
Effects of Multidisciplinary Rehabilitation Program in Patients with Long COVID-19: Post-COVID-19 Rehabilitation (PCR SIRIO 8) Study
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. End Points
- change in body composition;
- change in the CPET results (peak oxygen consumption [VO2 peak], predicted VO2 peak, VO2peak/breathing frequencypeak, predicted VO2peak/breathing frequencypeak (%), minute ventilation to carbon dioxide production [VE/VCO2], oxygen uptake efficiency slope [OUES], anaerobic threshold [AT]);
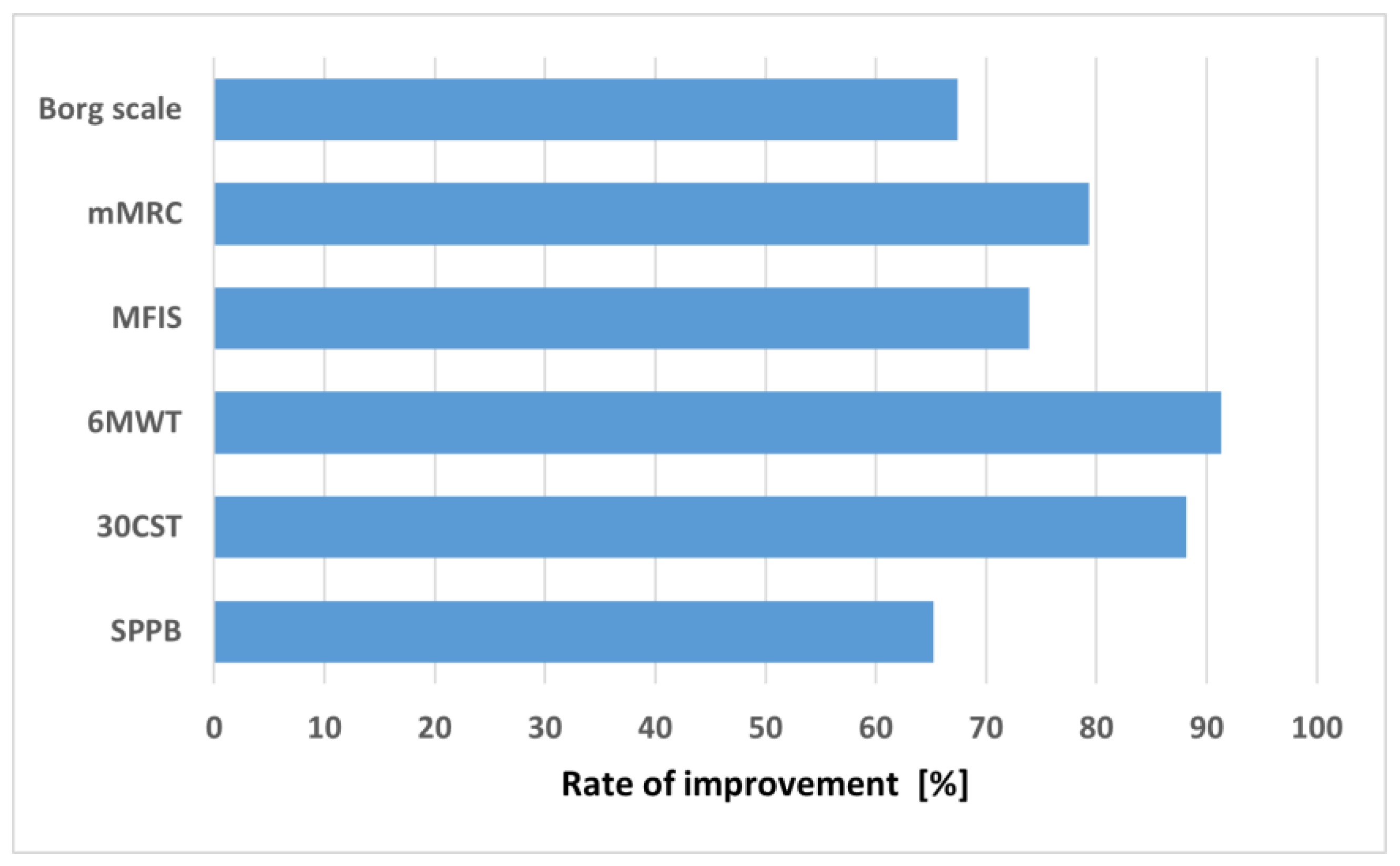
- change in perceived fatigue accordingly to the MFIS;
- change in perceived dyspnea accordingly to the mMRC dyspnea scale and the Borg scale;
- change in exercise tolerance accordingly to the 6MWT and the 30 CST;
- change in physical fitness accordingly to the SPPB test.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajda, R. The fear of COVID—A factor affecting the functioning of emergency medical service. Med. Res. J. 2022, 7, 272–273. [Google Scholar] [CrossRef]
- Kowalik, M.M.; Trzonkowski, P.; Łasińska-Kowara, M.; Mital, A.; Smiatacz, T.; Jaguszewski, M. COVID-19—Toward a comprehensive understanding of the disease. Cardiol. J. 2020, 27, 99–114. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19): Global Situation, Number of Confirmed Cases. Available online: https://covid19.who.int/ (accessed on 27 November 2022).
- Carfì, A.; Bernabei, R.; Landi, F. Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Sykes, D.L.; Holdsworth, L.; Jawad, N.; Gunasekera, P.; Morice, A.H.; Crooks, M.G. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ARC Study Group. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19): Post COVID-19 Condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 27 November 2022).
- Cabrera Martimbianco, A.L.; Pacheco, R.L.; Bagattini, Â.M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, 14357. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ 2021, 374, 1648. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain. Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Kujawski, S.; Zalewski, P.; Newton, J.L. Do some long COVID patients suffer from ME/CFS? Med. Res. J. 2021, 6, 279–280. [Google Scholar] [CrossRef]
- Renaud-Charest, O.; Lui, L.M.W.; Eskander, S.; Ceban, F.; Ho, R.; Di Vincenzo, J.D.; Rosenblat, J.D.; Lee, Y.; Subramaniapillai, M.; McIntyre, R.S. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 2021, 144, 129–137. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain. Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Kubica, A.; Michalski, P.; Kasprzak, M.; Podhajski, P.; Pietrzykowski, Ł.; Rzepka-Cholasińska, A.; Fabiszak, T.; Kryś, J. Functioning of patients with post-COVID syndrome—preliminary data. Med. Res. J. 2021, 6, 224–229. [Google Scholar] [CrossRef]
- Winzer, E.B.; Woitek, F.; Linke, A. Physical Activity in the Prevention and Treatment of Coronary Artery Disease. J. Am. Heart. Assoc. 2018, 7, 007725. [Google Scholar] [CrossRef] [Green Version]
- Soderlund, P.D. Effectiveness of motivational interviewing for improving physical activity self-management for adults with type 2 diabetes: A review. Chronic Illn. 2018, 14, 54–68. [Google Scholar] [CrossRef] [Green Version]
- Navidad, L.; Padial-Ruz, R.; González, M.C. Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 187. [Google Scholar] [CrossRef]
- Michalski, P.; Kosobucka, A.; Pietrzykowski, Ł.; Kasprzak, M.; Buszko, K.; Obońska, K.; Fabiszak, T.; Kubica, A. Effectiveness of therapeutic education in patients with myocardial infarction. Med. Res. J. 2018, 2, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Michalski, P.; Kasprzak, M.; Siedlaczek, M.; Kubica, A. The impact of knowledge and effectiveness of educational intervention on readiness for hospital discharge and adherence to therapeutic recommendations in patients with acute coronary syndrome. Med. Res. J. 2020, 5, 72–78. [Google Scholar] [CrossRef]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am. J. Physiol. Heart. Circ. Physiol. 2020, 318, 1441–1446. [Google Scholar] [CrossRef]
- Rinaldo, R.F.; Mondoni, M.; Parazzini, E.M.; Pitari, F.; Brambilla, E.; Luraschi, S.; Balbi, M.; Sferrazza Papa, G.F.; Sotgiu, G.; Guazzi, M.; et al. Deconditioning as main mechanism of impaired exercise response in COVID-19 survivors. Eur. Respir. J. 2021, 58, 2100870. [Google Scholar] [CrossRef] [PubMed]
- Kubica, A.; Michalski, P.; Pietrzykowski, Ł.; Rzepka-Cholasińska, A.; Kosobucka-Ozdoba, A.; Jasiewicz, M.; Laskowska, E.; Kryś, J.; Ostrowska, M. Post-COVID-19 rehabilitation (PCR-SIRIO 8) study. A rationale and protocol of the study. Med. Res. J. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Kuodi, P.; Gorelik, Y.; Zayyad, H.; Wertheim, O.; Wiegler, K.B.; Jabal, K.A.; Dror, A.A.; Nazzal, S.; Glikan, D.; Edelstein, M. Association between vaccination status and reported incidence of post-acute COVID-19 symptoms in Israel: A cross-sectional study 2020-21, Israel. NPJ Vaccines 2022, 7, 101. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence (NICE): London, UK, 2021.
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports. Med. 2020, 54, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation After COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef]
- Takekawa, T.; Kashiwabara, K.; Yamada, N.; Watanabe, S.; Hama, M.; Hashimoto, G.; Abo, M.; Shinfuku, K. Rehabilitation therapy for a severe case of coronavirus disease 2019: A case report. J. Med. Case Rep. 2022, 16, 339. [Google Scholar] [CrossRef]
- Udina, C.; Ars, J.; Morandi, A.; Vilaró, J.; Cáceres, C.; Inzitari, M. Rehabilitation in adult post-COVID-19 patients in post-acute care with Therapeutic Exercise. J. Frailty Aging 2021, 10, 297–300. [Google Scholar] [CrossRef]
- Barbara, C.; Clavario, P.; De Marzo, V.; Lotti, R.; Guglielmi, G.; Porcile, A.; Russo, C.; Griffo, R.; Mäkikallio, T.; Hautala, A.J.; et al. Effects of exercise rehabilitation in patients with long coronavirus disease 2019. Eur. J. Prev. Cardiol. 2022, 29, e258–e260. [Google Scholar] [CrossRef]
- Besnier, F.; Bérubé, B.; Malo, J.; Gagnon, C.; Grégoire, C.A.; Juneau, M.; Simard, F.; L’Allier, P.; Nigam, A.; Iglésies-Grau, J.; et al. Cardiopulmonary Rehabilitation in Long-COVID-19 Patients with Persistent Breathlessness and Fatigue: The COVID-Rehab Study. Int. J. Environ. Res. Public Health 2022, 19, 4133. [Google Scholar] [CrossRef]
- Morrow, A.; Gray, S.R.; Bayes, H.K.; Sykes, R.; McGarry, E.; Anderson, D.; Boiskin, D.; Burke, C.; Cleland, J.G.F.; Goodyear, C.; et al. Prevention and early treatment of the long-term physical effects of COVID-19 in adults: Design of a randomised controlled trial of resistance exercise-CISCO-21. Trials 2022, 23, 660. [Google Scholar] [CrossRef]
- Flannery, T.; Brady-Sawant, H.; Tarrant, R.; Davison, J.; Shardha, J.; Halpin, S.; Sivan, M.; Ross, D. A Mixed-Methods Evaluation of a Virtual Rehabilitation Program for Self-Management in Post-COVID-19 Syndrome (Long COVID). Int. J. Environ. Res. Public Health 2022, 19, 2680. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Study Population (n = 97) |
|---|---|
| Age [years] | 60.0 (50.0–68.0) |
| Female | 53 (54.6) |
| Body mass index [kg/m2] | 28.1 (24.4–31.1) |
| Current smoker | 11 (11.3) |
| Hypertension | 45 (46.4) |
| Hyperlipidemia | 24 (27.7) |
| Coronary artery disease | 18 (18.6) |
| Heart failure | 6 (6.2) |
| COPD | 12 (12.4) |
| LVEF [%] | 60.0 (55.0–62.0) |
| Hemoglobin [g/dL] | 13.8 (12.9–14.7) |
| Glucose [mg/dL] | 97.0 (90.0–111.0) |
| eGFR [mL/min] | 90.9 (77.5–103.8) |
| C-reactive protein [mg/L] | 1.8 (0.7–4.0) |
| NT-pro BNP [ng/L] | 105.0 (42.5–240.0) |
| Vaccination against COVID-19 | 74 (76.3) |
| Pre | Post | p | |
|---|---|---|---|
| Body composition | |||
| Weight (kg) | 78.3 (67.8–98.9) | 79.2 (68.2–92.4) | 0.6809 |
| BMI (kg/m2) | 27.4 (24.5–30.9) | 27.6 (24.6–30.7) | 0.5114 |
| Waist circumference (cm) | 94.0 (88.0–105.0) | 93.0 (88.0–107.0) | 0.0008 |
| Abdominal fatty tissued mass (kg) | 2.8 (1.9–3.9) | 2.5 (1.6–3.7) | 0.0086 |
| Skeletal muscle mass (kg) | 23.2 (18.6–29.3) | 24.2 (19.0–30.5) | 0.0104 |
| Fat-free body mass (kg) | 50.7 (42.0–62.0) | 51.7 (42.6–63.3) | 0.2428 |
| Fat-free body mass ratio (%) | 65.9 (59.4–70.8) | 66.3 (57.5–71.6) | 0.3916 |
| Body fat mass (kg) | 27.5 (19.6–32.9) | 27.7 (19.9–33.3) | 0.8296 |
| Body fat mass ratio (%) | 34.0 (29.2–40.6) | 33.7 (28.8–42.5) | 0.4471 |
| Body water (kg) | 37.5 (31.5–45.6) | 38.2 (31.7–46.3) | 0.3677 |
| Body water ratio (%) | 48.6 (43.1–51.8) | 48.8 (43.4–53.0) | 0.2394 |
| Extracellular body water (kg) | 17.0 (14.8–20.2) | 16.9 (14.6–20.4) | 0.2228 |
| Extracellular body water ratio (%) | 21.7 (20.1–23.1) | 21.5 (20.4–23.1) | 0.3710 |
| Hydration (%) | 84.2 (77.0–90.9) | 80.3 (76.4–89.7) | 0.0001 |
| Phase angle | 4.8 (4.4–5.2) | 5.0 (4.6–5.4) | <0.0001 |
| CPET | |||
| VO2peak (mL/kg/min) | 18.0 (15.0–18.5) | 18.0 (15.5–20.0) | 0.7364 |
| Predicted VO2peak (%) | 79.5 (70.5–93.0) | 81.0 (72.0–92.5) | 0.8563 |
| VO2peak/breathing frequencypeak | 29.5 (26.0–35.5) | 29.5 (25.5–33.5) | 0.8563 |
| Predicted VO2peak/breathing Frequencypeak (%) | 100.5 (86.5–124.5) | 101.5 (89.5–114) | 0.3803 |
| VE/VCO2 slope | 29.4 (27.6–32.3) | 29.2 (24.7–33.5) | 0.0806 |
| OUES slope | 2.05 (1.4–2.35) | 2.1 (1.6–2.5) | 0.8512 |
| Predicted AT (%) | 50.0 (42.0–59.0) | 50 (43.0–60.0) | 0.9935 |
| Pre | Post | p | |
|---|---|---|---|
| Borg scale | 3 (3–5) | 2 (1–3) | <0.0001 |
| mMRC | 2 (2–2) | 1 (0–2) | <0.0001 |
| MFIS | 37.0 (26.0–51.0) | 27.0 (20.0–36.5) | <0.0001 |
| 6MWT | 320 (290–380) | 382.5 (331.5–435.0) | <0.0001 |
| 30CST | 13 (10–16) | 16 (14–20) | <0.0001 |
| SPPB | 14 (13–15) | 16 (14–16) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostrowska, M.; Rzepka-Cholasińska, A.; Pietrzykowski, Ł.; Michalski, P.; Kosobucka-Ozdoba, A.; Jasiewicz, M.; Kasprzak, M.; Kryś, J.; Kubica, A. Effects of Multidisciplinary Rehabilitation Program in Patients with Long COVID-19: Post-COVID-19 Rehabilitation (PCR SIRIO 8) Study. J. Clin. Med. 2023, 12, 420. https://doi.org/10.3390/jcm12020420
Ostrowska M, Rzepka-Cholasińska A, Pietrzykowski Ł, Michalski P, Kosobucka-Ozdoba A, Jasiewicz M, Kasprzak M, Kryś J, Kubica A. Effects of Multidisciplinary Rehabilitation Program in Patients with Long COVID-19: Post-COVID-19 Rehabilitation (PCR SIRIO 8) Study. Journal of Clinical Medicine. 2023; 12(2):420. https://doi.org/10.3390/jcm12020420
Chicago/Turabian StyleOstrowska, Małgorzata, Alicja Rzepka-Cholasińska, Łukasz Pietrzykowski, Piotr Michalski, Agata Kosobucka-Ozdoba, Małgorzata Jasiewicz, Michał Kasprzak, Jacek Kryś, and Aldona Kubica. 2023. "Effects of Multidisciplinary Rehabilitation Program in Patients with Long COVID-19: Post-COVID-19 Rehabilitation (PCR SIRIO 8) Study" Journal of Clinical Medicine 12, no. 2: 420. https://doi.org/10.3390/jcm12020420