
Beneficial Effects of Combined Use of Extracorporeal Membrane Oxygenation and Hypothermic Machine Perfusion in Porcine Donors after Cardiac Death for Liver Transplantation
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Procedures
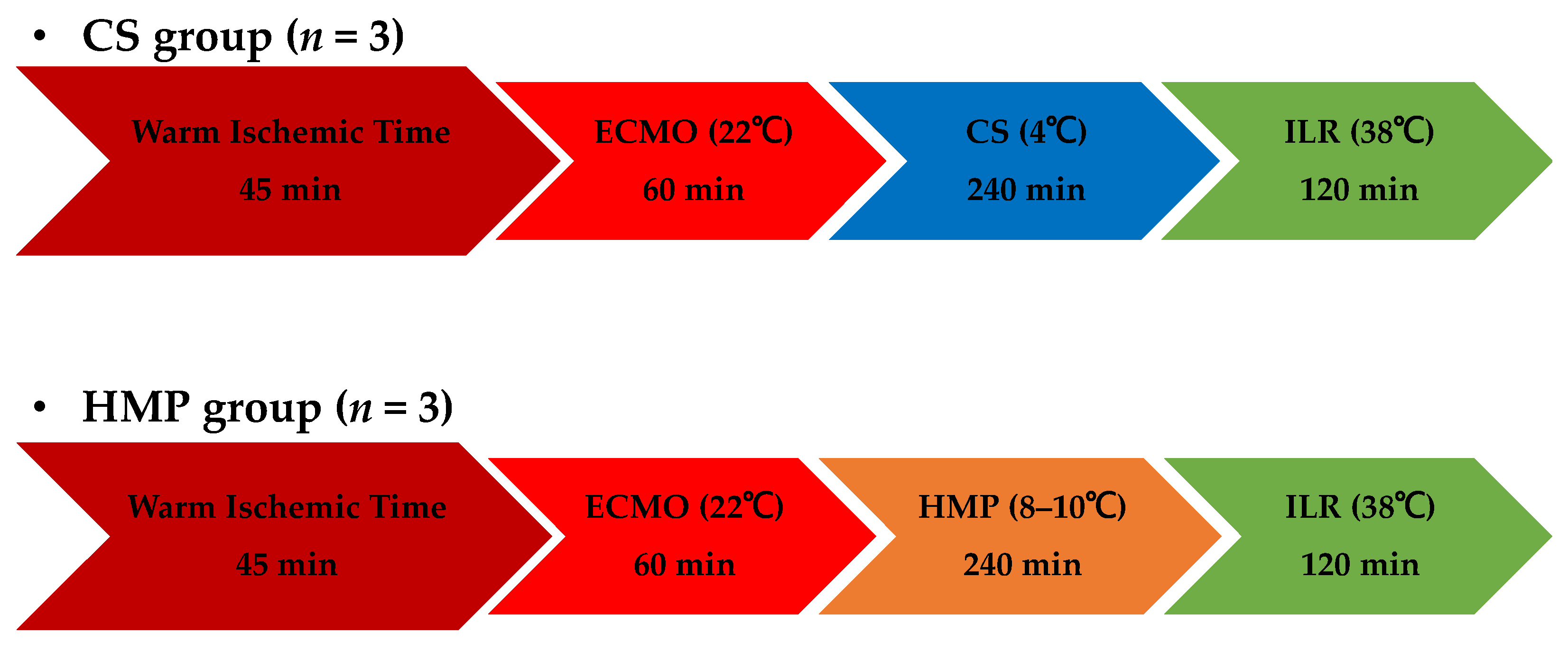
2.2. Experimental Design
2.3. Extracorporeal Membrane Oxygenation Protocol
2.4. Preservation Protocol
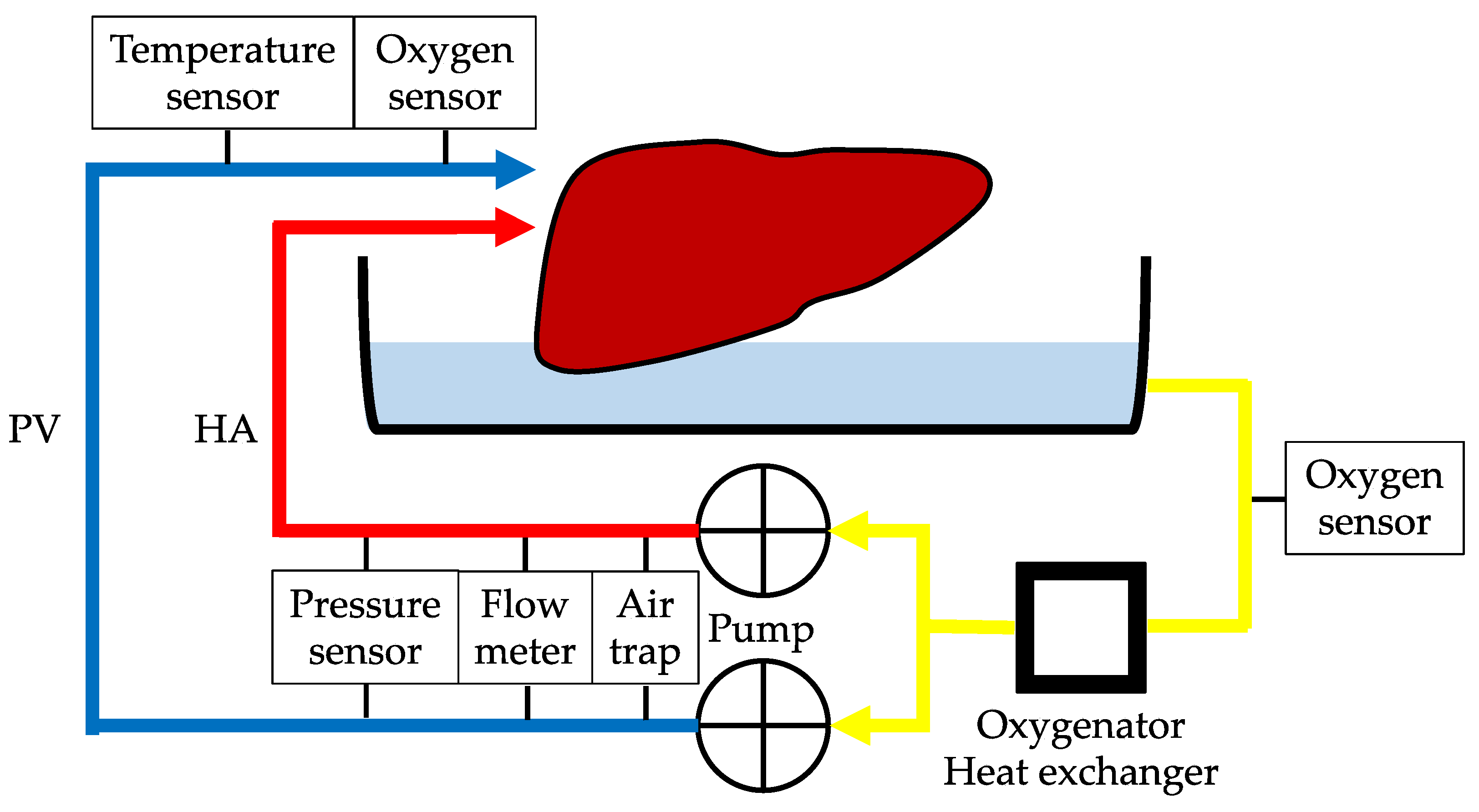
2.5. Isolated Liver Reperfusion
2.6. Primary Outcomes—Viability Assessment
2.7. Secondary Outcomes—Morphological Assessment
2.8. Statistical Analyses
3. Results
3.1. Laboratory Test Results
3.2. Hemodynamic Results
3.3. Morphological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blok, J.J.; Detry, O.; Putter, H.; Rogiers, X.; Porte, R.J.; van Hoek, B.; Pirenne, J.; Metselaar, H.J.; Lerut, J.P.; Ysebaert, D.K.; et al. Longterm results of liver transplantation from donation after circulatory death. Liver Transpl. 2016, 22, 1107–1114. [Google Scholar] [CrossRef]
- Kalisvaart, M.; de Haan, J.E.; Polak, W.G.; Metselaar, H.J.; Wijnhoven, B.P.L.; JNM, I.J.; de Jonge, J. Comparison of Postoperative Outcomes between Donation after Circulatory Death and Donation after Brain Death Liver Transplantation Using the Comprehensive Complication Index. Ann. Surg. 2017, 266, 772–778. [Google Scholar] [CrossRef]
- Laing, R.W.; Scalera, I.; Isaac, J.; Mergental, H.; Mirza, D.F.; Hodson, J.; Wilkin, R.J.; Perera, M.T.; Muiesan, P. Liver Transplantation Using Grafts from Donors after Circulatory Death: A Propensity Score-Matched Study From a Single Center. Am. J. Transplant. 2016, 16, 1795–1804. [Google Scholar] [CrossRef]
- Dutkowski, P.; Polak, W.G.; Muiesan, P.; Schlegel, A.; Verhoeven, C.J.; Scalera, I.; DeOliveira, M.L.; Kron, P.; Clavien, P.A. First Comparison of Hypothermic Oxygenated PErfusion Versus Static Cold Storage of Human Donation after Cardiac Death Liver Transplants: An International-Matched Case Analysis. Ann. Surg. 2015, 262, 764–770. [Google Scholar] [CrossRef]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; Garcia-Valdecasas, J.C.; Heaton, N.; et al. A randomized trial of normothermic preservation in liver transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Muller, X.; Kalisvaart, M.; Muellhaupt, B.; Perera, M.; Isaac, J.R.; Clavien, P.A.; Muiesan, P.; Dutkowski, P. Outcomes of DCD liver transplantation using organs treated by hypothermic oxygenated perfusion before implantation. J. Hepatol. 2019, 70, 50–57. [Google Scholar] [CrossRef]
- Muller, X.; Schlegel, A.; Wurdinger, M.; Wendt, M.; Kron, P.; Eshmuminov, D.; Mullhaupt, B.; Clavien, P.A.; Dutkowski, P. Can hypothermic oxygenated perfusion (HOPE) rescue futile DCD liver grafts? HPB 2019, 21, 1156–1165. [Google Scholar] [CrossRef]
- van Rijn, R.; Schurink, I.J.; de Vries, Y.; van den Berg, A.P.; Cortes Cerisuelo, M.; Darwish Murad, S.; Erdmann, J.I.; Gilbo, N.; de Haas, R.J.; Heaton, N.; et al. Hypothermic Machine Perfusion in Liver Transplantation—A Randomized Trial. N. Engl. J. Med. 2021, 384, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Weissenbacher, A.; Vrakas, G.; Nasralla, D.; Ceresa, C.D.L. The future of organ perfusion and re-conditioning. Transpl. Int. 2019, 32, 586–597. [Google Scholar] [CrossRef]
- Fondevila, C.; Hessheimer, A.J.; Ruiz, A.; Calatayud, D.; Ferrer, J.; Charco, R.; Fuster, J.; Navasa, M.; Rimola, A.; Taura, P.; et al. Liver transplant using donors after unexpected cardiac death: Novel preservation protocol and acceptance criteria. Am. J. Transplant. 2007, 7, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.J.E.; Kosmoliaptsis, V.; Pley, C.; Randle, L.; Fear, C.; Crick, K.; Gimson, A.E.; Allison, M.; Upponi, S.; Brais, R.; et al. Observations on the ex situ perfusion of livers for transplantation. Am. J. Transplant. 2018, 18, 2005–2020. [Google Scholar] [CrossRef]
- Hessheimer, A.J.; Coll, E.; Torres, F.; Ruiz, P.; Gastaca, M.; Rivas, J.I.; Gomez, M.; Sanchez, B.; Santoyo, J.; Ramirez, P.; et al. Normothermic regional perfusion vs. super-rapid recovery in controlled donation after circulatory death liver transplantation. J. Hepatol. 2019, 70, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Lomero, M.; Gardiner, D.; Coll, E.; Haase-Kromwijk, B.; Procaccio, F.; Immer, F.; Gabbasova, L.; Antoine, C.; Jushinskis, J.; Lynch, N.; et al. Donation after circulatory death today: An updated overview of the European landscape. Transpl. Int. 2020, 33, 76–88. [Google Scholar] [CrossRef]
- Matsuno, N.; Obara, H.; Watanabe, R.; Iwata, S.; Kono, S.; Fujiyama, M.; Hirano, T.; Kanazawa, H.; Enosawa, S. Rewarming preservation by organ perfusion system for donation after cardiac death liver grafts in pigs. Transplant. Proc. 2014, 46, 1095–1098. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Wang, F.; Zhang, Y.; Li, C.; Xia, C.; Chen, H.; Lu, X.; Liu, F. Comparison of hematologic and biochemical reference values in specific-pathogen-free 1-month-old Yorkshire pigs and Yorkshire-Landrace crossbred pigs. Can. J. Vet. Res. 2019, 83, 285–290. [Google Scholar]
- Li, C.; Wang, F.; Li, R.; Ishfaq, M.; Chen, H.; Liu, F.; Liu, Y. Hematologic and biochemical reference intervals for 1-month-old specific-pathogen-free Landrace pigs. Vet. Clin. Pathol. 2021, 50, 76–80. [Google Scholar] [CrossRef]
- Garcia-Valdecasas, J.C.; Tabet, J.; Valero, R.; Taura, P.; Rull, R.; Garcia, F.; Montserrat, E.; Gonzalez, F.X.; Ordi, J.; Beltran, J.; et al. Liver conditioning after cardiac arrest: The use of normothermic recirculation in an experimental animal model. Transpl. Int. 1998, 11, 424–432. [Google Scholar] [CrossRef]
- Net, M.; Valero, R.; Almenara, R.; Barros, P.; Capdevila, L.; Lopez-Boado, M.A.; Ruiz, A.; Sanchez-Crivaro, F.; Miquel, R.; Deulofeu, R.; et al. The effect of normothermic recirculation is mediated by ischemic preconditioning in NHBD liver transplantation. Am. J. Transplant. 2005, 5, 2385–2392. [Google Scholar] [CrossRef]
- Fondevila, C.; Hessheimer, A.J.; Maathuis, M.H.; Munoz, J.; Taura, P.; Calatayud, D.; Leuvenink, H.; Rimola, A.; Ploeg, R.J.; Garcia-Valdecasas, J.C. Superior preservation of DCD livers with continuous normothermic perfusion. Ann. Surg. 2011, 254, 1000–1007. [Google Scholar] [CrossRef]
- Imber, C.J.; St Peter, S.D.; Lopez de Cenarruzabeitia, I.; Pigott, D.; James, T.; Taylor, R.; McGuire, J.; Hughes, D.; Butler, A.; Rees, M.; et al. Advantages of normothermic perfusion over cold storage in liver preservation. Transplantation 2002, 73, 701–709. [Google Scholar] [CrossRef]
- Seelhammer, T.G.; Bohman, J.K.; Schulte, P.J.; Hanson, A.C.; Aganga, D.O. Comparison of Bivalirudin Versus Heparin for Maintenance Systemic Anticoagulation during Adult and Pediatric Extracorporeal Membrane Oxygenation. Crit. Care Med. 2021, 49, 1481–1492. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, F.; Curro, J.M.; La Via, L.; Dezio, V.; Martucci, G.; Brancati, S.; Murabito, P.; Pappalardo, F.; Astuto, M. Use of nafamostat mesilate for anticoagulation during extracorporeal membrane oxygenation: A systematic review. Artif. Organs 2022, 46, 2371–2381. [Google Scholar] [CrossRef]
- Vairetti, M.; Ferrigno, A.; Carlucci, F.; Tabucchi, A.; Rizzo, V.; Boncompagni, E.; Neri, D.; Gringeri, E.; Freitas, I.; Cillo, U. Subnormothermic machine perfusion protects steatotic livers against preservation injury: A potential for donor pool increase? Liver Transpl. 2009, 15, 20–29. [Google Scholar] [CrossRef]
- Olschewski, P.; Gass, P.; Ariyakhagorn, V.; Jasse, K.; Hunold, G.; Menzel, M.; Schoning, W.; Schmitz, V.; Neuhaus, P.; Puhl, G. The influence of storage temperature during machine perfusion on preservation quality of marginal donor livers. Cryobiology 2010, 60, 337–343. [Google Scholar] [CrossRef]
- Tolboom, H.; Izamis, M.L.; Sharma, N.; Milwid, J.M.; Uygun, B.; Berthiaume, F.; Uygun, K.; Yarmush, M.L. Subnormothermic machine perfusion at both 20 degrees C and 30 degrees C recovers ischemic rat livers for successful transplantation. J. Surg. Res. 2012, 175, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Iwata, H.; Nakajo, T.; Kaneko, H.; Okazawa, Y.; Zin, N.K.M.; Bochimoto, H.; Ohashi, M.; Kawada, Y.; Kamikawa, S.; Kudo, T.; et al. Combined Use of Subnormothermic Extracorporeal Support and Hypothermic Oxygenated Machine Perfusion for Liver Graft after Cardiac Death in Pigs. Transplant. Proc. 2023, 54, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Bochimoto, H.; Matsuno, N.; Ishihara, Y.; Shonaka, T.; Koga, D.; Hira, Y.; Nishikawa, Y.; Furukawa, H.; Watanabe, T. The ultrastructural characteristics of porcine hepatocytes donated after cardiac death and preserved with warm machine perfusion preservation. PLoS ONE 2017, 12, e0186352. [Google Scholar] [CrossRef] [PubMed]
- Bochimoto, H.; Ishihara, Y.; Mohd Zin, N.K.; Iwata, H.; Kondoh, D.; Obara, H.; Matsuno, N. Ultrastructural changes in porcine liver sinusoidal endothelial cells of machine perfused liver donated after cardiac death. World J. Gastroenterol. 2022, 28, 2100–2111. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Nakamura, S.; Koizumi, T.; Sakaguchi, S.; Baba, S.; Muro, H.; Fujise, Y. The beneficial effect of a prostaglandin I2 analog on ischemic rat liver. Transplantation 1991, 52, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Buchwald, J.E.; Martins, P.N. Review of Current Machine Perfusion Therapeutics for Organ Preservation. Transplantation 2020, 104, 1792–1803. [Google Scholar] [CrossRef] [PubMed]
- Ishii, D.; Matsuno, N.; Gochi, M.; Iwata, H.; Shonaka, T.; Nishikawa, Y.; Obara, H.; Yokoo, H.; Furukawa, H. Beneficial effects of end-ischemic oxygenated machine perfusion preservation for split-liver transplantation in recovering graft function and reducing ischemia-reperfusion injury. Sci. Rep. 2021, 11, 22608. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Matsuno, N.; Watanabe, K.; Furukori, M.; Obara, H.; Bochimoto, H.; Watanabe, T.; Fukukawa, H. Scanning Electron Microscopy Findings of Machine Perfused Liver Graft after Warm Ischemia between Hypothermic and Rewarming Machine Perfusion in Pigs. Transplant. Proc. 2016, 48, 2467–2470. [Google Scholar] [CrossRef]
- Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Stepanova, A.; Niatsetskaya, Z.; Sosunov, S.; Arndt, S.; Murphy, M.P.; Galkin, A.; Ten, V.S. Attenuation of oxidative damage by targeting mitochondrial complex I in neonatal hypoxic-ischemic brain injury. Free Radic. Biol. Med. 2018, 124, 517–524. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijevic, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Muller, X.; Mueller, M.; Stepanova, A.; Kron, P.; de Rougemont, O.; Muiesan, P.; Clavien, P.A.; Galkin, A.; Meierhofer, D.; et al. Hypothermic oxygenated perfusion protects from mitochondrial injury before liver transplantation. EBioMedicine 2020, 60, 103014. [Google Scholar] [CrossRef]
- Wang, L.; Thompson, E.; Bates, L.; Pither, T.L.; Hosgood, S.A.; Nicholson, M.L.; Watson, C.J.E.; Wilson, C.; Fisher, A.J.; Ali, S.; et al. Flavin Mononucleotide as a Biomarker of Organ Quality—A Pilot Study. Transplant. Direct 2020, 6, e600. [Google Scholar] [CrossRef] [PubMed]
- Panconesi, R.; Flores Carvalho, M.; Mueller, M.; Meierhofer, D.; Dutkowski, P.; Muiesan, P.; Schlegel, A. Viability Assessment in Liver Transplantation-What Is the Impact of Dynamic Organ Preservation? Biomedicines 2021, 9, 161. [Google Scholar] [CrossRef] [PubMed]
- Maione, F.; Gilbo, N.; Lazzaro, S.; Friend, P.; Camussi, G.; Romagnoli, R.; Pirenne, J.; Jochmans, I.; Monbaliu, D. Porcine Isolated Liver Perfusion for the Study of Ischemia Reperfusion Injury: A Systematic Review. Transplantation 2018, 102, 1039–1049. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medication Name | Brand Name and Manufacturer | Quantity | |
|---|---|---|---|
| Histidine-tryptophan-ketoglutarate solution | Custodiol; Dr. Franz Köhler Chemie GMBH, Bensheim, Germany | 500 | mL |
| 5% albumin | Kenketu Albumin 25% for I.V. Injection 12.5 g/50 mL; Takeda Pharmaceutical, Tokyo, Japan | 250 | mL |
| Vitamin | Vitaject Injection Kit; Terumo, Tokyo, Japan | 10 | mL |
| Amino acid | Hikarilevan; Nihon Pharmaceutical, Tokyo, Japan | 200 | mL |
| Glutathione | Tathion for Injection; Choseido Pharmaceutical, Tokushima, Japan | 1000 | mg |
| Fast-acting insulin human | Novolin R Injection; Novo Nordisk Pharma, Tokyo, Japan | 50 | units |
| Methylprednisolone sodium succinate | Solu-Medrol for Intravenous Use; Pfizer, Tokyo, Japan | 250 | mg |
| 8.4% sodium bicarbonate | Meylon Injection 8.4%; Otsuka Pharmaceutical Factory, Naruto, Japan | 20 | mL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwata, H.; Obara, H.; Nakajo, T.; Kaneko, H.; Okazawa, Y.; Mohd Zin, N.K.; Bochimoto, H.; Ohashi, M.; Kawada, Y.; Ohara, M.; et al. Beneficial Effects of Combined Use of Extracorporeal Membrane Oxygenation and Hypothermic Machine Perfusion in Porcine Donors after Cardiac Death for Liver Transplantation. J. Clin. Med. 2023, 12, 6031. https://doi.org/10.3390/jcm12186031
Iwata H, Obara H, Nakajo T, Kaneko H, Okazawa Y, Mohd Zin NK, Bochimoto H, Ohashi M, Kawada Y, Ohara M, et al. Beneficial Effects of Combined Use of Extracorporeal Membrane Oxygenation and Hypothermic Machine Perfusion in Porcine Donors after Cardiac Death for Liver Transplantation. Journal of Clinical Medicine. 2023; 12(18):6031. https://doi.org/10.3390/jcm12186031
Chicago/Turabian StyleIwata, Hiroyoshi, Hiromichi Obara, Tetsuya Nakajo, Hiroki Kaneko, Yuga Okazawa, Nur Khatijah Mohd Zin, Hiroki Bochimoto, Makito Ohashi, Yoko Kawada, Mizuho Ohara, and et al. 2023. "Beneficial Effects of Combined Use of Extracorporeal Membrane Oxygenation and Hypothermic Machine Perfusion in Porcine Donors after Cardiac Death for Liver Transplantation" Journal of Clinical Medicine 12, no. 18: 6031. https://doi.org/10.3390/jcm12186031