
Breast Cancer Care Pathways for Women with Preexisting Severe Mental Disorders: Evidence of Disparities in France?
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Conceptual Framework
2.2. Setting
2.3. Study Design and Data Source
2.4. Study Population
2.5. Matching between Cases and Controls
2.6. Indicators of Cancer Care Pathways and Mortality
2.7. Adjustment for Covariates
2.8. Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Global Cancer Care Received According to SMI Status
3.3. Indicators of the Quality of Cancer Care Pathways According to SMI Status
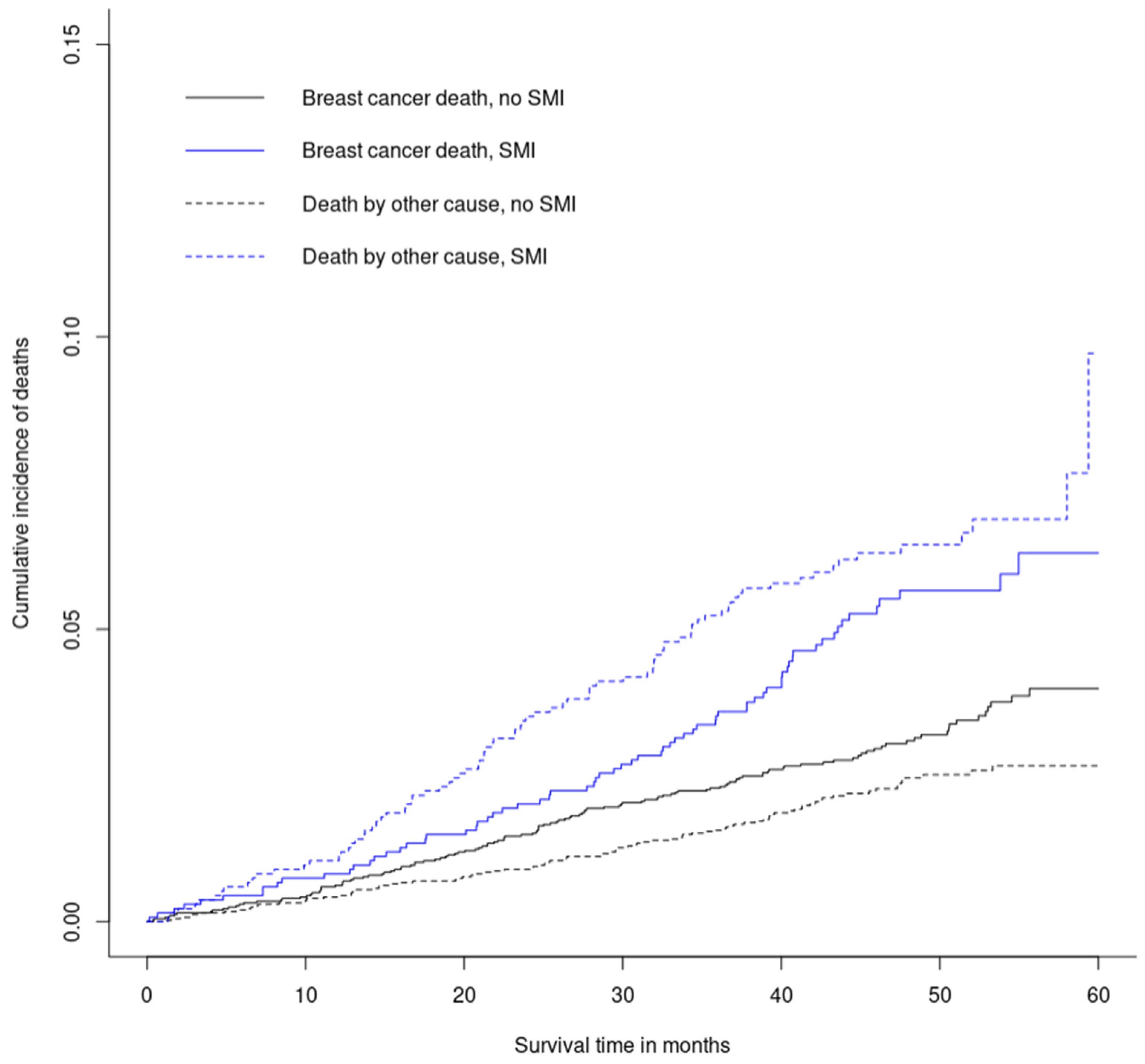
3.4. Mortality Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleury, M.J.; Grenier, G. Etat de Situation Sur La Santé Mentale Au Québec et Réponse Du Système de Santé et Des Services Sociaux; Gouvernement du Québec: Québec, QC, Canada, 2012. [Google Scholar]
- Baldwin, J.A. Schizophrenia and Physical Disease. Psychol. Med. 1979, 9, 611–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, D.; Kisely, S.; Pais, J. The Epidemiology of Excess Mortality in People with Mental Illness. Can. J. Psychiatry 2010, 55, 752–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, S.C.; Bland, R.C. Mortality in a Cohort of Patients with Schizophrenia: A Record Linkage Study. Can. J. Psychiatry 1991, 36, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of All-Cause and Suicide Mortality in Mental Disorders: A Meta-Review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Thornicroft, G. Physical Health Disparities and Mental Illness: The Scandal of Premature Mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef] [Green Version]
- Wahlbeck, K.; Westman, J.; Nordentoft, M.; Gissler, M.; Laursen, T.M. Outcomes of Nordic Mental Health Systems: Life Expectancy of Patients with Mental Disorders. Br. J. Psychiatry 2011, 199, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandré, C.; Moreau, D.; Coldefy, M.; Ben Dridi, I.; Morel, S. Surmortalite des personnes vivant avec un trouble psychique: Enseignements de la litterature et perspectives. Sante Publique 2022, 34, 613–619. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, A.; Labad, J.; Seeman, M.V. Schizophrenia and Cancer. Curr. Opin. Support. Palliat. Care 2020, 14, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Coldefy, M.; Gandré, C. Persons with Severe Mental Disorders: Life Expectancy Is Greatly Reduced and Premature Mortality Has Quadrupled. Questions D’économie de la Santé 2018, 237, 1–7. [Google Scholar]
- Kisely, S.; Crowe, E.; Lawrence, D. Cancer-Related Mortality in People with Mental Illness. JAMA Psychiatry 2013, 70, 209–217. [Google Scholar] [CrossRef] [Green Version]
- de Mooij, L.D.; Kikkert, M.; Theunissen, J.; Beekman, A.T.F.; de Haan, L.; Duurkoop, P.W.R.A.; Van, H.L.; Dekker, J.J.M. Dying Too Soon: Excess Mortality in Severe Mental Illness. Front. Psychiatry 2019, 10, 855. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Küstner, B.; Guzman-Parra, J.; Pardo, Y.; Sanchidrián, Y.; Díaz-Ruiz, S.; Mayoral-Cleries, F. Excess Mortality in Patients with Schizophrenia Spectrum Disorders in Malaga (Spain): A Cohort Study. Epidemiol. Psychiatr. Sci. 2021, 30, e11. [Google Scholar] [CrossRef] [PubMed]
- Lichtermann, D.; Ekelund, J.; Pukkala, E.; Tanskanen, A.; Lönnqvist, J. Incidence of Cancer among Persons with Schizophrenia and Their Relatives. Arch. Gen. Psychiatry 2001, 58, 573–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinty, E.E.; Zhang, Y.; Guallar, E.; Ford, D.E.; Steinwachs, D.; Dixon, L.B.; Keating, N.L.; Daumit, G.L. Cancer Incidence in a Sample of Maryland Residents with Serious Mental Illness. Psychiatr. Serv. 2012, 63, 714–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anmella, G.; Fico, G.; Lotfaliany, M.; Hidalgo-Mazzei, D.; Soto-Angona, Ó.; Giménez-Palomo, A.; Amoretti, S.; Murru, A.; Radua, J.; Solanes, A.; et al. Risk of Cancer in Bipolar Disorder and the Potential Role of Lithium: International Collaborative Systematic Review and Meta-Analyses. Neurosci. Biobehav. Rev. 2021, 126, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-H.; Tsai, S.-J.; Su, T.-P.; Li, C.-T.; Lin, W.-C.; Cheng, C.-M.; Chen, T.-J.; Bai, Y.-M. Cancer Risk in Patients with Bipolar Disorder and Unaffected Siblings of Such Patients: A Nationwide Population-Based Study. Int. J. Cancer 2022, 150, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Dembling, B.; Schorling, J. The Association between Schizophrenia and Cancer: A Population-Based Mortality Study. Schizophr. Res. 2002, 57, 139–146. [Google Scholar] [CrossRef]
- Dalton, S.O.; Mellemkjaer, L.; Thomassen, L.; Mortensen, P.B.; Johansen, C. Risk for Cancer in a Cohort of Patients Hospitalized for Schizophrenia in Denmark, 1969-1993. Schizophr. Res. 2005, 75, 315–324. [Google Scholar] [CrossRef]
- Pettersson, D.; Gissler, M.; Hällgren, J.; Ösby, U.; Westman, J.; Bobo, W.V. The Overall and Sex- and Age-Group Specific Incidence Rates of Cancer in People with Schizophrenia: A Population-Based Cohort Study. Epidemiol. Psychiatr. Sci. 2020, 29, e132. [Google Scholar] [CrossRef]
- Solmi, M.; Firth, J.; Miola, A.; Fornaro, M.; Frison, E.; Fusar-Poli, P.; Dragioti, E.; Shin, J.I.; Carvalho, A.F.; Stubbs, B.; et al. Disparities in Cancer Screening in People with Mental Illness across the World versus the General Population: Prevalence and Comparative Meta-Analysis Including 4 717 839 People. Lancet Psychiatry 2020, 7, 52–63. [Google Scholar] [CrossRef]
- Hwong, A.; Wang, K.; Bent, S.; Mangurian, C. Breast Cancer Screening in Women With Schizophrenia: A Systematic Review and Meta-Analysis. Psychiatr. Serv. 2020, 71, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Salas, S.; Pauly, V.; Baumstarck, K.; Bernard, C.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Auquier, P.; Boyer, L. End-of-Life Care among Patients with Schizophrenia and Cancer: A Population-Based Cohort Study from the French National Hospital Database. Lancet Public Health 2019, 4, e583–e591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fond, G.; Baumstarck, K.; Auquier, P.; Fernandes, S.; Pauly, V.; Bernard, C.; Orleans, V.; Llorca, P.-M.; Lançon, C.; Salas, S.; et al. Recurrent Major Depressive Disorder’s Impact on End-of-Life Care of Cancer: A Nationwide Study. J. Affect. Disord. 2020, 263, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Pauly, V.; Duba, A.; Salas, S.; Viprey, M.; Baumstarck, K.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Auquier, P.; et al. End of Life Breast Cancer Care in Women with Severe Mental Illnesses. Sci. Rep. 2021, 11, 10167. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Baumstarck, K.; Auquier, P.; Pauly, V.; Bernard, C.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Salas, S.; Boyer, L. End-of-Life Care Among Patients With Bipolar Disorder and Cancer: A Nationwide Cohort Study. Psychosom. Med. 2020, 82, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Viprey, M.; Pauly, V.; Salas, S.; Baumstarck, K.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Auquier, P.; Boyer, L.; Fond, G. Palliative and High-Intensity End-of-Life Care in Schizophrenia Patients with Lung Cancer: Results from a French National Population-Based Study. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 1571–1578. [Google Scholar] [CrossRef]
- Ishikawa, H.; Yasunaga, H.; Matsui, H.; Fushimi, K.; Kawakami, N. Differences in Cancer Stage, Treatment and in-Hospital Mortality between Patients with and without Schizophrenia: Retrospective Matched-Pair Cohort Study. Br. J. Psychiatry 2016, 208, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Kaneshiro, K.; Kubo, M.; Taniguchi, M.; Yamada, M.; Sadakari, Y.; Kai, M.; Tsutsumi, C.; Tsukamoto, T.; Yoshida, N.; Tanaka, M.; et al. Current Status and Problems of Breast Cancer Treatment with Schizophrenia. Clin. Breast Cancer 2022, 22, e399–e406. [Google Scholar] [CrossRef]
- Ahlgrén-Rimpiläinen, A.J.; Arffman, M.; Suvisaari, J.; Manderbacka, K.; Lumme, S.; Keskimäki, I.; Huovinen, R.; Pukkala, E. Excess Mortality from Breast Cancer in Female Breast Cancer Patients with Severe Mental Illness. Psychiatry Res. 2020, 286, 112801. [Google Scholar] [CrossRef] [PubMed]
- Mahar, A.L.; Kurdyak, P.; Hanna, T.P.; Coburn, N.G.; Groome, P.A. The Effect of a Severe Psychiatric Illness on Colorectal Cancer Treatment and Survival: A Population-Based Retrospective Cohort Study. PLoS ONE 2020, 15, e0235409. [Google Scholar] [CrossRef]
- Launders, N.; Scolamiero, L.; Osborn, D.; Hayes, J. Cancer Rates and Mortality in People with Severe Mental Illness: Further Evidence of Lack of Parity. Schizophr. Res. 2022, 246, 260–267. [Google Scholar] [CrossRef]
- Irwin, K.E.; Park, E.R.; Shin, J.A.; Fields, L.E.; Jacobs, J.M.; Greer, J.A.; Taylor, J.B.; Taghian, A.G.; Freudenreich, O.; Ryan, D.P.; et al. Predictors of Disruptions in Breast Cancer Care for Individuals with Schizophrenia. Oncologist 2017, 22, 1374–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, L.; Stivanello, E.; Belvederi Murri, M.; Perlangeli, V.; Pandolfi, P.; Carnevali, F.; Caruso, R.; Saponaro, A.; Ferri, M.; Sanza, M.; et al. Mortality from Cancer in People with Severe Mental Disorders in Emilia Romagna Region, Italy. Psychooncology 2021, 30, 2039–2051. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.L.; Hou, S.S.-Y.; Lee-Tauler, S.Y.; Progovac, A.M.; Samson, F.; Sanchez, M.J. A Review of Mental Health and Mental Health Care Disparities Research: 2011–2014. Med. Care Res. Rev. 2018, 76, 1077558718780592. [Google Scholar] [CrossRef] [PubMed]
- Inca. 2021–2030 France Ten-Year Cancer-Control Strategy. In 2021–2025 Roadmap; Institut National du Cancer: Boulogne Billancourt, France, 2021. [Google Scholar]
- INCA. Panorama des Cancers en France; Institut National du Cancer: Boulogne Billancourt, France, 2022. [Google Scholar]
- HCAAM. Organiser La Médecine Spécialisée et Le Second Recours: Une Pièce Essentielle de La Transformation de Notre Système de Santé; Haut Conseil pour l’Avenir de l’Assurance Maladie: Paris, France, 2020. [Google Scholar]
- OECD. Health at a Glance 2021: OECD Indicators; Organisation for Economic Cooperation and Development: Paris, France, 2021. [Google Scholar]
- CNAM. Complémentaire Santé. Available online: https://www.ameli.fr/val-de-marne/assure/droits-demarches/difficultes-acces-droits-soins/complementaire-sante (accessed on 28 May 2022).
- INCA. Dépistage des Cancers du Sein—S’informer et Décider; Institut National du Cancer: Boulogne Billancourt, France, 2017. [Google Scholar]
- Or, Z.; Roccoco, E.; Touré, M.; Bonastre, J. Impact of Competition Versus Centralisation of Hospital Care on Process Quality: A Multilevel Analysis of Breast Cancer Surgery in France. Int. J. Health Policy Manag. 2022, 11, 459–469. [Google Scholar] [CrossRef] [PubMed]
- DREES. Panoramas de La Drees. Les Établissements de Santé—Édition 2021; Direction de la recherche, des études, de l’évaluation et des statistiques: Paris, France, 2021. [Google Scholar]
- CNAM. Améliorer La Qualité Du Système de Santé et Maitriser Les Dépenses: Propositions de l’Assurance Maladie Pour 2022; Caisse Nationale d’Assurance Maladie: Paris, France, 2021. [Google Scholar]
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Ménager, C.; Rachas, A.; de Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a National Administrative Database to Guide Public Decisions: From the Système National d’information Interrégimes de l’Assurance Maladie (SNIIRAM) to the Système National Des Données de Santé (SNDS) in France. Rev. D’épidémiol. Sante Publique 2017, 65, S149–S167. [Google Scholar] [CrossRef]
- Health Data Hub Documentation Collaborative du SNDS. Available online: https://gitlab.com/healthdatahub/documentation-snds/-/blob/master/introduction/01-snds.md (accessed on 1 June 2022).
- Caisse Nationale d’Assurance Maladie. Méthode de Repérage des Pathologies et d’Affectation des Dépenses aux Pathologies. Available online: https://www.ameli.fr/l-assurance-maladie/statistiques-et-publications/etudes-en-sante-publique/cartographie-des-pathologies-et-des-depenses/methode.php (accessed on 6 March 2020).
- Légifrance Décret N° 2021-848 Du 29 Juin 2021 Relatif Au Traitement de Données à Caractère Personnel Dénommé « Système National Des Données de Santé ». Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043715694 (accessed on 1 June 2022).
- Bellass, S.; Taylor, J.; Han, L.; Prady, S.L.; Shiers, D.; Jacobs, R.; Holt, R.I.G.; Radford, J.; Gilbody, S.; Hewitt, C.; et al. Exploring Severe Mental Illness and Diabetes: Protocol for a Longitudinal, Observational, and Qualitative Mixed Methods Study. JMIR Res. Protoc. 2019, 8, e13407. [Google Scholar] [CrossRef]
- Barley, E.A.; Borschmann, R.D.; Walters, P.; Tylee, A. Interventions to Encourage Uptake of Cancer Screening for People with Severe Mental Illness. Cochrane Database Syst. Rev. 2016, 9, CD009641. [Google Scholar] [CrossRef]
- Cnam Méthodologie Médicale de La Cartographie Des Pathologies et Des Dépenses; Version G7 (Années 2012 à 2018); Caisse Nationale d’Assurance Maladie: Paris, France, 2020.
- INCA. Cancer du Sein: Indicateurs de Qualité et de Sécurité des Soins; Institut National du Cancer: Boulogne Billancourt, France, 2019. [Google Scholar]
- Houzard, S.; Courtois, E.; Le Bihan Benjamin, C.; Erbault, M.; Arnould, L.; Barranger, E.; Coussy, F.; Couturaud, B.; Cutuli, B.; de Cremoux, P.; et al. Monitoring Breast Cancer Care Quality at National and Local Level Using the French National Cancer Cohort. Clin. Breast Cancer 2022, 22, e832–e841. [Google Scholar] [CrossRef]
- Forrest, L.F.; Adams, J.; Wareham, H.; Rubin, G.; White, M. Socioeconomic Inequalities in Lung Cancer Treatment: Systematic Review and Meta-Analysis. PLoS Med. 2013, 10, e1001376. [Google Scholar] [CrossRef] [Green Version]
- Loretti, A. La Fabrique des Inégalités Sociales de Santé; Presses de l’Ecole des Hautes études en Santé Publique: Rennes, France, 2021. [Google Scholar]
- Biscond, M.; Guimbaud, R.; Digue, L.; Cirilo-Cassaigne, I.; Bousser, V.; Oum-Sack, E.; Goddard, J.; Bauvin, E.; Delpierre, C.; Grosclaude, P.; et al. How Does Comorbidity Affect Colon Cancer Patients’ Care Trajectory? Results from the French EvaCCoR Cohort Study. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101422. [Google Scholar] [CrossRef] [PubMed]
- Morishima, T.; Okawa, S.; Koyama, S.; Nakata, K.; Tabuchi, T.; Miyashiro, I. Between-Hospital Variations in 3-Year Survival among Patients with Newly Diagnosed Gastric, Colorectal, and Lung Cancer. Sci. Rep. 2022, 12, 7134. [Google Scholar] [CrossRef] [PubMed]
- Rey, G.; Jougla, E.; Fouillet, A.; Hémon, D. Ecological Association between a Deprivation Index and Mortality in France over the Period 1997–2001: Variations with Spatial Scale, Degree of Urbanicity, Age, Gender and Cause of Death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantinou, P.; Tuppin, P.; Fagot-Campagna, A.; Gastaldi-Ménager, C.; Schellevis, F.G.; Pelletier-Fleury, N. Two Morbidity Indices Developed in a Nationwide Population Permitted Performant Outcome-Specific Severity Adjustment. J. Clin. Epidemiol. 2018, 103, 60–70. [Google Scholar] [CrossRef] [Green Version]
- CNAM. Les Indices de Morbidité MRMI et ERMI Élaborés à Partir Des Données de La Cartographie Des Pathologies et Des Dépenses; Caisse Nationale d’Assurance Maladie: Paris, France, 2021. [Google Scholar]
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Yaffe, M.J.; Mainprize, J.G. Overdetection of Breast Cancer. Curr. Oncol. 2022, 29, 3894–3910. [Google Scholar] [CrossRef]
- Peterson, L.G.; Popkin, M.K. Neuropsychiatric Effects of Chemotherapeutic Agents for Cancer. Psychosomatics 1980, 21, 141–153. [Google Scholar] [CrossRef]
- Yap, K.y.-L.; Tay, W.L.; Chui, W.K.; Chan, A. Clinically Relevant Drug Interactions between Anticancer Drugs and Psychotropic Agents. Eur. J. Cancer Care 2011, 20, 6–32. [Google Scholar] [CrossRef]
- Sharma, A.; Ngan, S.; Nandoskar, A.; Lowdell, C.; Lewis, J.S.; Hogben, K.; Coombes, R.C.; Stebbing, J. Schizophrenia Does Not Adversely Affect the Treatment of Women with Breast Cancer: A Cohort Study. Breast 2010, 19, 410–412. [Google Scholar] [CrossRef]
- Forrest, L.F.; White, M.; Rubin, G.; Adams, J. The Role of Patient, Tumour and System Factors in Socioeconomic Inequalities in Lung Cancer Treatment: Population-Based Study. Br. J. Cancer 2014, 111, 608–618. [Google Scholar] [CrossRef] [Green Version]
- De Wild, S.R.; de Munck, L.; Simons, J.M.; Verloop, J.; van Dalen, T.; Elkhuizen, P.H.M.; Houben, R.M.A.; van Leeuwen, A.E.; Linn, S.C.; Pijnappel, R.M.; et al. De-Escalation of Radiotherapy after Primary Chemotherapy in CT1–2N1 Breast Cancer (RAPCHEM; BOOG 2010-03): 5-Year Follow-up Results of a Dutch, Prospective, Registry Study. Lancet Oncol. 2022, 23, 1201–1210. [Google Scholar] [CrossRef]
- Chua, B.H.; Link, E.K.; Kunkler, I.H.; Whelan, T.J.; Westenberg, A.H.; Gruber, G.; Bryant, G.; Ahern, V.; Purohit, K.; Graham, P.H.; et al. Radiation Doses and Fractionation Schedules in Non-Low-Risk Ductal Carcinoma in Situ in the Breast (BIG 3-07/TROG 07.01): A Randomised, Factorial, Multicentre, Open-Label, Phase 3 Study. Lancet 2022, 400, 431–440. [Google Scholar] [CrossRef]
- Céspedes, P.; Sánchez-Martínez, V.; Lera-Calatayud, G.; Vila-Candel, R.; Cauli, O.; Buigues, C. Delay in the Diagnosis of Breast and Colorectal Cancer in People with Severe Mental Disorders. Cancer Nurs. 2020, 43, E356–E362. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.; Corveleyn, A.; Park, E.; Irwin, K. Challenges, Rewards and Lessons Learned from Family and Community Caregivers of Individuals with Serious Mental Illness and Cancer. 2022. Available online: https://assets.researchsquare.com/files/rs-2241067/v1/b5f6f038-4c93-4226-a2f7-6edf5ae05bec.pdf?c=1668465661 (accessed on 19 December 2022).
- Levin, J.B.; Aebi, M.E.; Tatsuoka, C.; Cassidy, K.A.; Sajatovic, M. Adherence to Psychotropic and Nonpsychotropic Medication Among Patients With Bipolar Disorder and General Medical Conditions. Psychiatr. Serv. 2016, 67, 342–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, K.E.; Ko, N.; Walsh, E.P.; Decker, V.; Arrillaga-Romany, I.; Plotkin, S.R.; Franas, J.; Gorton, E.; Moy, B. Developing a Virtual Equity Hub: Adapting the Tumor Board Model for Equity in Cancer Care. Oncologist 2022, 27, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Onwumere, J.; Stubbs, B.; Stirling, M.; Shiers, D.; Gaughran, F.; Rice, A.S.; Williams, A.C.d.C.; Scott, W. Pain Management in People with Severe Mental Illness: An Agenda for Progress. Pain 2022, 163, 1653–1660. [Google Scholar] [CrossRef]
- MoH Instruction No DGOS/R4/DGCS/3B/DGS/P4/2018/137 du 5 Juin 2018 Relative Aux Projets Territoriaux de Santé Mentale; Ministry in Charge of Health: Paris, France, 2018.
- Evans, C.K.; Sabatier, R.; Chinot, O.; Loschi, A.; Arnaud, S.; Mellinas, M. Development of advanced practice nursing in oncology and hematology-oncology in France: Early status report. Bull. Cancer 2022, 109, 139–150. [Google Scholar] [CrossRef]
- Hervieux, E. Place de l’IPA Mention Pathologies Chroniques Stabilisées En Secteur Psychiatrique. Rev. Prat. Av. 2021, 2, 93–97. [Google Scholar]


{kind=link}
| Characteristic | Women with SMI (n = 1581) | Women without SMI (n = 96,179) |
|---|---|---|
| Mean (±SD) or n (%) | ||
| Demographic and socioeconomic characteristics | ||
| Age | 60.84 (±11.92) | 60.68 (±13.74) |
| Inclusion in the scheme covering healthcare costs for low-income groups (CMU-C) * | 70 (4.43) | 3256 (3.39) |
| Missing values | 1 (0.06) | 16 (0.02) |
| Inclusion in the scheme providing allowances for purchasing complementary health insurance (ACS) * | 176 (11.13) | 2124 (2.21) |
| Missing values | 1 (0.06) | 16 (0.02) |
| Quintile of community-level deprivation index (FDep) * | ||
| 1st quintile (least deprived) | 277 (17.52) | 19,159 (19.92) |
| 2nd quintile | 267 (16.89) | 18,657 (19.40) |
| 3rd quintile | 403 (25.49) | 19,655 (20.44) |
| 4th quintile | 314 (19.86) | 18,396 (19.13) |
| 5th quintile (most deprived) | 267 (16.89) | 17,170 (17.85) |
| Missing values | 53 (3.35) | 3142 (3.27) |
| Residency in an overseas territory | 29 (1.83) | 1664 (1.73) |
| Missing values | 0 (0.00) | 68 (0.07) |
| Clinical characteristics | ||
| Non-metastatic invasive breast cancer | ||
| Invasive carcinoma with lymph node involvement | 293 (18.53) | 16,306 (16.95) |
| Invasive carcinoma without lymph node involvement | 1092 (69.07) | 67,658 (70.35) |
| Others | ||
| Ductal carcinoma in situ * | 37 (2.34) | 3109 (3.23) |
| Lobular carcinoma in situ | 4 (0.25) | 345 (0.36) |
| Carcinoma in situ of uncertain type | 18 (1.14) | 1296 (1.35) |
| Metastatic breast cancer * | 126 (7.97) | 6403 (6.66) |
| Tumor of uncertain malignant potential | 11 (0.70) | 1062 (1.10) |
| Comorbidity index * | 0.58 (±0.97) | 0.31 (±0.70) |
| Women with NMI Breast Cancer with Lymph Node Involvement | Women with NMI Breast Cancer without Lymph Node Involvement | Total of Women with NMI Breast Cancer | ||||||
|---|---|---|---|---|---|---|---|---|
| SMI (N = 263) | No SMI (N = 789) | SMI (N = 1083) | No SMI (N = 3249) | Univariate Analysis | Multivariable Analysis + | |||
| % ^ | OR (SMI vs. No SMI) | 95% CI | AOR (SMI vs. No SMI) | 95% CI | ||||
| Main diagnostic testsX | ||||||||
| Mammogram | 91.25 | 97.72 | 92.43 | 97.26 | 0.32 * | 0.24–0.42 | 0.38 * | 0.28–0.51 |
| Breast biopsy | 81.37 | 90.49 | 83.84 | 90.67 | 0.52 * | 0.44–0.62 | 0.56 * | 0.47–0.67 |
| Echography | 89.73 | 96.32 | 87.17 | 92.67 | 0.50 * | 0.41–0.62 | 0.58 * | 0.47–0.72 |
| MRI | 27.76 | 36.25 | 23.27 | 29.70 | 0.71 * | 0.62–0.81 | 0.76 * | 0.67–0.87 |
| Number of main diagnostic tests ^ | 2.90 (0.96) | 3.21 (0.70) | 2.87 (0.92) | 3.10 (0.72) | 0.92 * | 0.90–0.94 | 0.93 * | 0.92–0.95 |
| Mammogram + breast biopsy (recommended combination) | 79.09 | 89.48 | 81.26 | 89.54 | 0.49 * | 0.42–0.58 | 0.54 * | 0.46–0.64 |
| Treatment | ||||||||
| Neoadjuvant chemotherapy | 16.73 | 12.29 | 6.09 | 6.09 | 1.13 | 0.91–1.40 | 1.22 | 0.97–1.54 |
| Lumpectomy | 53.99 | 68.57 | 72.95 | 76.58 | 0.75 * | 0.66–0.85 | 0.82 * | 0.70–0.95 |
| Mastectomy | 54.75 | 37.26 | 26.04 | 22.19 | 1.38 * | 1.21–1.57 | 1.38 * | 1.20–1.58 |
| Adjuvant chemotherapy | 58.94 | 66.03 | 21.79 | 26.75 | 0.78 * | 0.69–0.88 | 0.80 * | 0.70–0.91 |
| Adjuvant radiotherapy | 88.59 | 93.79 | 74.33 | 77.75 | 0.80 * | 0.69–0.92 | 0.87 * | 0.75–0.98 |
| Hormone therapy | 74.52 | 82.51 | 69.99 | 71.13 | 0.88 | 0.77–1.01 | 0.86 * | 0.75–0.99 |
| Type of treatment combination | ||||||||
| Operative only | 4.18 | 0.25 | 7.39 | 5.48 | 1.55 * | 1.19–2.02 | 1.47 * | 1.13–1.91 |
| Operative + radiotherapy | 3.42 | 1.14 | 12.28 | 11.97 | 1.08 | 0.88–1.32 | 1.14 | 0.93–1.41 |
| Of which lumpectomy only + radiotherapy | 0.76 | 0.89 | 11.54 | 11.45 | 1.01 | 0.81–1.24 | 1.08 | 0.87–1.34 |
| Operative + radiotherapy + chemo/hormone therapy | 84.41 | 91.38 | 61.03 | 65.28 | 0.80 * | 0.71–0.91 | 0.84 * | 0.74–0.96 |
| Operative + chemo/hormone therapy | 5.70 | 4.94 | 11.08 | 11.30 | 1.00 | 0.81–1.22 | 0.94 | 0.77–1.16 |
| No operation + any other form of treatment | 2.28 | 2.28 | 8.22 | 5.97 | 1.37 * | 1.09–1.72 | 1.06 | 0.61–1.81 |
| Type of Breast Cancer | Indicator of Cancer Care Quality | SMI% (n/d) | No SMI% (n/d) | Target Threshold | Alert Threshold | Univariate Analysis | Multivariable Analysis + | ||
|---|---|---|---|---|---|---|---|---|---|
| OR (SMI vs. No SMI) | 95% CI | AOR (SMI vs. No SMI) | 95% CI | ||||||
| Indicators of diagnosis (process) | |||||||||
| Proportion of women undergoing their first treatment within 6 weeks post-mammogram (Indicator 1) # | 39.1 (422/1079) | 46.5 (1659/3565) | ≥90% | <80% | 0.74 * | 0.64–0.84 | 0.75 * | 0.65–0.87 | |
| Proportion of women undergoing biopsy within 2 weeks post-mammogram (Indicator 2) # | 62.7 (677/1079) | 66.1 (2355/3565) | ≥90% | <80% | 0.87 * | 0.75–0.99 | 0.91 | 0.79–1.06 | |
| Proportion of women undergoing their first treatment within 4 weeks post-biopsy (Indicator 3) # | 34.8 (376/1079) | 41.5 (1479/3565) | ≥90% | <80% | 0.75 * | 0.65–0.86 | 0.78 * | 0.67–0.91 | |
| Proportion of women undergoing biopsy prior to first treatment (Indicator 4) ## | 87.8 (1080/1230) | 92.1 (3580/3886) | >98% | ≤95% | 0.61 * | 0.50–0.75 | 0.65 * | 0.52–0.80 | |
| Indicators of diagnosis and treatment (process) | |||||||||
| Proportion of women without lymph node involvement undergoing sentinel lymph node excision without axillary dissection (Indicator 5) | 24.3 (263/1083) | 26.2 (849/3245) | >95% | <90% | 0.91 | 0.77–1.06 | 0.82 * | 0.67–0.99 | |
| Indicators of treatment (process) | |||||||||
| Proportion of women undergoing radiotherapy after breast-conserving surgery (Indicator 6) | 91.8 (780/850) | 94.2 (2676/2840) | >95% | <90% | 0.68 * | 0.51–0.91 | 0.79 | 0.58–1.09 | |
| Proportion of women undergoing adjuvant radiotherapy within 12 weeks post-surgery (Indicator 7A) | 82.1 (536/653) | 85.0 (1659/1952) | >95% | <90% | 0.82 | 0.65–1.03 | 0.88 | 0.69–1.11 | |
| Proportion of women undergoing adjuvant chemotherapy within 6 weeks post-surgery (Indicator 7B) | 47.3 (185/391) | 50.6 (703/1390) | >90% | <85% | 0.87 | 0.70–1.09 | 0.86 | 0.69–1.08 | |
| Proportion of women undergoing radiotherapy within 6 weeks post-adjuvant chemotherapy (Indicator 8) | 74.9 (250/334) | 77.5 (907/1171) | >95% | <90% | 0.86 | 0.65–1.13 | 0.90 | 0.68–1.20 | |
| Indicators of treatment (outcomes) | |||||||||
| Proportion of women not treated with neoadjuvant chemotherapy undergoing breast reintervention (Indicator 9) | 17.0 (149/875) | 14.2 (405/2848) | <10% | >20% | 1.24 * | 1.01–1.52 | 1.22 | 0.99–1.49 | |
| Indicators of follow-up (process) | |||||||||
| Proportion of women who have had their first follow-up mammogram (Indicator 10) | 52.5 (604/1151) | 58.5 (2155/3682) | >98% | <95% | 0.78 * | 0.69–0.89 | 0.81 * | 0.71–0.93 | |
| Univariate Analysis | Main Multivariable Analysis + | Sensitivity Analyses + | |||||
|---|---|---|---|---|---|---|---|
| (1) | (2) | ||||||
| HR (SMI vs. No SMI) | 95% CI | aHR (SMI vs. No SMI) | 95% CI | aHR (SMI vs. No SMI) | 95% CI | aHR (SMI vs. No SMI) | 95% CI |
| 1.68 | 1.25–2.24 | 1.39 | 1.03–1.87 | 1.46 | 1.0–1.94 | 1.50 | 1.14–1.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seppänen, A.-V.; Daniel, F.; Houzard, S.; Le Bihan, C.; Coldefy, M.; Gandré, C. Breast Cancer Care Pathways for Women with Preexisting Severe Mental Disorders: Evidence of Disparities in France? J. Clin. Med. 2023, 12, 412. https://doi.org/10.3390/jcm12020412
Seppänen A-V, Daniel F, Houzard S, Le Bihan C, Coldefy M, Gandré C. Breast Cancer Care Pathways for Women with Preexisting Severe Mental Disorders: Evidence of Disparities in France? Journal of Clinical Medicine. 2023; 12(2):412. https://doi.org/10.3390/jcm12020412
Chicago/Turabian StyleSeppänen, Anna-Veera, Fabien Daniel, Sophie Houzard, Christine Le Bihan, Magali Coldefy, and Coralie Gandré. 2023. "Breast Cancer Care Pathways for Women with Preexisting Severe Mental Disorders: Evidence of Disparities in France?" Journal of Clinical Medicine 12, no. 2: 412. https://doi.org/10.3390/jcm12020412