is it worth it?—A 15-year experience at a single Chinese center. J. Gastrointest. Oncol. 2020, 11, 319–328. [Google Scholar] [CrossRef]
- Hamad, A.; Underhill, J.; Ansari, A.; Thayaparan, V.; Cloyd, J.M.; Li, Y.; Pawlik, T.M.; Tsung, A.; Abushahin, L.; Ejaz, A. Surgical treatment of hepatic oligometastatic pancreatic ductal adenocarcinoma: An analysis of the National Cancer Database. Surgery 2022, 171, 1464–1470. [Google Scholar] [CrossRef]
- Su, B.-B.; Bai, D.-S.; Yu, J.-Q.; Zhang, C.; Jin, S.-J.; Zhou, B.-H.; Jiang, G.-Q. Can Patients with Pancreatic Cancer and Liver Metastases Obtain Survival Benefit from Surgery? A Population-Based Study. J. Cancer 2021, 12, 539–552. [Google Scholar] [CrossRef]
- Tao, L.; Xiu, D.; Sadula, A.; Ye, C.; Chen, Q.; Wang, H.; Zhang, Z.; Zhang, L.; Tao, M.; Yuan, C. Surgical resection of primary tumor improves survival of pancreatic neuroendocrine tumor with liver metastases. Oncotarget 2017, 8, 79785–79792. [Google Scholar] [CrossRef] [Green Version]
- Gleisner, A.L.; Assumpcao, L.; Cameron, J.L.; Wolfgang, C.L.; Choti, M.A.; Herman, J.M.; Schulick, R.D.; Pawlik, T.M. Is resection of periampullary or pancreatic adenocarcinoma with synchronous hepatic metastasis justified? Cancer 2007, 110, 2484–2492. [Google Scholar] [CrossRef]
- Ettrich, T.J.; Seufferlein, T. Systemic Therapy for Metastatic Pancreatic Cancer. Curr. Treat. Options Oncol. 2021, 22, 106. [Google Scholar] [CrossRef]
- Philip, P.A.; Benedetti, J.; Corless, C.L.; Wong, R.; O’Reilly, E.M.; Flynn, P.J.; Rowland, K.M.; Atkins, J.N.; Mirtsching, B.C.; Rivkin, S.E.; et al. Phase III Study Comparing Gemcitabine Plus Cetuximab versus Gemcitabine in Patients with Advanced Pancreatic Adenocarcinoma: Southwest Oncology Group–Directed Intergroup Trial S0205. J. Clin. Oncol. 2010, 28, 3605–3610. [Google Scholar] [CrossRef] [Green Version]
- Kindler, H.L.; Niedzwiecki, D.; Hollis, D.; Sutherland, S.; Schrag, D.; Hurwitz, H.; Innocenti, F.; Mulcahy, M.F.; O’Reilly, E.; Wozniak, T.F.; et al. Gemcitabine Plus Bevacizumab Compared with Gemcitabine Plus Placebo in Patients with Advanced Pancreatic Cancer: Phase III Trial of the Cancer and Leukemia Group B (CALGB 80303). J. Clin. Oncol. 2010, 28, 3617–3622. [Google Scholar] [CrossRef] [Green Version]
- Kindler, H.L.; Ioka, T.; Richel, D.J.; Bennouna, J.; Létourneau, R.; Okusaka, T.; Funakoshi, A.; Furuse, J.; Park, Y.S.; Ohkawa, S.; et al. Axitinib plus gemcitabine versus placebo plus gemcitabine in patients with advanced pancreatic adenocarcinoma: A double-blind randomised phase 3 study. Lancet Oncol. 2011, 12, 256–262. [Google Scholar] [CrossRef]
- Feng, F.; Cai, W.; Wang, G.; Chen, W.; Yang, H.; Sun, M.; Zhou, L. Metastatic pancreatic adenocarcinomas could be classified into M1a and M1b category by the number of metastatic organs. BMC Gastroenterol. 2020, 20, 289. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, S.C.; Song, K.B.; Kim, J.; Kang, D.R.; Lee, J.H.; Park, K.-M.; Lee, Y.-J. Improved survival after palliative resection of unsuspected stage IV pancreatic ductal adenocarcinoma. HPB 2016, 18, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zhang, J.; Lui, W.; Huo, Y.; Fu, X.; Yang, M.; Hua, R.; Wang, L.; Sun, Y. Patients with hepatic oligometastatic pancreatic body/tail ductal adenocarcinoma may benefit from synchronous resection. HPB 2020, 22, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Büschenfelde, C.M.Z.; Friess, H.; Kleeff, J. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [Green Version]
- Christodoulidis, G.; Magouliotis, E.; Samara, A.A.; Floros, T.; Zotos, P.A.; Tolia, M.; Zacharoulis, D. The surgical challenge of oligometastatic pancreatic cancer: A systemic review of the literature. J. Balk. Union Oncol. 2021, 26, 1742–1746. [Google Scholar]
- Shao, Y.; Feng, J.; Hu, Z.; Wu, J.; Zhang, M.; Shen, Y.; Zheng, S. Feasibility of pancreaticoduodenectomy with synchronous liver metastasectomy for oligometastatic pancreatic ductal adenocarcinoma—A case-control study. Ann. Med. Surg. 2020, 62, 490–494. [Google Scholar] [CrossRef]
- Seelig, S.K.; Burkert, B.; Chromik, A.M.; Tannapfel, A.; Uhl, W.; Seelig, M.H. Pancreatic Resections for Advanced M1-Pancreatic Carcinoma: The Value of Synchronous Metastasectomy. HPB Surg. 2010, 2010, 579672. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Raw Data of mPDAC Patients | Data after Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| Non-Surgery (n = 3094) | Surgery (n = 205) | p-Value | Non-surgery (n = 105) | Surgery (n = 105) | p-Value | |
| Sex, n (%) | ||||||
| Female | 1383 (44.7%) | 96 (46.8%) | 0.838 | 52 (49.5%) | 48 (45.7%) | 0.858 |
| Male | 1711 (55.3%) | 109 (53.2%) | 53 (50.5%) | 57 (54.3%) | ||
| Age, n (%) | ||||||
| <65 | 1216 (39.3%) | 80 (39.0%) | 0.065 | 44 (41.9%) | 41 (39.0%) | 0.974 |
| ≥85 | 190 (6.1%) | 1 (0.5%) | 32 (30.5%) | 35 (33.3%) | ||
| 65–74 | 992 (32.1%) | 74 (36.1%) | 29 (27.6%) | 28 (26.7%) | ||
| 75–84 | 696 (22.5%) | 50 (24.4%) | 0 (0%) | 1 (1.0%) | ||
| Race, n (%) | ||||||
| Black | 401 (13.0%) | 17 (8.3%) | 0.436 | 9 (8.6%) | 12 (11.4%) | 0.789 |
| Other (American Indian/AK Native, Asian/Pacific Islander) | 260 (8.4%) | 18 (8.8%) | 6 (5.7%) | 10 (9.5%) | ||
| White | 2433 (78.6%) | 170 (82.9%) | 90 (85.7%) | 83 (79.0%) | ||
| Location, n (%) | ||||||
| OthPancreas | 663 (21.4%) | 25 (12.2%) | <0.001 | 18 (17.1%) | 18 (17.1%) | 1 |
| PancreasBodyTail | 1228 (39.7%) | 65 (31.7%) | 25 (23.8%) | 25 (23.8%) | ||
| PancreasHead | 1203 (38.9%) | 115 (56.1%) | 62 (59.0%) | 62 (59.0%) | ||
| Grade, n (%) | ||||||
| Moderately differentiated; Grade II | 1243 (40.2%) | 71 (34.6%) | 0.634 | 43 (41.0%) | 38 (36.2%) | 0.997 |
| Poorly differentiated; Grade III | 1617 (52.3%) | 122 (59.5%) | 54 (51.4%) | 59 (56.2%) | ||
| Undifferentiated; anaplastic; Grade IV | 52 (1.7%) | 2 (1.0%) | 2 (1.9%) | 2 (1.9%) | ||
| Well differentiated; Grade I | 182 (5.9%) | 10 (4.9%) | 6 (5.7%) | 6 (5.7%) | ||
| AJCC 8th pT, n (%) | ||||||
| T1 | 50 (1.6%) | 4 (2.0%) | 0.802 | 1 (1.0%) | 1 (1.0%) | 0.975 |
| T2 | 299 (9.7%) | 27 (13.2%) | 13 (12.4%) | 12 (11.4%) | ||
| T3 | 315 (10.2%) | 22 (10.7%) | 5 (4.8%) | 9 (8.6%) | ||
| T4 | 2430 (78.5%) | 152 (74.1%) | 86 (81.9%) | 83 (79.0%) | ||
| Radiotherapy, n (%) | ||||||
| None/unknown | 2936 (94.9%) | 189 (92.2%) | 0.246 | 102 (97.1%) | 98 (93.3%) | 0.432 |
| Yes | 158 (5.1%) | 16 (7.8%) | 3 (2.9%) | 7 (6.7%) | ||
| Chemotherapy, n (%) | ||||||
| No/unknown | 1306 (42.2%) | 60 (29.3%) | 0.001 | 59 (56.2%) | 58 (55.2%) | 0.99 |
| Yes | 1788 (57.8%) | 145 (70.7%) | 46 (43.8%) | 47 (44.8%) | ||
| Systemic therapy, n (%) | ||||||
| No systemic therapy | 3023 (97.7%) | 60 (29.3%) | <0.001 | 59 (56.2%) | 58 (55.2%) | 0.999 |
| Systemic therapy after surgery | 54 (1.7%) | 119 (58.0%) | 37 (35.2%) | 36 (34.3%) | ||
| Systemic therapy before surgery | 12 (0.4%) | 14 (6.8%) | 6 (5.7%) | 8 (7.6%) | ||
| Systemic therapy both before and after surgery | 5 (0.2%) | 12 (5.9%) | 3 (2.9%) | 3 (2.9%) | ||
| Bone metastasis, n (%) | ||||||
| NA | 77 (2.5%) | 5 (2.4%) | 0.997 | 2 (1.9%) | 3 (2.9%) | 0.987 |
| No | 2847 (92.0%) | 190 (92.7%) | 99 (94.3%) | 99 (94.3%) | ||
| Yes | 170 (5.5%) | 10 (4.9%) | 4 (3.8%) | 3 (2.9%) | ||
| Brain metastasis, n (%) | ||||||
| NA | 74 (2.4%) | 5 (2.4%) | 0.856 | 2 (1.9%) | 3 (2.9%) | 0.903 |
| No | 3000 (97.0%) | 200 (97.6%) | 103 (98.1%) | 102 (97.1%) | ||
| Yes | 20 (0.6%) | 0 (0%) | ||||
| Liver metastasis, n (%) | ||||||
| NA | 14 (0.5%) | 0 (0%) | 0.002 | 16 (15.2%) | 18 (17.1%) | 0.932 |
| No | 387 (12.5%) | 46 (22.4%) | 89 (84.8%) | 87 (82.9%) | ||
| Yes | 2693 (87.0%) | 159 (77.6%) | ||||
| Lung metastasis, n (%) | ||||||
| NA | 86 (2.8%) | 3 (1.5%) | 0.036 | 2 (1.9%) | 2 (1.9%) | 1 |
| No | 2319 (75.0%) | 174 (84.9%) | 90 (85.7%) | 91 (86.7%) | ||
| Yes | 689 (22.3%) | 28 (13.7%) | 13 (12.4%) | 12 (11.4%) | ||
| Distant lymph node metastasis, n (%) | ||||||
| NA | 2224 (71.9%) | 142 (69.3%) | 0.731 | 84 (80.0%) | 78 (74.3%) | 0.509 |
| No | 761 (24.6%) | 52 (25.4%) | 15 (14.3%) | 24 (22.9%) | ||
| Yes | 109 (3.5%) | 11 (5.4%) | 6 (5.7%) | 3 (2.9%) | ||
| Other metastasis, n (%) | ||||||
| NA | 2227 (72.0%) | 142 (69.3%) | 0.236 | 84 (80.0%) | 78 (74.3%) | 0.83 |
| No | 678 (21.9%) | 42 (20.5%) | 16 (15.2%) | 18 (17.1%) | ||
| Yes | 189 (6.1%) | 21 (10.2%) | 5 (4.8%) | 9 (8.6%) | ||
| Metastasis, n (%) | ||||||
| Multi-metastasis | 644 (20.8%) | 22 (10.7%) | 0.002 | 11 (10.5%) | 8 (7.6%) | 0.771 |
| Oligo-metastasis | 2450 (79.2%) | 183 (89.3%) | 94 (89.5%) | 97 (92.4%) | ||
| Number of regional nodes examined | ||||||
| Mean (SD) | NA | 14.7 (12.4) | NA | 14.3 (12.0) | ||
| Median [min, max] | NA | 13.0 [0, 84.0] | NA | 13.0 [0, 68.0] | ||
| Number of regional nodes positive | ||||||
| Mean (SD) | NA | 3.21 (4.26) | NA | 3.10 (3.71) | ||
| Median [min, max] | NA | 2.00 [0, 20.0] | NA | 2.00 [0, 14.0] | ||
| Size | ||||||
| Mean (SD) | 46.2 (32.3) | 44.0 (25.1) | 0.49 | 43.0 (20.7) | 45.2 (25.5) | 0.774 |
| Median [min, max] | 42.0 [0, 900] | 39.0 [0, 188] | 40.0 [0, 103] | 40.0 [0, 185] | ||
| Survival months | ||||||
| Mean (SD) | 6.23 (8.11) | 14.4 (16.7) | <0.001 | 6.87 (8.33) | 14.3 (18.9) | <0.001 |
| Median [min, max] | 3.00 [0, 82.0] | 9.00 [0, 99.0] | 4.00 [0, 44.0] | 6.00 [0, 99.0] | ||
| Analysis | Overall Survival | Cancer-Specific Survival | ||||
|---|---|---|---|---|---|---|
| Non-Surgery | Surgery | p-Value | Non-Surgery | Surgery | p-Value | |
| Months (95%CI) | Months (95%CI) | Months (95%CI) | Months (95%CI) | |||
| Restricted mean survival time | 6.453 (5.198–7.709) | 9.489 (8.062–10.916) | <0.01 | 6.54 (5.254–7.826) | 9.76 (8.311–11.209) | <0.01 |
| Restricted mean time lost | 13.547 (12.291–14.802) | 10.511 (9.084–11.938) | <0.01 | 13.46 (12.174–14.746) | 10.24 (12.174–14.746) | <0.01 |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Sex (male vs. female) | 0.76 (0.57–1.01) | 0.057 | 0.79 (0.58–1.07) | 0.126 |
| Age (reference <65) | ||||
| ≥85 | 0.67 (0.09–4.86) | 0.695 | 1.22 (0.16–9.15) | 0.849 |
| 65–74 | 1.18 (0.84–1.67) | 0.334 | 1.17 (0.82–1.66) | 0.376 |
| 75–84 | 2.6 (1.82–3.71) | <0.001 | 2.07 (1.41–3.05) | <0.001 |
| Race (reference Black) | ||||
| Other | 0.78 (0.39–1.57) | 0.492 | ||
| White | 1.06 (0.66–1.7) | 0.823 | ||
| Location (reference OthPancreas) | ||||
| PancreasBodyTail | 1.32 (0.83–2.09) | 0.243 | ||
| PancreasHead | 1.35 (0.9–2.03) | 0.142 | ||
| Grade (reference Grade II) | ||||
| Grade III | 1.54 (1.14–2.09) | 0.005 | 1.3 4(0.97–1.85) | 0.08 |
| Grade IV | 2.43 (0.88–6.7) | 0.086 | 1.69 (0.6–4.8) | 0.324 |
| Grade I | 0.94 (0.47–1.89) | 0.867 | 0.52 (0.26–1.08) | 0.079 |
| pT (reference T1) | ||||
| T2 | 0.57 (0.13–2.44) | 0.45 | ||
| T3 | 0.72 (0.16–3.22) | 0.668 | ||
| T4 | 0.77 (0.19–3.1) | 0.708 | ||
| Surgery (yes vs. No) | 0.58 (0.43–0.77) | <0.001 | 0.48 (0.36–0.65) | <0.001 |
| Radiotherapy (yes vs. No) | 0.6 (0.31–1.18) | 0.137 | ||
| Chemotherapy (yes vs. No) | 0.35 (0.26–0.47) | <0.001 | 0.37 (0.26–0.52) | <0.001 |
| Systemic therapy (yes vs. No) | 0.38 (0.22–0.65) | <0.001 | 0.71 (0.4–1.28) | 0.259 |
| Bone metastasis (reference NA) | ||||
| No | 0.54 (0.22–1.31) | 0.172 | ||
| Yes | 0.56 (0.17–1.85) | 0.343 | ||
| Brain metastasis (reference NA) | ||||
| No | 0.49 (0.2–1.19) | 0.114 | ||
| Liver metastasis (reference NA) | ||||
| No | 0.98 (0.67–1.44) | 0.921 | ||
| Lung metastasis (reference NA) | ||||
| No | 0.67 (0.25–1.82) | 0.431 | ||
| Yes | 1.05 (0.37–3.03) | 0.923 | ||
| Distant lymph node metastasis (reference NA) | ||||
| No | 0.78 (0.53–1.14) | 0.195 | ||
| Yes | 0.63 (0.3–1.35) | 0.237 | ||
| Other metastasis (reference NA) | ||||
| No | 0.79 (0.53–1.19) | 0.266 | ||
| Yes | 0.64 (0.35–1.19) | 0.16 | ||
| Metastasis (oligo- vs. multi-) | 1.07 (0.63–1.81) | 0.809 | ||
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Sex (male vs. female) | 0.77 (0.57–1.04) | 0.093 | 0.8(0.58–1.1) | 0.173 |
| Age (reference <65) | ||||
| ≥85 | 0 (0–Inf) | 0.995 | 0 (0–Inf) | 0.993 |
| 65–74 | 1.2 (0.84–1.72) | 0.32 | 1.18 (0.81–1.72) | 0.399 |
| 75–84 | 2.55 (1.77–3.69) | <0.001 | 1.99 (1.33–3) | <0.001 |
| Race (reference Black) | ||||
| Other | 0.8 (0.39–1.65) | 0.548 | ||
| White | 1.12 (0.68–1.86) | 0.649 | ||
| Location (reference OthPancreas) | ||||
| PancreasBodyTail | 1.4 (0.86–2.28) | 0.177 | 1.66 (0.98–2.81) | 0.058 |
| PancreasHead | 1.5 (0.97–2.31) | 0.067 | 1.47 (0.93–2.34) | 0.1 |
| Grade (reference Grade II) | ||||
| Grade III | 1.74 (1.27–2.41) | 0.001 | 1.54 (1.1–2.17) | 0.013 |
| Grade IV | 1.99 (0.62–6.37) | 0.247 | 1.37 (0.42–4.52) | 0.605 |
| Grade I | 1.07 (0.53–2.15) | 0.853 | 0.74 (0.35–1.57) | 0.434 |
| pT (reference T1) | ||||
| T2 | 0.48 (0.11–2.1) | 0.332 | ||
| T3 | 0.66 (0.15–2.96) | 0.583 | ||
| T4 | 0.75 (0.19–3.05) | 0.691 | ||
| Surgery (yes vs. No) | 0.54 (0.4–0.73) | <0.001 | 0.45 (0.33–0.63) | <0.001 |
| Radiotherapy (yes vs. No) | 0.64 (0.33–1.25) | 0.193 | ||
| Chemotherapy (yes vs. No) | 0.33 (0.24–0.45) | <0.001 | 0.38 (0.27–0.55) | <0.001 |
| Systemic therapy (yes vs. No) | 0.35 (0.2–0.63) | <0.001 | 0.67 (0.35–1.25) | 0.206 |
| Bone metastasis (reference NA) | ||||
| No | 0.52 (0.21–1.27) | 0.15 | ||
| Yes | 0.47 (0.14–1.63) | 0.233 | ||
| Brain metastasis (reference NA) | ||||
| No | 0.47 (0.19–1.14) | 0.095 | 0.5 (0.19–1.34) | 0.169 |
| Liver metastasis (reference NA) | ||||
| No | 1.01 (0.68–1.51) | 0.945 | ||
| Lung metastasis (reference NA) | ||||
| No | 0.64 (0.24–1.75) | 0.388 | ||
| Yes | 1 (0.35–2.9) | 0.994 | ||
| Distant lymph node metastasis (reference NA) | ||||
| No | 0.69 (0.46–1.04) | 0.075 | 0.81 (0.53–1.25) | 0.352 |
| Yes | 0.65 (0.3–1.38) | 0.26 | 0.44 (0.2–0.97) | 0.041 |
| Other metastasis (reference NA) | ||||
| No | 0.72 (0.47–1.11) | 0.135 | ||
| Yes | 0.6 (0.31–1.13) | 0.115 | ||
| Metastasis (oligo- vs. multi-) | 1.1 (0.64–1.91) | 0.723 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Zhang, X.; Sun, C.; Li, Z.; Fei, H.; Zhao, D. Does Surgical Resection Significantly Prolong the Long-Term Survival of Patients with Oligometastatic Pancreatic Ductal Adenocarcinoma? A Cross-Sectional Study Based on 18 Registries. J. Clin. Med. 2023, 12, 513. https://doi.org/10.3390/jcm12020513
Li Z, Zhang X, Sun C, Li Z, Fei H, Zhao D. Does Surgical Resection Significantly Prolong the Long-Term Survival of Patients with Oligometastatic Pancreatic Ductal Adenocarcinoma? A Cross-Sectional Study Based on 18 Registries. Journal of Clinical Medicine. 2023; 12(2):513. https://doi.org/10.3390/jcm12020513
Chicago/Turabian StyleLi, Zheng, Xiaojie Zhang, Chongyuan Sun, Zefeng Li, He Fei, and Dongbing Zhao. 2023. "Does Surgical Resection Significantly Prolong the Long-Term Survival of Patients with Oligometastatic Pancreatic Ductal Adenocarcinoma? A Cross-Sectional Study Based on 18 Registries" Journal of Clinical Medicine 12, no. 2: 513. https://doi.org/10.3390/jcm12020513