

The Efficacity of the NeuroAssist Robotic System for Motor Rehabilitation of the Upper Limb—Promising Results from a Pilot Study
 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
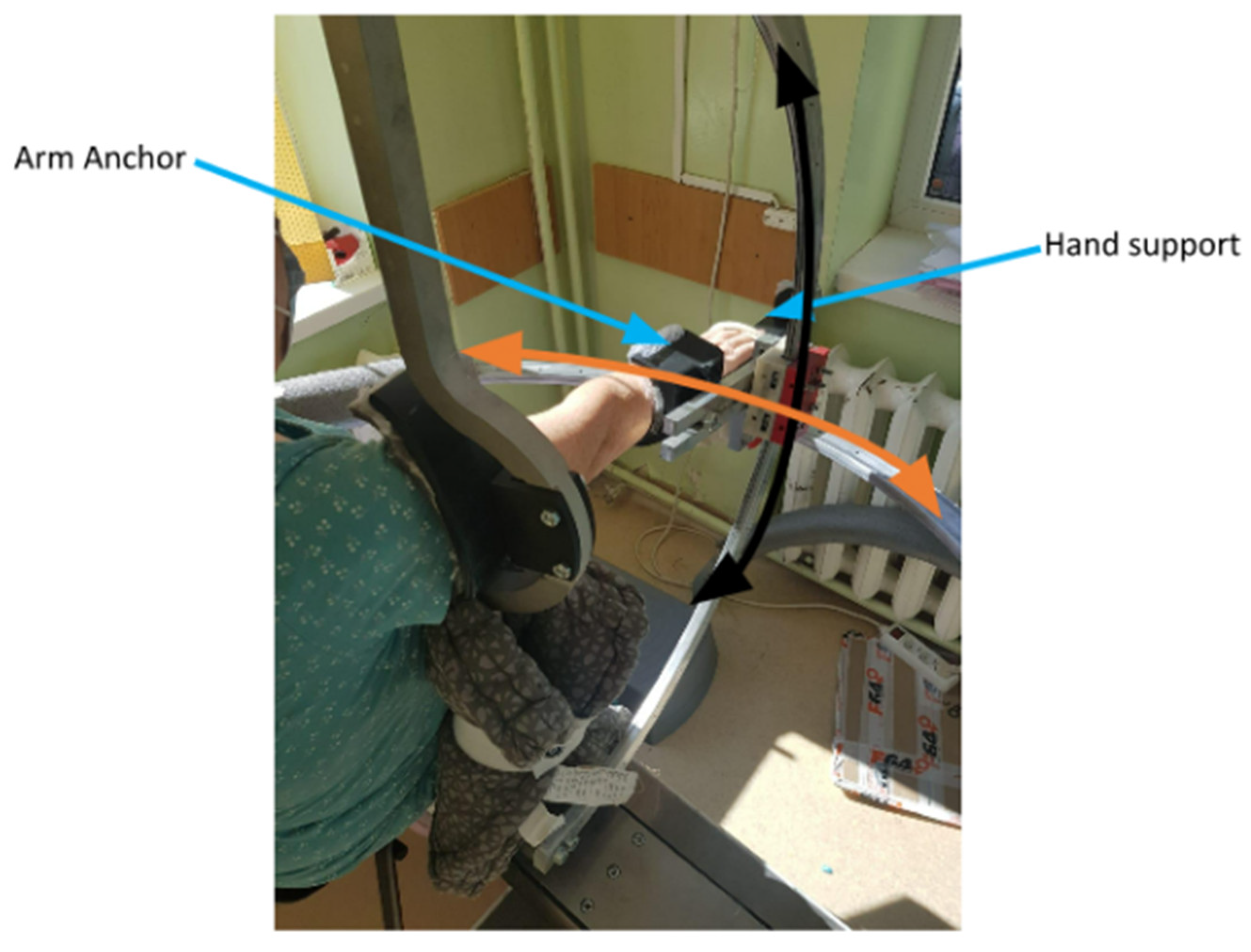
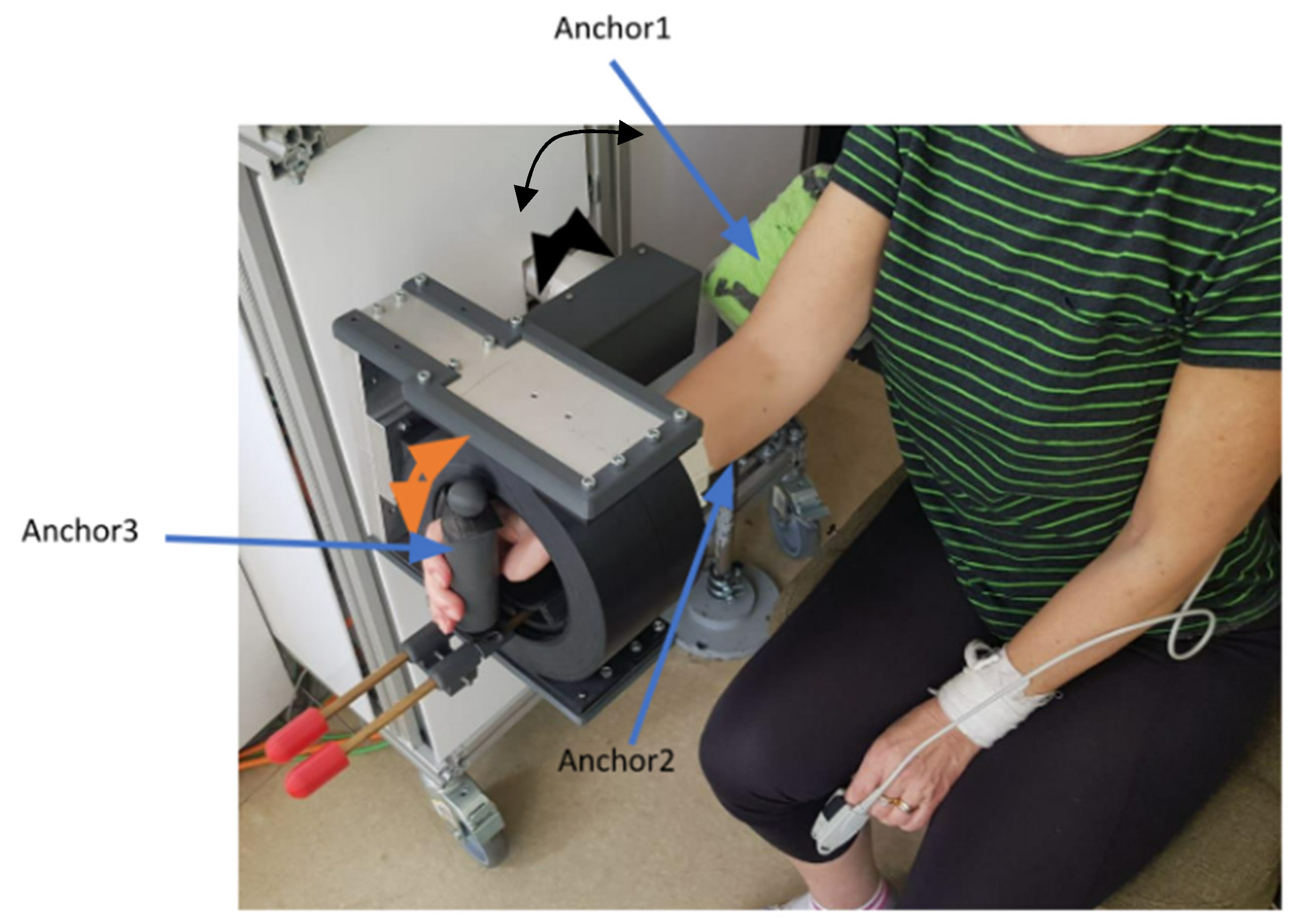
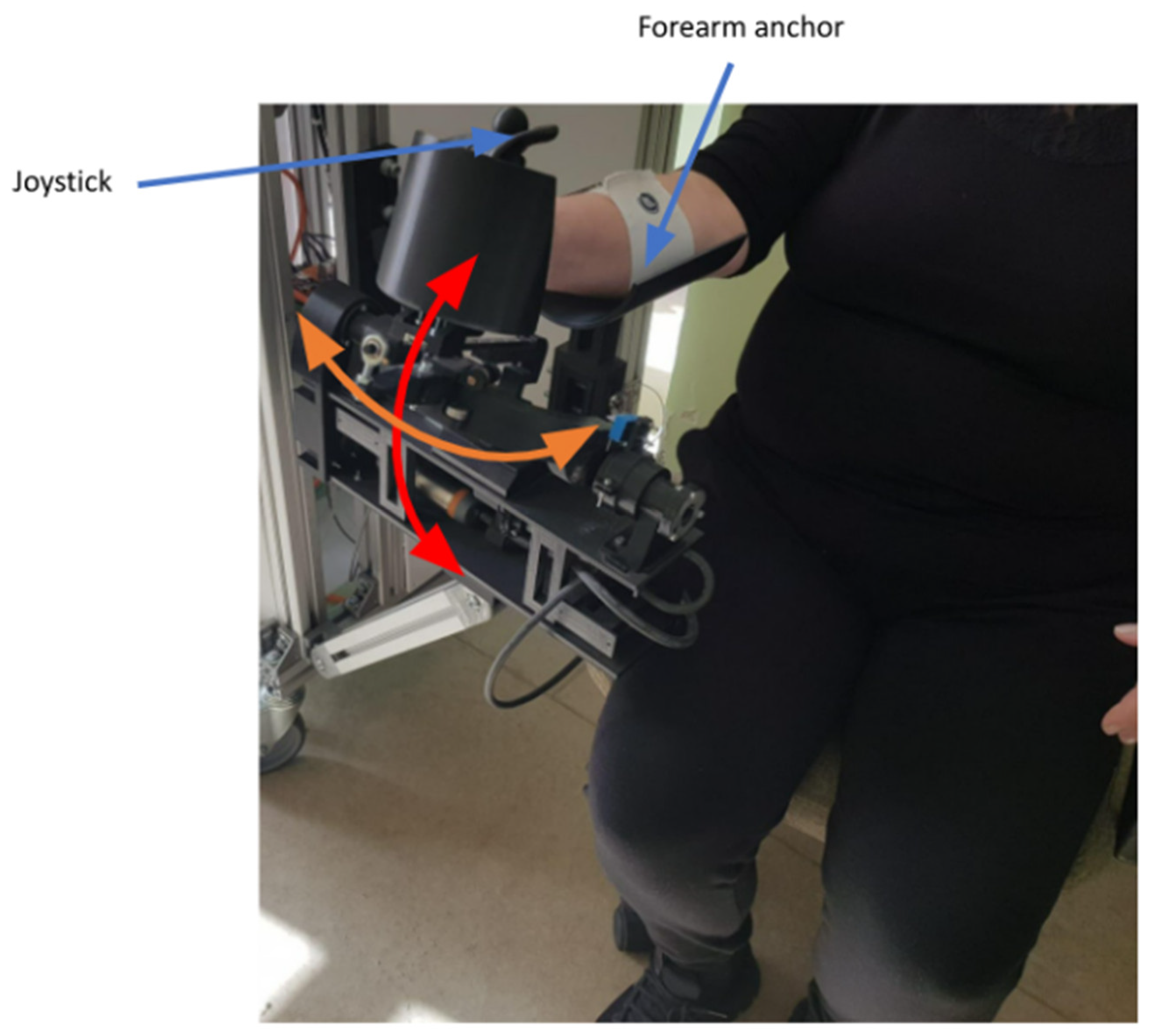
2.1. The Robot
2.2. The Sensors
2.3. The Patients
2.4. The Procedures
2.5. The Intervention
2.6. Statistical Analysis
3. Results
3.1. Clinical and Goniometric Aspects
3.2. Nerve Conduction Studies and Electromyography
3.3. Range of Motion Measurements
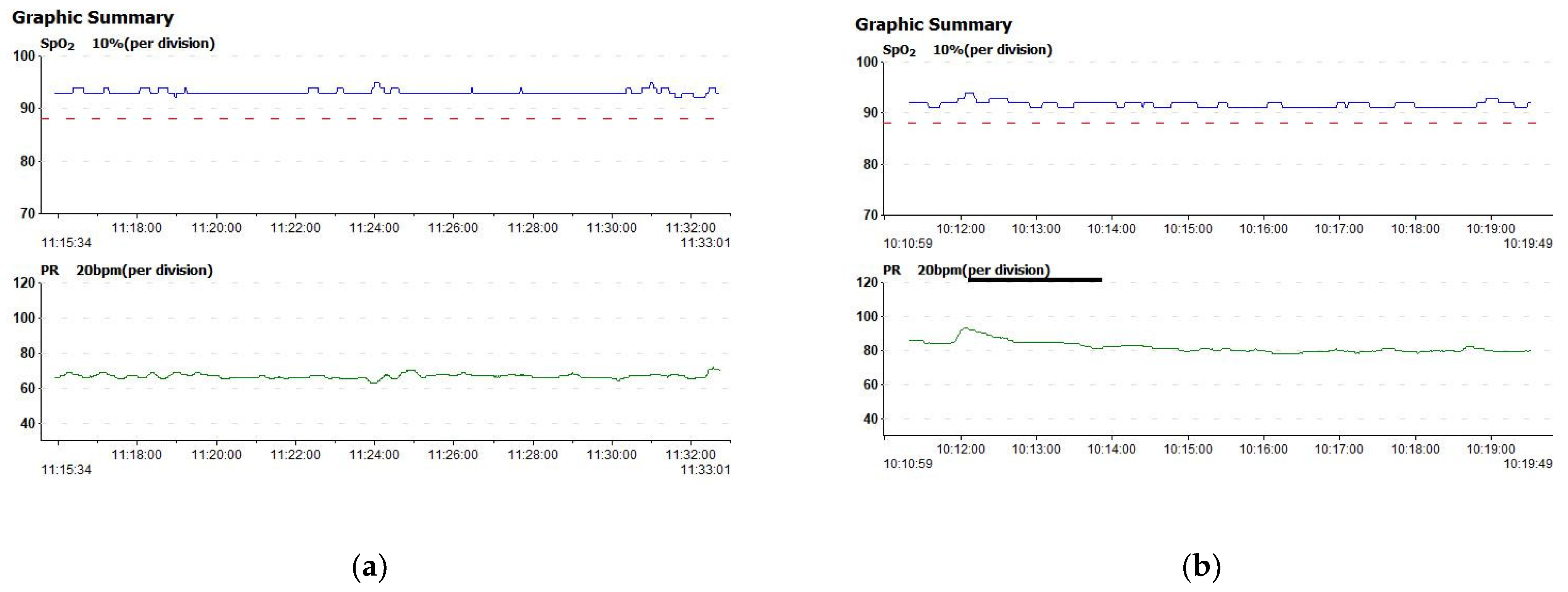
3.4. Vitals during Therapy Sessions
4. Discussion
Study LIMITS and Future Endeavors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, G.; Cocchi, I.; Paolucci, S.; Iosa, M. Robot-assisted therapy for arm recovery for stroke patients: State of the art and clinical implication. Expert Rev. Med. Devices 2020, 17, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.C.; Nelles, G.; Benson, R.R.; Kaplan, J.D.; Parker, R.A.; Kwong, K.K.; Kennedy, D.N.; Finklestein, S.P.; Rosen, B.R. A functional MRI study of subjects recovered from hemiparetic stroke. Stroke 1997, 28, 2518–2527. [Google Scholar] [CrossRef]
- Duret, C.; Grosmaire, A.G.; Krebs, H.I. Robot-assisted therapy in upper extremity hemiparesis: Overview of an evidence-based approach. Front. Neurol. 2019, 10, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, W.T.; Chong, Y.Y.; Tse, M.K.; Chien, C.W.; Cheng, H.Y. Robot-assisted therapy for upper-limb rehabilitation in subacute stroke patients: A systematic review and meta-analysis. Brain Behav. 2020, 10, e01742. [Google Scholar] [CrossRef] [PubMed]
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Zhang, C.; Li-Tsang, C.W.P.; Au, R.K.C. Robotic approaches for the rehabilitation of upper limb recovery after stroke: A systematic review and meta-analysis. Int. J. Rehabil. Res. 2017, 40, 19–28. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2015, 2015, CD006876. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; Van Wegen, E.E.H.; Meskers, C.G.M.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb after Stroke. Neurorehabilit. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef]
- Pignolo, L. Robotics in neuro-rehabilitation. J. Rehabil. Med. 2009, 41, 955–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchwald, A.; Falconer, C.; Rykman-Peltz, A.; Cortes, M.; Pascual-Leone, A.; Thickbroom, G.W.; Krebs, H.I.; Fregni, F.; Gerber, L.M.; Oromendia, C.; et al. Robotic Arm Rehabilitation in Chronic Stroke Patients With Aphasia May Promote Speech and Language Recovery (but Effect Is Not Enhanced by Supplementary tDCS). Front. Neurol. 2018, 9, 853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.S.; Kim, S.H.; Noh, S.E.; Bang, H.J.; Lee, K.M. Robotic-Assisted Shoulder Rehabilitation Therapy Effectively Improved Poststroke Hemiplegic Shoulder Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 1015–1022. [Google Scholar] [CrossRef]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.d.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, R.; Pisano, F.; Delconte, C.; Mazzone, A.; Grioni, G.; Castagna, M.; Bazzini, G.; Imarisio, C.; Maggioni, G.; Pistarini, C. Comparison of exercise training effect with different robotic devices for upper limb rehabilitation: A retrospective study. Eur. J. Phys. Rehabil. Med. 2017, 53, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Colombo, R.; Sterpi, I.; Mazzone, A.; Delconte, C.; Pisano, F. Robot-aided neurorehabilitation in sub-acute and chronic stroke: Does spontaneous recovery have a limited impact on outcome? NeuroRehabilitation 2013, 33, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Brusturean, E.; Gherman, B.; Birlescu, I.; Craciunas, R.; Ulinici, I.; Simori, G.; et al. Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases. J. Pers. Med. 2021, 11, 953. [Google Scholar] [CrossRef]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Simori, G.; Banica, A.; Brusturean, E.; Burz, A.; Craciunas, R.; Ulinici, I.; et al. The Impact of Robotic Rehabilitation on the Motor System in Neurological Diseases. A Multimodal Neurophysiological Approach. Int. J. Environ. Res. Public Health 2020, 17, 6557. [Google Scholar] [CrossRef]
- Pisla, D.; Tarnita, D.; Tucan, P.; Tohanean, N.; Vaida, C.; Geonea, I.D.; Bogdan, G.; Abrudan, C.; Carbone, G.; Plitea, N. A Parallel Robot with Torque Monitoring for Brachial Monoparesis Rehabilitation Tasks. Appl. Sci. 2021, 11, 9932. [Google Scholar] [CrossRef]
- Tucan, P.; Gherman, B.; Major, K.; Vaida, C.; Major, Z.; Plitea, N.; Carbone, G.; Pisla, D. Fuzzy Logic-Based Risk Assessment of a Parallel Robot for Elbow and Wrist Rehabilitation. Int. J. Environ. Res. Public Health 2020, 17, 654. [Google Scholar] [CrossRef]
- Tucan, P.; Vaida, C.; Ulinici, I.; Banica, A.; Burz, A.; Pop, N.; Birlescu, I.; Gherman, B.; Plitea, N.; Antal, T.; et al. Optimization of the ASPIRE Spherical Parallel Rehabilitation Robot Based on Its Clinical Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 3281. [Google Scholar] [CrossRef] [PubMed]
- Geonea, I.D.; Tarnita, D.; Pisla, D.; Carbone, G.; Bolcu, A.; Tucan, P.; Georgescu, M.; Tarniță, D.N. Dynamic Analysis of a Spherical Parallel Robot Used for Brachial Monoparesis Rehabilitation. Appl. Sci. 2021, 11, 11849. [Google Scholar] [CrossRef]
- Tarnita, D.; Geonea, I.D.; Pisla, D.; Carbone, G.; Gherman, B.; Tohanean, N.; Tucan, P.; Abrudan, C.; Tarnita, D.N. Analysis of Dynamic Behavior of ParReEx Robot Used in Upper Limb Rehabilitation. Appl. Sci. 2022, 12, 7907. [Google Scholar] [CrossRef]
- Burz, A.; Tucan, P.; Tohanean, N.; Gherman, B.; Vaida, C.; Abrudan, C.; Carbone, G.; Pisla, D. HRI Based Command System of a Modular Parallel Robot for Brachial Monoparesis. In Proceedings of the 2022 IEEE International Conference on Automation, Quality and Testing, Robotics (AQTR), Cluj-Napoca, Romania, 19–21 May 2022; pp. 1–6. [Google Scholar]
- Carpinella, I.; Cattaneo, D.; Bertoni, R.; Ferrarin, M. Robot Training of Upper Limb in Multiple Sclerosis: Comparing Protocols With or WithoutManipulative Task Components. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 351–360. [Google Scholar] [CrossRef]
- Gijbels, D.; Lamers, I.; Kerkhofs, L.; Alders, G.; Knippenberg, E.; Feys, P. The Armeo Spring as training tool to improve upper limb functionality in multiple sclerosis: A pilot study. J. NeuroEng. Rehabil. 2011, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- Cheung, E.Y.Y.; Ng, T.K.W.; Yu, K.K.K.; Kwan, R.L.C.; Cheing, G.L.Y. Robot-Assisted Training for People With Spinal Cord Injury: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2320–2331. [Google Scholar] [CrossRef]
- Morone, G.; de Sire, A.; Martino Cinnera, A.; Paci, M.; Perrero, L.; Invernizzi, M.; Lippi, L.; Agostini, M.; Aprile, I.; Casanova, E.; et al. Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review. Brain Sci. 2021, 11, 1630. [Google Scholar] [CrossRef]
- Sørensen, L.; Månum, G. A single-subject study of robotic upper limb training in the subacute phase for four persons with cervical spinal cord injury. Spinal Cord Ser. Cases 2019, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Amirabdollahian, F.; Loureiro, R.; Gradwell, E.; Collin, C.; Harwin, W.; Johnson, G. Multivariate analysis of the Fugl-Meyer outcome measures assessing the effectiveness of GENTLE/S robot-mediated stroke therapy. J. NeuroEng. Rehabil. 2007, 4, 4. [Google Scholar] [CrossRef]
- Iandolo, R.; Marini, F.; Semprini, M.; Laffranchi, M.; Mugnosso, M.; Cherif, A.; De Michieli, L.; Chiappalone, M.; Zenzeri, J. Perspectives and Challenges in Robotic Neurorehabilitation. Appl. Sci. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Loureiro, R.; Amirabdollahian, F.; Topping, M.; Driessen, B.; Harwin, W. Upper Limb Robot Mediated Stroke Therapy—GENTLE/s Approach. Auton. Robot. 2003, 15, 35–51. [Google Scholar] [CrossRef] [Green Version]
- Rosati, G.; Gallina, P.; Masiero, S. Design, Implementation and Clinical Tests of a Wire-Based Robot for Neurorehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 560–569. [Google Scholar] [CrossRef]
- Stefano, M.; Patrizia, P.; Mario, A.; Ferlini, G.; Rizzello, R.; Rosati, G. Robotic upper limb rehabilitation after acute stroke by NeReBot: Evaluation of treatment costs. Biomed. Res. Int. 2014, 2014, 265634. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Duret, C.; Grosmaire, A.G.; Battini, E. Combining Upper Limb Robotic Rehabilitation with Other Therapeutic Approaches after Stroke: Current Status, Rationale, and Challenges. Biomed. Res. Int. 2017, 2017, 8905637. [Google Scholar] [CrossRef]
- Chen, Z.J.; Gu, M.H.; He, C.; Xiong, C.H.; Xu, J.; Huang, X.L. Robot-Assisted Arm Training in Stroke Individuals With Unilateral Spatial Neglect: A Pilot Study. Front. Neurol. 2021, 12, 691444. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Li, Q.-y.; Qu, Q.; Ding, L.; Chen, Z.; Huang, F.; Hu, S.; Deng, W.; Guo, F.; Wang, C.; et al. Comparative Effectiveness of Robot-Assisted Training Versus Enhanced Upper Extremity Therapy on Upper and Lower Extremity for Stroke Survivors: A Multicentre Randomized Controlled Trial. J. Rehabil. Med. 2022, 54, jrm00314. [Google Scholar] [CrossRef]
- Sale, P.; Franceschini, M.; Mazzoleni, S.; Palma, E.; Agosti, M.; Posteraro, F. Effects of upper limb robot-assisted therapy on motor recovery in subacute stroke patients. J. NeuroEng. Rehabil. 2014, 11, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehem, S.; Gilliaux, M.; Stoquart, G.; Detrembleur, C.; Jacquemin, G.; Palumbo, S.; Frederick, A.; Lejeune, T. Effectiveness of upper-limb robotic-assisted therapy in the early rehabilitation phase after stroke: A single-blind, randomised, controlled trial. Ann. Phys. Rehabil. Med. 2019, 62, 313–320. [Google Scholar] [CrossRef]
- Budhota, A.; Chua, K.S.G.; Hussain, A.; Kager, S.; Cherpin, A.; Contu, S.; Vishwanath, D.; Kuah, C.W.K.; Ng, C.Y.; Yam, L.H.L.; et al. Robotic Assisted Upper Limb Training Post Stroke: A Randomized Control Trial Using Combinatory Approach Toward Reducing Workforce Demands. Front. Neurol. 2021, 12, 622014. [Google Scholar] [CrossRef]
- Shapiro, D.C.P.B.E. Electromyography and Neuromuscular Disorders, 4th ed.; Clinical-Electrophysiologic-Ultrasound Correlations; Elsevier: Philadelphia, PA, USA, 2020. [Google Scholar]
- Dziemian, K.; Kiper, A.; Baba, A.; Baldan, F.; Alhelou, M.; Agostini, M.; Turolla, A.; Kiper, P. The effect of robot therapy assisted by surface EMG on hand recovery in post-stroke patients. A pilot study. Med. Rehabil. 2017, 21, 4–10. [Google Scholar] [CrossRef]
- Törnbom, K.; Sunnerhagen, K.S.; Danielsson, A. Perceptions of physical activity and walking in an early stage after stroke or acquired brain injury. PLoS ONE 2017, 12, e0173463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T1 | T2 | Z | p | |
|---|---|---|---|---|
| Barthel Index (points) | 53.00 (37.72) | 60.50 (36.39) | −2.41 | 0.016 |
| ADL (points) | 4.70 (3.43) | 5.50 (3.80) | −2.07 | 0.038 |
| Dynamometer (kg) | 8.33 (8.37) | 9.89 (10.06) | −1.57 | 0.116 |
| Muscle segment strength (Scale) | 2.70 (1.61) | 3.30 (0.91) | −1.85 | 0.063 |
| Shoulder abduction (degrees) | 54.00 (47.71) | 58.50 (52.33) | −1.34 | 0.180 |
| Shoulder flexion (degrees) | 70.00 (56.61) | 80.00 (63.59) | −2.20 | 0.026 |
| Elbow flexion (degrees) | 105.50 (59.18) | 120.50 (55.35) | −1.82 | 0.068 |
| Wrist flexion (degrees) | 34.00 (28.75) | 42.50 (33.76) | −2.03 | 0.042 |
| Wrist extension (degrees) | 30.00 (22.97) | 41.00 (30.62) | −2.03 | 0.042 |
| Ulnar deviation (degrees) | 23.50 (19.44) | 33.50 (24.15) | −2.21 | 0.027 |
| Radial deviation (degrees) | 17.50 (18.14) | 27.00 (24.85) | −2.20 | 0.027 |
| Pronation (degrees) | 52.50 (45.41) | 53.50 (46.07) | −1.00 | 0.317 |
| Supination (degrees) | 47.50 (44.04) | 54.50 (41.79) | −1.60 | 1.109 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Barthel Index | - | ||||||||||||
| 2. ADL Index | 0.98 ** | - | |||||||||||
| 3. Muscle strength | 0.78 ** | 0.80 ** | - | ||||||||||
| 4. Shoulder abduction | 0.84 ** | 0.86 ** | 0.91 ** | - | |||||||||
| 5. Shoulder flexion | 0.92 ** | 0.94 ** | 0.91 ** | 0.95 ** | - | ||||||||
| 6. Elbow flexion | 0.91 ** | 0.91 ** | 0.83 ** | 0.88 ** | 0.92 ** | - | |||||||
| 7. Wrist flexion | 0.78 ** | 0.74 * | 0.70 * | 0.72 * | 0.78 ** | 0.81 ** | - | ||||||
| 8. Wrist extension | 0.85 ** | 0.83 ** | 0.65 * | 0.62 | 0.78 ** | 0.83 ** | 0.78 ** | - | |||||
| 9. Ulnar deviation | 0.78 ** | 0.79 ** | 0.78 ** | 0.76 ** | 0.83 ** | 0.88 ** | 0.80 ** | 0.91 ** | - | ||||
| 10. Radial deviation | 0.77 ** | 0.77 ** | 0.82 ** | 0.88 ** | 0.89 ** | 0.75 * | 0.82 ** | 0.57 | 0.65 * | - | |||
| 11. Pronation | 0.85 ** | 0.85 ** | 0.91 ** | 0.98 ** | 0.93 ** | 0.89 ** | 0.71 * | 0.62 | 0.75 * | 0.84 ** | - | ||
| 12. Supination | 0.75 * | 0.75 * | 0.90 ** | 0.95 ** | 0.87 ** | 0.88 ** | 0.75 * | 0.62 | 0.82 ** | 0.81 ** | 0.96 ** | ||
| 13. Dynamometer | 0.72 * | 0.74 * | 0.76 ** | 0.85 ** | 0.84 ** | 0.75 * | 0.68 * | 0.72 * | 0.85 ** | 0.80 ** | 0.77 ** | 0.81 ** | - |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Barthel | 1 | ||||||||||||
| 2. ADL | 0.98 ** | 1 | |||||||||||
| 3. FMS | 0.59 | 0.66 * | 1 | ||||||||||
| 4. Shoulder abduction | 0.86 ** | 0.90 ** | 0.84 ** | 1 | |||||||||
| 5. Shoulder flexion | 0.93 ** | 0.95 ** | 0.80 ** | 0.95 ** | 1 | ||||||||
| 6. Elbow flexion | 0.85 ** | 0.87 ** | 0.51 | 0.75 * | 0.82 ** | 1 | |||||||
| 7. Wrist flexion | 0.87 ** | 0.89 ** | 0.70 * | 0.86 ** | 0.89 ** | 0.80 ** | 1 | ||||||
| 8. Wrist extension | 0.88 ** | 0.86 ** | 0.57 | 0.78 ** | 0.82 ** | 0.85 ** | 0.93 ** | 1 | |||||
| 9. Ulnar deviation | 0.92 ** | 0.91 ** | 0.54 | 0.81 ** | 0.85 ** | 0.87 ** | 0.95 ** | 0.98 ** | 1 | ||||
| 10. Radial deviation | 0.78 ** | 0.78 ** | 0.64 * | 0.81 ** | 0.79 ** | 0.69 * | 0.90 ** | 0.78 ** | 0.82 ** | 1 | |||
| 11. Pronation | 0.89 ** | 0.90 ** | 0.76* | 0.96 ** | 0.93 ** | 0.76 ** | 0.81 ** | 0.77 ** | 0.80 ** | 0.81 ** | 1 | ||
| 12. Supination | 0.94 ** | 0.94 ** | 0.72 * | 0.95 ** | 0.94 ** | 0.85 ** | 0.90 ** | 0.89 ** | 0.91 ** | 0.85 ** | 0.97 ** | 1 | |
| 13. Dynamometer | 0.75 * | 0.82 ** | 0.73 * | 0.88 ** | 0.82 ** | 0.64 * | 0.90 ** | 0.73 * | 0.79 ** | 0.87 ** | 0.79 ** | 0.81 ** |
| ENoG Parameters | T1 | T2 | Z | p |
|---|---|---|---|---|
| aCMAP median (mV) | 6.40 (2.34) | 6.95 (2.32) | −1.21 | 0.225 |
| mVCM median (m/s) | 58.55 (8.79) | 58.66 (8.03) | −1.21 | 0.500 |
| F waves median (ms) | 23.63 (2.64) | 23.03 (2.93) | −0.67 | 0.500 |
| aCMAP ulnar (mV) | 6.75 (2.24) | 6.45 (2.38) | −1.57 | 0.116 |
| mVCM ulnar (m/s) | 67.45 (9.67) | 62.95 (9.94) | −1.48 | 0.138 |
| F waves ulnar (ms) | 24.85 (3.52) | 25.27 (3.27) | −0.13 | 0.893 |
| aSNAP median (µV) | 16.34 (15.04) | 13.71 (11.97) | −0.40 | 0.686 |
| aSNAP ulnar (µV) | 16.44 (18.12) | 15.41 (18.44) | −0.67 | 0.500 |
| aSNAP radial (µV) | 18.82 (5.46) | 16.43 (6.20) | −1.36 | 0.173 |
| T1 | T2 | Z | p | |
|---|---|---|---|---|
| ABP FIB | 0.40 (0.69) | 0.90 (1.10) | −1.63 | 0.102 |
| ABP PSW | 0.00 (0.00) | 0.30 (0.48) | −1.73 | 0.083 |
| ABP activation | 1.00 (0.94) | 1.10 (1.10) | −1.00 | 0.317 |
| ABP MAUP amp | 452.50 (267.62) | 531.83 (249.27) | −0.73 | 0.461 |
| ABP MAUP duration | 15.15 (11.36) | 13.11 (6.08) | −0.67 | 0.500 |
| ABP polyphasic | 41.67 (40.82) | 29.67 (35.01) | −0.73 | 0.465 |
| ABP recruitment | 1.10 (0.99) | 1.20 (1.13) | −1.00 | 0.317 |
| FCR FIB | 0.10 (0.31) | 0.20 (0.63) | −0.44 | 0.655 |
| FCR PSW | 0.00 (0.00) | 0.00 (0.00) | 0.00 | 1.000 |
| FCR activation | 1.00 (0.94) | 1.30 (0.94) | −1.73 | 0.083 |
| FCR MAUP amp | 498.67 (334.72) | 531.71 (398.33) | −0.73 | 0.465 |
| FCR MAUP duration | 12.53 (3.59) | 13.97 (6.99) | −0.36 | 0.715 |
| FCR polyphasic | 37.00 (26.53) | 40.14 (30.85) | −0.36 | 0.715 |
| FCR recruitment | 1.10 (0.99) | 1.30 (0.949) | −1.41 | 0.157 |
| EDC FIB | 0.30 (0.67) | 0.40 (0.69) | −0.57 | 0.564 |
| EDC PSW | 0.10 (0.31) | 0.10 (0.31) | 0.00 | 1.000 |
| EDC activation | 1.00 (0.94) | 1.40 (1.17) | −2.00 | 0.046 |
| EDC MAUP amp | 665.00 (163.24) | 822.14 (339.40) | −1.21 | 0.225 |
| EDC MAUP duration | 19.17 (6.61) | 19.88 (8.00) | −0.40 | 0.684 |
| EDC polyphasic | 63.29 (35.44) | 65.86 (36.88) | −1.13 | 0.257 |
| EDC recruitment | 1.10 (0.99) | 1.60 (1.35) | −1.89 | 0.059 |
| Biceps FIB | 0.20 (0.63) | 0.40 (0.69) | −0.55 | 0.577 |
| Biceps PSW | 0.00 (0.00) | 0.10 (0.31) | −1.00 | 0.317 |
| Biceps activation | 1.30 (0.82) | 1.60 (0.96) | −1.73 | 0.083 |
| Biceps MAUP amp | 524.13 (221.94) | 510.63 (230.02) | −0.94 | 0.345 |
| Biceps MAUP duration | 15.05 (7.52) | 13.20 (5.99) | −1.78 | 0.075 |
| Biceps polyphasic | 39.00 (35.78) | 25.13 (35.58) | −1.36 | 0.173 |
| Biceps recruitment | 1.30 (0.82) | 1.50 (0.97) | −1.41 | 0.157 |
| Deltoid FIB | 0.30 (0.67) | 0.60 (0.84) | −1.34 | 0.180 |
| Deltoid PSW | 0.10 (0.31) | 0.20 (0.42) | −1.00 | 0.317 |
| Deltoid activation | 1.30 (0.94) | 1.60 (0.96) | −1.73 | 0.083 |
| Deltoid MAUP amp | 584.38 (166.29) | 587.67 (337.83) | −0.52 | 0.600 |
| Deltoid MAUP duration | 18.97 (6.06) | 13.144 (3.88) | −1.99 | 0.046 |
| Deltoid polyphasic | 60.25 (33.20) | 39.56 (23.06) | −1.75 | 0.080 |
| Deltoid recruitment | 1.50 (1.08) | 1.70 (1.05) | −1.41 | 0.157 |
| FDS FIB | 0.00 (0.00) | 0.00 (0.00) | 0.00 | 1.000 |
| FDS PSW | 0.00 (0.00) | 0.00 (0.00) | 0.00 | 1.000 |
| FDS activation | 1.00 (1.054) | 1.20 (1.13) | −1.41 | 0.157 |
| FDS MAUP amp | 597.33 (231.20) | 630.50 (336.98) | −0.40 | 0.686 |
| FDS MAUP duration | 14.50 (4.62) | 13.783 (5.41) | −0.27 | 0.786 |
| FDS polyphasic | 41.33 (35.27) | 48.17 (31.09) | −0.13 | 0.893 |
| FDS recruitment | 1.10 (1.10) | 1.30 (1.16) | −1.41 | 0.157 |
| T1 | T2 | Z | p | |
|---|---|---|---|---|
| Wrist flexion amplitude (degrees) | 48.00 (15.846) | 55.00 (13.744) | −2.80 | 0.005 |
| Wrist extension amplitude (degrees) | 42.50 (10.341) | 48.50 (11.068) | −2.80 | 0.005 |
| Wrist flexion-extension speed (degrees/second) | 30.00 (0.00) | 30.00 (0.00) | 0.00 | 1.000 |
| Wrist flexion-extension repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| Wrist abduction amplitude (degrees) | 22.00 (7.528) | 26.00 (6.146) | −2.53 | 0.011 |
| Wrist adduction amplitude (degrees) | 31.00 (9.944) | 35.00 (5.774) | −2.33 | 0.020 |
| Wrist abduction-adduction speed (degrees/second) | 30.00 (0.00) | 30.00 (0.00) | 0.00 | 1.000 |
| Wrist abduction-adduction repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| Elbow flexion amplitude (degrees) | 73.50 (2.41) | 73.50 (2.41) | 0.00 | 1.000 |
| Elbow extension amplitude (degrees) | 13.50 (2.41) | 13.50 (2.41) | 0.00 | 1.000 |
| Elbow flexion-extension speed (degrees/second) | 10.00 (0.00) | 10.00 (0.00) | 0.00 | 1.000 |
| Elbow flexion-extension repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| Elbow pronation amplitude (degrees) | 60.00 (0.00) | 60.00 (0.00) | 0.00 | 1.000 |
| Elbow supination amplitude (degrees) | 45.00 (0.00) | 45.00 (0.00) | 0.00 | 1.000 |
| Elbow pronation/supination speed (degrees/second) | 15.00 (0.00) | 15.00 (0.00) | 0.00 | 1.000 |
| Elbow pronation/supination repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| Shoulder flexion amplitude (degrees) | 61.00 (4.59) | 62.50 (4.85) | −1.73 | 0.083 |
| Shoulder extension amplitude (degrees) | 0.00 (0.00) | 0.00 (0.00) | 0.00 | 1.000 |
| Shoulder flexion-extension speed (degrees/second) | 10.00 (0.00) | 10.00 (0.00) | 0.00 | 1.000 |
| Shoulder flexion-extension repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| Shoulder abduction amplitude (degrees) | 29.00 (16.63) | 33.50 (16.50) | −2.06 | 0.039 |
| Shoulder adduction amplitude (degrees) | 29.00 (3.16) | 30.00 (0.00) | 1.00 | 0.317 |
| Shoulder abduction-adduction speed (degrees /second) | 20.00 (0.00) | 20.00 (0.00) | 0.00 | 1.000 |
| Shoulder abduction-adduction repetitions/minute | 15.00 (0.00) | 30.00 (0.00) | −3.16 | 0.002 |
| T1 | T2 | Z | p | |
|---|---|---|---|---|
| Shoulder abduction | 52.81 (46.66) | 57.21 (51.19) | −1.34 | 0.180 |
| Shoulder flexion | 68.46 (55.37) | 78.24 (62.20) | −2.22 | 0.026 |
| Elbow flexion | 103.18 (55.37) | 117.85 (54.13) | −1.82 | 0.068 |
| Wrist flexion | 33.25 (28.12) | 41.57 (33.03) | −2.03 | 0.042 |
| Wrist extension | 29.34 (22.47) | 40.10 (29.95) | −2.03 | 0.042 |
| Ulnar deviation | 22.98 (19.02) | 32.76 (23.63) | −2.21 | 0.027 |
| Radial deviation | 17.12 (17.74) | 26.41 (24.31) | −0.20 | 0.026 |
| Pronation | 51.35 (44.42) | 52.32 (45.06) | −1.00 | 0.317 |
| Supination | 46.46 (43.08) | 53.30 (40.88) | −1.60 | 0.109 |
| Goniometer | Shoulder Abduction | Shoulder Flexion | Elbow Flexion | Wrist Flexion | Wrist Extension | Ulnar Deviation | Radial Deviation | Pronation | Supination |
|---|---|---|---|---|---|---|---|---|---|
| Sensors | |||||||||
| Shoulder abduction | 1 | ||||||||
| Shoulder flexion | 0.950 * | 1 | |||||||
| Elbow flexion | 0.885 * | 0.922 * | 1 | ||||||
| Wrist flexion | 0.722 * | 0.783 * | 0.817 * | 1 | |||||
| Wrist extension | 0.628 * | 0.784 * | 0.832 * | 0.782 * | 1 | ||||
| Ulnar deviation | 0.768 * | 0.833 * | 0.887 * | 0.802 * | 0.914 * | 1 | |||
| Radial deviation | 0.889 * | 0.898 * | 0.759 * | 0.820 * | 0.573 * | 0.658 * | 1 | ||
| Pronation | 0.984 * | 0.933 * | 0.891 * | 0.715 * | 0.623 * | 0.750 * | 0.845 * | 1 | |
| Supination | 0.952 * | 0.878 * | 0.880 * | 0.759 * | 0.620 * | 0.822 * | 0.812 * | 0.960 * | 1 |
| Goniometer | Shoulder Abduction | Shoulder Flexion | Elbow Flexion | Wrist Flexion | Wrist Extension | Ulnar Deviation | Radial Deviation | Pronation | Supination |
|---|---|---|---|---|---|---|---|---|---|
| Sensors | |||||||||
| Shoulder abduction | 1 | ||||||||
| Shoulder flexion | 0.954 * | 1 | |||||||
| Elbow flexion | 0.758 * | 0.825 * | 1 | ||||||
| Wrist flexion | 0.867 * | 0.891 * | 0.809 * | 1 | |||||
| Wrist extension | 0.788 * | 0.827 * | 0.850 * | 0.935 * | 1 | ||||
| Ulnar deviation | 0.811 * | 0.852 * | 0.871 * | 0.952 * | 0.982 * | 1 | |||
| Radial deviation | 0.812 * | 0.794 * | 0.694 * | 0.900 * | 0.785 * | 0.829 * | 1 | ||
| Pronation | 0.968 * | 0.932 * | 0.767 * | 0.810 * | 0.777 * | 0.801 * | 0.816 * | 1 | |
| Supination | 0.956 * | 0.949 * | 0.851 * | 0.902 * | 0.899 * | 0.915 * | 0.854 * | 0.972 * | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tohanean, N.; Tucan, P.; Vanta, O.-M.; Abrudan, C.; Pintea, S.; Gherman, B.; Burz, A.; Banica, A.; Vaida, C.; Neguran, D.A.; et al. The Efficacity of the NeuroAssist Robotic System for Motor Rehabilitation of the Upper Limb—Promising Results from a Pilot Study. J. Clin. Med. 2023, 12, 425. https://doi.org/10.3390/jcm12020425
Tohanean N, Tucan P, Vanta O-M, Abrudan C, Pintea S, Gherman B, Burz A, Banica A, Vaida C, Neguran DA, et al. The Efficacity of the NeuroAssist Robotic System for Motor Rehabilitation of the Upper Limb—Promising Results from a Pilot Study. Journal of Clinical Medicine. 2023; 12(2):425. https://doi.org/10.3390/jcm12020425
Chicago/Turabian StyleTohanean, Nicoleta, Paul Tucan, Oana-Maria Vanta, Cristian Abrudan, Sebastian Pintea, Bogdan Gherman, Alin Burz, Alexandru Banica, Calin Vaida, Deborah Alice Neguran, and et al. 2023. "The Efficacity of the NeuroAssist Robotic System for Motor Rehabilitation of the Upper Limb—Promising Results from a Pilot Study" Journal of Clinical Medicine 12, no. 2: 425. https://doi.org/10.3390/jcm12020425