
Effect of Dapagliflozin on Patients with Rheumatic Heart Disease Mitral Stenosis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subject
2.3. Measurement of Biomarker and LA Function
2.4. Statistical Analysis
3. Results
3.1. Effect of Dapagliflozin on Biomarker Fibrosis Levels in RHD Mitral Stenosis
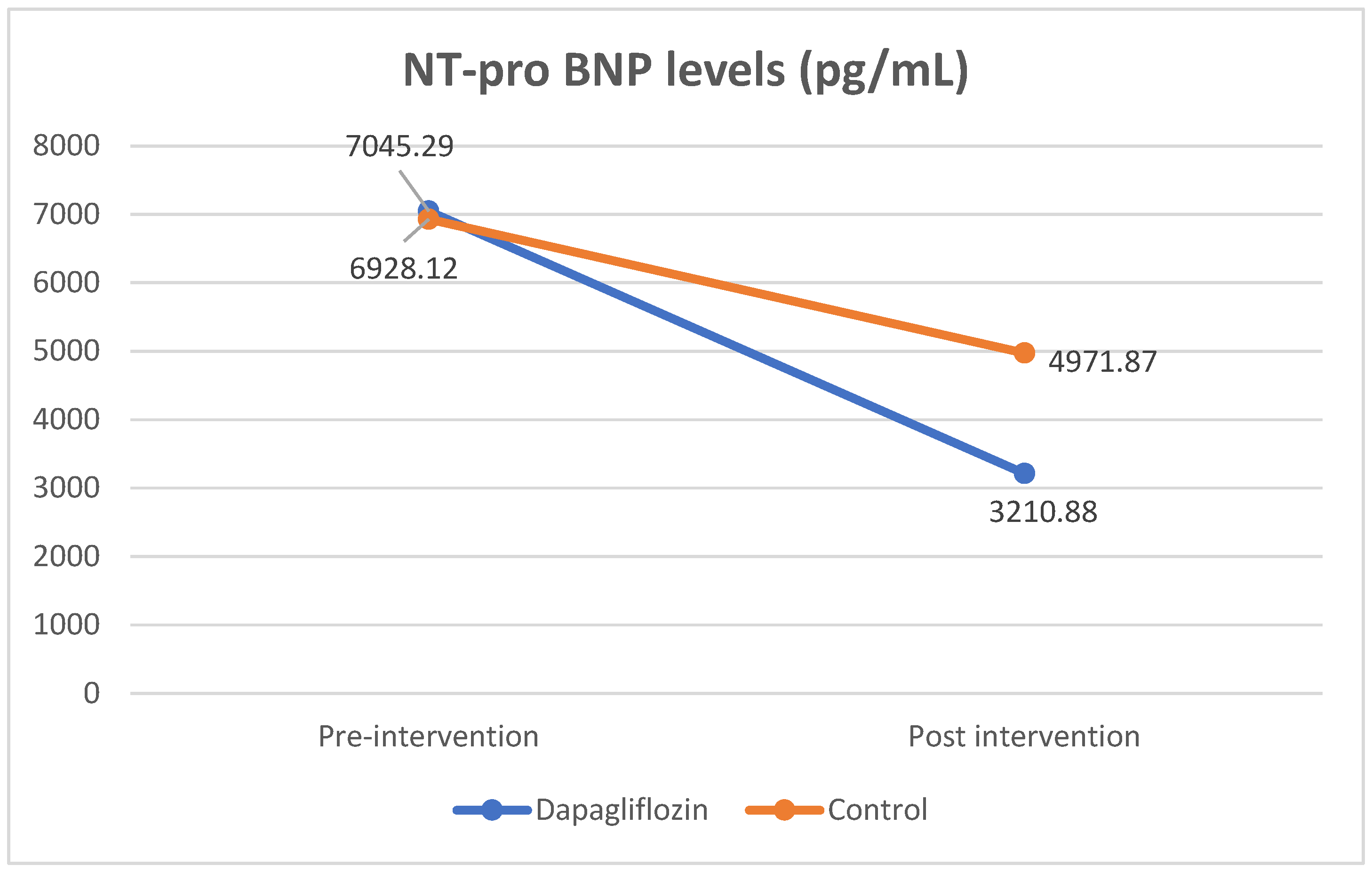
3.2. Effect of Dapagliflozin on NT-pro BNP Levels in RHD Mitral Stenosis
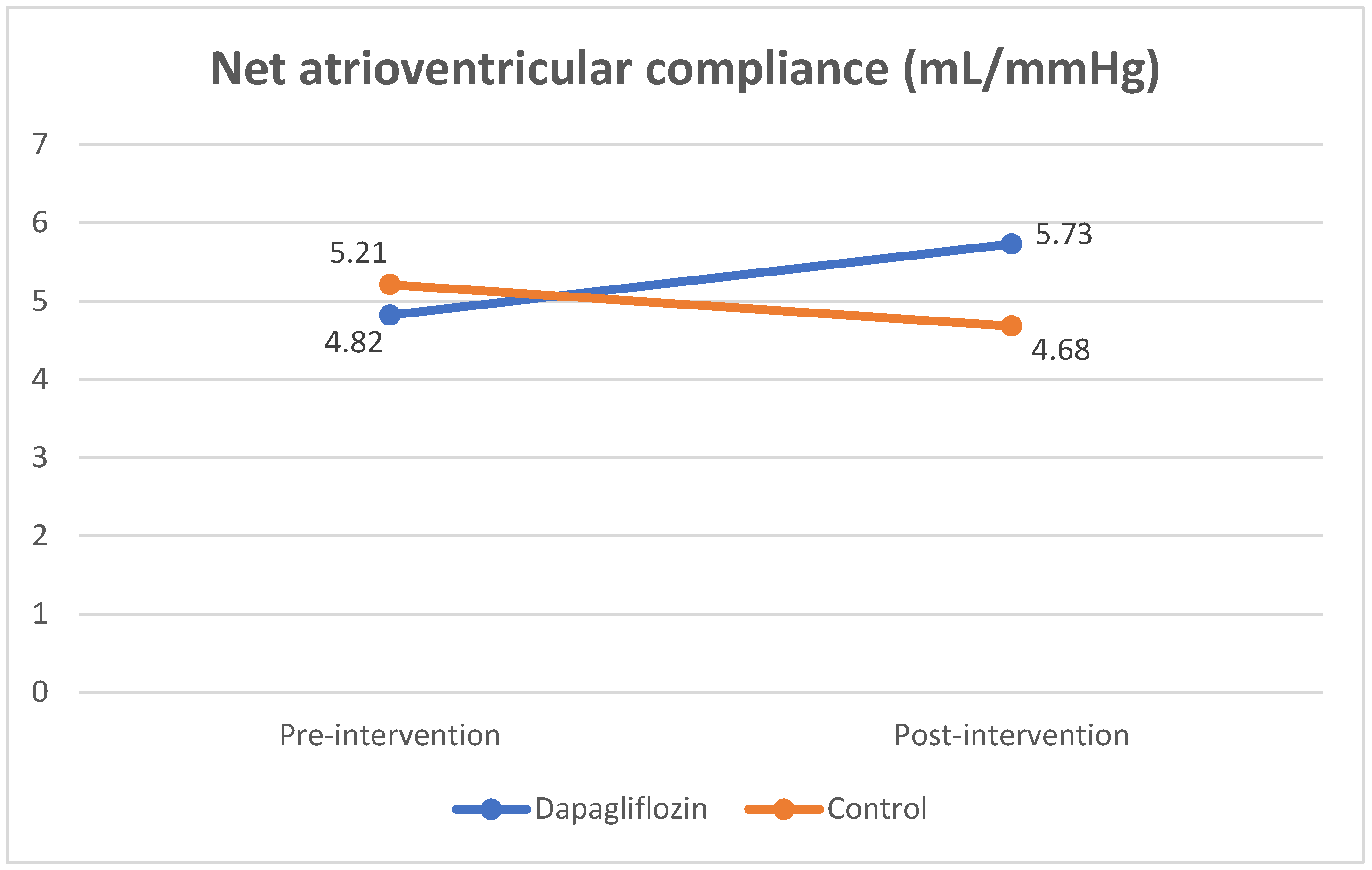
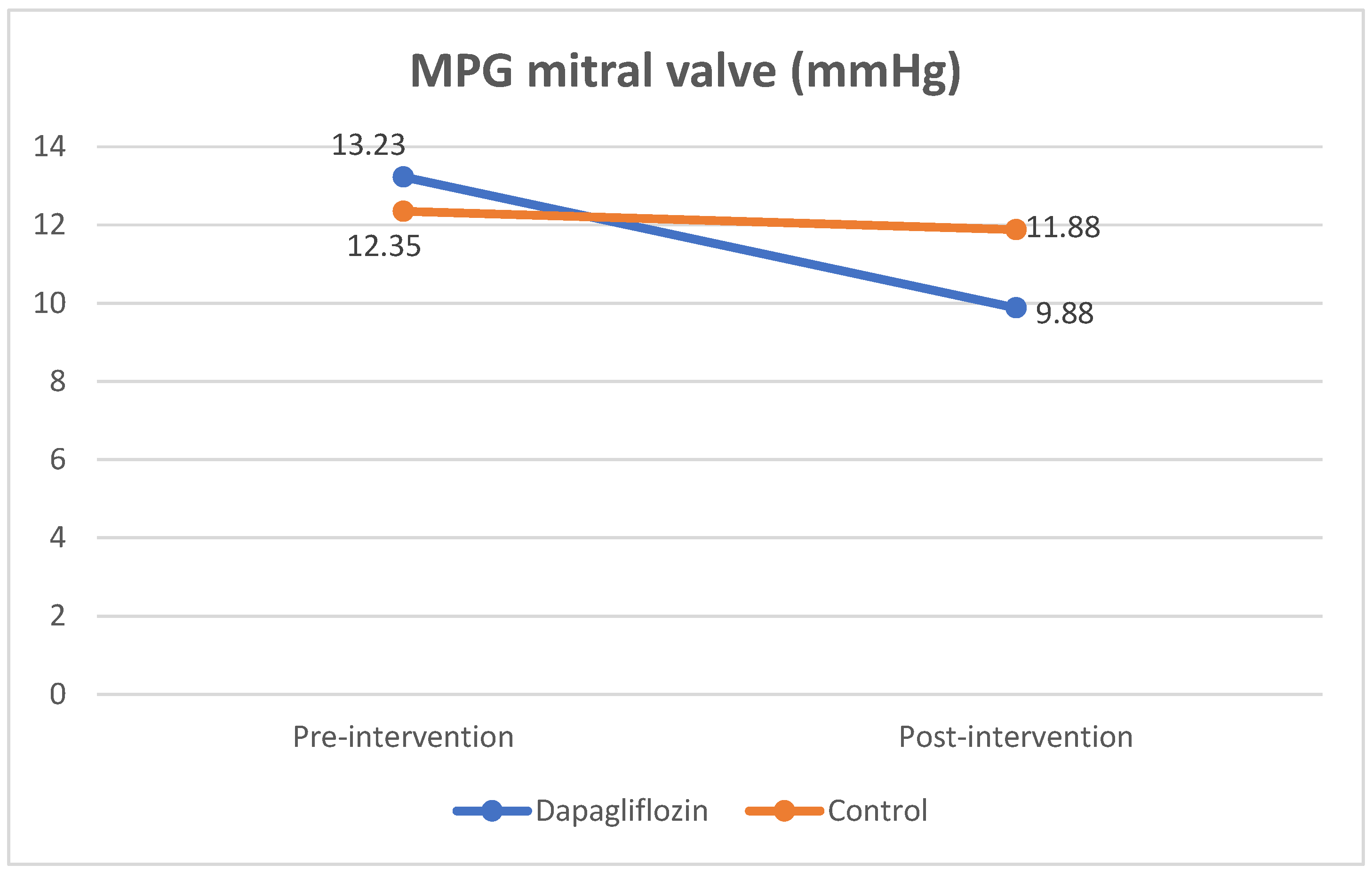
3.3. Effect of Dapagliflozin on Cn and Mitral Valve Mean Pressure Gradient in RHD Mitral Stenosis
3.4. Relationship of Changes in Fibrosis Biomarkers with Cn and NT-pro BNP Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Steer, A.C.; Carapetis, J.R. Acute Rheumatic Fever and Rheumatic Heart Disease in Indigenous Populations. Pediatr. Clin. 2009, 56, 1401–1419. [Google Scholar] [CrossRef] [PubMed]
- Guilherme, L.; Köhler, K.F.; Kalil, J. Rheumatic heart disease: Mediation by complex immune events. Adv. Clin. Chem. 2011, 53, 31–50. [Google Scholar] [PubMed]
- Kim, L.; Do, K.K.; Woo, I.Y.; Dong, H.S.; Ick, M.J.; Han, K.P.; Chang, B.C. Overexpression of transforming growth factor-β1 in the valvular fibrosis of chronic rheumatic heart disease. J. Korean Med. Sci. 2008, 23, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Toor, D.; Sharma, N. T cell subsets: An integral component in pathogenesis of rheumatic heart disease. Immunol. Res. 2018, 66, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, T.; Mukherjee, S.; Ghosh, S.; Biswas, M.; Dutta, S.; Pattari, S.; Chatterjee, S.; Bandyopadhyay, A. Clinical significance of markers of collagen metabolism in rheumatic mitral valve disease. PLoS ONE 2014, 9, e90527. [Google Scholar] [CrossRef]
- Banerjee, T.; Mukherjee, S.; Biswas, M.; Dutta, S.; Chatterjee, S.; Ghosh, S.; Pattari, S.; Nanda, N.C.; Bandyopadhyay, A. Circulating carboxy-terminal propeptide of type i procollagen is increased in rheumatic heart disease. Int. J. Cardiol. 2012, 156, 117–119. [Google Scholar] [CrossRef]
- Wynn, T. Cellular and molecular mechanisms in fibrosis. J. Pathol. 2008, 214, 199–210. [Google Scholar] [CrossRef]
- Kumar, R.K.; Antunes, M.J.; Beaton, A.; Mirabel, M.; Nkomo, V.T.; Okello, E.; Regmi, P.R.; Reményi, B.; Sliwa-Hähnle, K.; Zühlke, L.J.; et al. Contemporary Diagnosis and Management of Rheumatic Heart Disease: Implications for Closing the Gap: A Scientific Statement From the American Heart Association. Circulation 2020, 142, e337–e357. [Google Scholar] [CrossRef]
- Rudiktyo, E.; Wind, A.; Doevendans, P.; Siswanto, B.B.; Cramer, M.J.; Soesanto, A.M. Characteristics of patients with rheumatic heart disease in a national referral hospital in Indonesia. Med. J. Indones. 2022, 31, 178–185. [Google Scholar] [CrossRef]
- Ismail, A.S.; Baghdady, Y.; Salem, M.A.; Wahab, A.A. The use of MRI in quantification of the atrial fibrosis in patients with rheumatic mitral disease. Egypt J. Radiol. Nucl. Med. 2020, 51, 199. [Google Scholar] [CrossRef]
- Yetim, M.; Karaagac, K.; Şaşmaz, A.; Yılmaz, M. The Relationship Between Left Atrial Mechanical Function and Functional Capacity in Mitral Stenosis. J. Clin. Anal. Med. 2013, 4, 458–461. [Google Scholar]
- Hrabia, J.B.; Pogue, E.P.L.; Zayachkowski, A.G.; Długosz, D.; Kruszelnicka, O.; Surdacki, A.; Chyrchel, B. Left atrial compliance: An overlooked predictor of clinical outcome in patients with mitral stenosis or atrial fibrillation undergoing invasive management. Postep. W Kardiol. Interwencyjnej 2018, 14, 120–127. [Google Scholar] [CrossRef]
- Iltumur, K.; Karabulut, A.; Yokus, B.; Yavuzkir, M.; Taskesen, T.; Toprak, N. N-terminal proBNP plasma levels correlate with severity of mitral stenosis. J. Heart Valve Dis. 2005, 14, 735–741. [Google Scholar] [PubMed]
- Arat-Özkan, A.; Kaya, A.; Yiǧit, Z.; Balcı, H.; Ökçün, B.; Yazıcıoǧlu, N.; Küçükoǧlu, S. Serum N-Terminal pro-BNP Levels Correlate with Symptoms and Echocardiographic Findings in Patients with Mitral Stenosis. Echocardiography 2005, 22, 473–478. [Google Scholar] [CrossRef]
- Jhund, P.S.; Kondo, T.; Butt, J.H.; Docherty, K.F.; Claggett, B.L.; Desai, A.S.; Vaduganathan, M.; Gasparyan, S.B.; Bengtsson, O.; Lindholm, D.; et al. Dapagliflozin across the range of ejection fraction in patients with heart failure: A patient-level, pooled meta-analysis of DAPA-HF and DELIVER. Nat. Med. 2022, 28, 1956–1964. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef]
- Li, G.; Zhao, C.; Fang, S. SGLT2 promotes cardiac fibrosis following myocardial infarction and is regulated by miR-141. Exp. Ther. Med. 2021, 22, 715. [Google Scholar] [CrossRef]
- Tian, J.; Zhang, M.; Suo, M.; Liu, D.; Wang, X.; Liu, M.; Pan, J.; Jin, T.; An, F. Dapagliflozin alleviates cardiac fibrosis through suppressing EndMT and fibroblast activation via AMPKα/TGF-β/Smad signalling in type 2 diabetic rats. J. Cell Mol. Med. 2021, 25, 7642–7659. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, X.; Chu, Y.; Chen, X.; Du, H.; Zhang, H.; Chai, D. Dapagliflozin: A sodium–glucose cotransporter 2 inhibitor, attenuates angiotensin II-induced cardiac fibrotic remodeling by regulating TGFβ1/Smad signaling. Cardiovasc. Diabetol. 2021, 20, 121. [Google Scholar] [CrossRef]
- Lin, Y.W.; Chen, C.Y.; Shih, J.Y.; Cheng, B.C.; Chang, C.P.; Lin, M.T.; Ho, C.; Chen, Z.; Fisch, S.; Chang, W. Dapagliflozin improves cardiac hemodynamics and mitigates arrhythmogenesis in mitral regurgitation-induced myocardial dysfunction. J. Am. Heart Assoc. 2021, 10, e019274. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Soga, F.; Tatsumi, K.; Mochizuki, Y.; Sano, H.; Toki, H.; Matsumoto, K.; Shite, J.; Takaoka, H.; Doi, T.; et al. Positive effect of dapagliflozin on left ventricular longitudinal function for type 2 diabetic mellitus patients with chronic heart failure. Cardiovasc. Diabetol. 2020, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Oldgren, J.; Laurila, S.; Åkerblom, A.; Latva-Rasku, A.; Rebelos, E.; Isackson, H.; Saarenhovi, M.; Eriksson, O.; Heurling, K.; Johansson, E.; et al. Effects of 6 weeks of treatment with dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on myocardial function and metabolism in patients with type 2 diabetes: A randomized, placebo-controlled, exploratory study. Diabetes Obes. Metab. 2021, 23, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.H.; Docherty, K.F.; Jhund, P.S.; de Boer, R.A.; Böhm, M.; Desai, A.S.; Køber, L. Dapagliflozin and atrial fibrillation in heart failure with reduced ejection fraction: Insights from DAPA-HF. Eur. J. Heart Fail. 2022, 24, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Okunrintemi, V.; Mishriky, B.M.; Powell, J.R.; Cummings, D.M. Sodium-glucose co-transporter-2 inhibitors and atrial fibrillation in the cardiovascular and renal outcome trials. Diabetes Obes. Metab. 2021, 23, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Antonini-Canterin, F.; Moura, L.M.; Enache, R.; Leiballi, E.; Pavan, D.; Piazza, R.; Popescu, B.A.; Ginghina, C.; Nicolosi, G.L.; Rajamannan, N.M.; et al. Effect of hydroxymethylglutaryl coenzyme-a reductase inhibitors on the long-term progression of rheumatic mitral valve disease. Circulation 2010, 121, 2130–2136. [Google Scholar] [CrossRef]
- Herry, Y. P325Statin inhibits synthesis of type I collagen in patients with rheumatic heart disease. Cardiovasc. Res. 2018, 114 (Suppl. 1), S83. [Google Scholar] [CrossRef]
- Ambari, A.M.; Setianto, B.; Santoso, A.; Radi, B.; Dwiputra, B.; Susilowati, E.; Tulrahmi, F.; Wind, A.; Cramer, M.J.M.; Doevendans, P. Randomised controlled trial into the role of ramipril in fibrosis reduction in rheumatic heart disease: The RamiRHeD trial protocol. BMJ Open 2021, 11, e048016. [Google Scholar] [CrossRef]
- Ganesan, G. How to Assess Mitral Stenosis by Echo—A Step-by-Step Approach. J. Indian Acad. Echocardiogr. Cardiovasc. Imaging 2017, 1, 197–205. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Wojakowski, W. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Pandian, N.G.; Kim, J.K.; Arias-Godinez, J.A.; Marx, G.R.; Michelena, H.I.; Chander Mohan, J.; Ogunyankin, K.O.; Ronderos, R.E.; Sade, L.E.; Sadeghpour, A.; et al. Recommendations for the Use of Echocardiography in the Evaluation of Rheumatic Heart Disease: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2023, 36, 3–28. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Hung, J.; Barbosa, M.M.; Esteves, W.A.; Carvalho, V.T.; Lodi-Junqueira, L.; Neto, C.P.F.; Tan, T.C.; Levine, R.A. Impact of net atrioventricular compliance on clinical outcome in mitral stenosis. Circ. Cardiovasc. Imaging 2013, 6, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Cho, I.J.; Chang, H.J.; Lee, S.Y.; Shim, C.Y.; Hong, G.R.; Chung, N. Differential Impact of Net Atrioventricular Compliance on Clinical Outcomes in Patients with Mitral Stenosis According to Cardiac Rhythm. J. Am. Soc. Echocardiogr. 2017, 30, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Schwammenthal, E.; Vered, Z.; Agranat, O.; Kaplinsky, E.; Rabinowitz, B.; Feinberg, M.S. Impact of Atrioventricular Compliance on Pulmonary Artery Pressure in Mitral Stenosis. An Exercise Echocardiographic Study. Circulation 2000, 102, 2378–2384. [Google Scholar] [CrossRef]
- Ye, Y.; Bajaj, M.; Yang, H.C.; Perez-Polo, J.R.; Birnbaum, Y. SGLT-2 Inhibition with Dapagliflozin Reduces the Activation of the Nlrp3/ASC Inflammasome and Attenuates the Development of Diabetic Cardiomyopathy in Mice with Type 2 Diabetes. Further Augmentation of the Effects with Saxagliptin, a DPP4 Inhibitor. Cardiovasc. Drugs Ther. 2017, 31, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yang, Q.; Bai, W.; Yao, W.; Liu, L.; Xing, Y.; Qi, X. Dapagliflozin Attenuates Myocardial Fibrosis by Inhibiting the TGF-β1/Smad Signaling Pathway in a Normoglycemic Rabbit Model of Chronic Heart Failure. Front. Pharmacol. 2022, 13, 873108. [Google Scholar] [CrossRef]
- Xian, S.; Zeng, Z. Signalling pathways implicated in the pathogenesis of rheumatic heart disease (Review). Exp. Ther. Med. 2020, 21, 76. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.D.; Jhund, P.S.; Docherty, K.F.; Murphy, S.A.; Verma, S.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; et al. Time to Clinical Benefit of Dapagliflozin and Significance of Prior Heart Failure Hospitalization in Patients With Heart Failure With Reduced Ejection Fraction. JAMA Cardiol. 2021, 6, 499–507. [Google Scholar] [CrossRef]
- Guilherme, L. Rheumatic Heart Disease: Key Points on Valve Lesions Development. J. Clin. Exp. Cardiolog. 2012, 1, 13–21. [Google Scholar] [CrossRef]
- Guilherme, L.; Kalil, J. Rheumatic Heart Disease: Molecules Involved in Valve Tissue Inflammation Leading to the Autoimmune Process and Anti-S. pyogenes Vaccine. Front. Immunol. 2013, 4, 352. [Google Scholar] [CrossRef]
- Wright, E.M.; Loo, D.D.F.; Hirayama, B.A. Biology of Human Sodium Glucose Transporters. Physiol. Rev. 2011, 91, 733–794. [Google Scholar] [CrossRef] [PubMed]
- Uthman, L.; Baartscheer, A.; Schumacher, C.A.; Fiolet, J.W.T.; Kuschma, M.C.; Hollmann, M.W.; Coronel, R.; Weber, N.C.; Zuurbier, C.J. Direct Cardiac Actions of Sodium Glucose Cotransporter 2 Inhibitors Target Pathogenic Mechanisms Underlying Heart Failure in Diabetic Patients. Front. Physiol. 2018, 9, 1575. [Google Scholar] [CrossRef] [PubMed]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.S.; Shen, W.; Boulton, D.W.; Leslie, B.R.; Griffen, S.C. Interaction between the sodium-glucose-linked transporter 2 inhibitor dapagliflozin and the loop diuretic bumetanide in normal human subjects. J. Am. Heart Assoc. 2018, 7, e007046. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Kelly, R.V.; Huggins, C.; Stouffer, G.A. Mitral stenosis. In Cardiovascular Hemodynamics for the Clinician; Wiley: Hoboken, NJ, USA, 2017; pp. 129–142. [Google Scholar] [CrossRef]
- Kreimer, F.; Gotzmann, M. Left Atrial Cardiomyopathy—A Challenging Diagnosis. Front. Cardiovasc. Med. 2022, 9, 942385. [Google Scholar] [CrossRef]
- Ko, Y.-G.; Ha, J.-W.; Chung, N.; Shim, W.-H.; Kang, S.-M.; Rim, S.-J.; Jang, Y.; Cho, S.-Y.; Kim, S.-S. Effects of left atrial compliance on left atrial pressure in pure mitral stenosis. Catheter. Cardiovasc. Interv. 2001, 52, 328–333. [Google Scholar] [CrossRef]
- Barry, A. Borlaug. CAMEO-DAPA: Evaluation Of The Mechanism Of Benefit For Dapagliflozin In HFpEF: An Invasive Hemodynamic Randomized Trial. In ACC Scientific Sessions; American College of Cardiology: Washington, DC, USA, 2023. [Google Scholar]
- Shim, C.Y.; Seo, J.; Cho, I.; Lee, C.J.; Cho, I.J.; Lhagvasuren, P.; Hong, G.R. Randomized, Controlled Trial to Evaluate the Effect of Dapagliflozin on Left Ventricular Diastolic Function in Patients With Type 2 Diabetes Mellitus: The IDDIA Trial. Circulation 2021, 143, 510–512. [Google Scholar] [CrossRef]
- Cappetta, D.; De Angelis, A.; Ciuffreda, L.P.; Coppini, R.; Cozzolino, A.; Miccichè, A.; Berrino, L. Amelioration of diastolic dysfunction by dapagliflozin in a non-diabetic model involves coronary endothelium. Pharmacol. Res. 2020, 157, 104781. [Google Scholar] [CrossRef]
- Samiei, N.; Zolfaghari, R.; Sanati, H.; Tabrizi, R.R.; Zahedmehr, A.; Firouzi, A. NT-probnp in mitral stenosis: Can it be a predictor of hemodynamic status? Iran. Heart J. 2020, 21, 98–104. [Google Scholar]
- Safi, M.; Bayat, F.; Ahmadi, Z.; Shekarchizadeh, M.; Khaheshi, I.; Naderian, M. The change in NT-pro-BNP and post-PTMC echocardiography parameters in patients with mitral stenosis. A pilot study. Rom. J. Intern. Med. 2017, 55, 75–81. [Google Scholar] [CrossRef]
- Khare, R.; Dwivedi, S. NT-ProBNP as a Potential Marker of Left Atrial Dysfunction in Rheumatic Mitral Stenosis: Correlation with Left Atrial Function after PBMV. J. Heart Valve Dis. 2016, 25, 613–618. [Google Scholar] [PubMed]
- Inoue, S.; Murakami, Y.; Sano, K.; Katoh, H.; Shimada, T. Atrium as a source of brain natriuretic polypeptide in patients with atrial fibrillation. J. Card. Fail. 2000, 6, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Stewart, R.A.H.; Zeng, I.; Raffel, C.; Kerr, A.J. Comparison of Atrial and Brain Natriuretic Peptide for the Assessment of Mitral Stenosis. Heart Lung Circ. 2011, 20, 517–524. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | Dapagliflozin Group (n = 17) | Control Group (n = 16) | p-Value |
|---|---|---|---|
| Demography and comorbidities | |||
| Age, years | 51.35 ± 9.88 | 55.94 ± 6.65 | 0.13 |
| Sex | |||
| Female, n (%) | 14 (82.53%) | 15 (93.75%) | 0.601 |
| Male, n (%) | 3 (17.64%) | 1 (6.25%) | |
| Body mass index (BMI), kg/m2 | 22.87 ± 3.14 | 21.08 ± 3.10 | 0.11 |
| Atrial fibrillation (%) | 17 (100%) | 16 (100%) | - |
| Hypertension, n (%) | 1 (5.88%) | 3 (1.87%) | 0.335 |
| Type 2 diabetes, n (%) | 2 (11.76%) | 0 (0%) | 0.485 |
| Coronary artery disease, n (%) | 0 (0%) | 0 (0%) | - |
| Smoker, n (%) | 1 (5.88%) | 1 (6.25%) | 0.965 |
| Examination | |||
| Systolic blood pressure, mmHg | 118.53 ± 13.25 | 116.63 ± 17.25 | 0.417 |
| Diastolic blood pressure, mmHg | 76.71 ± 10.83 | 78.00 ± 13.79 | 0.766 |
| Heart rate, bpm | 72.11 ± 14.13 | 78.93 ± 15.50 | 0.196 |
| Creatinine, mg/dL | 1.03 ± 0.48 | 0.93 ± 0.34 | 0.773 |
| eGFR, mL/ mL/min/1.73 m2 | 67.94 ± 26.37 | 65.37 ± 22.22 | 0.765 |
| Blood glucose, mg/dL | 128.94 ± 43.78 | 116.75 ± 22.22 | 0.787 |
| Echocardiography parameters | |||
| MVA planimetry, cm2 | 0.75 ± 0.13 | 0.77 ± 0.13 | 0.616 |
| LA diameter, mm | 56.14 ± 9.26 | 53.52 ± 8.36 | 0.402 |
| RV diameter, mm | 36.29 ± 4.51 | 33.46 ± 7.09 | 0.177 |
| LVIDd, mm | 47.34 ± 7.21 | 45.99 ± 5.81 | 0.665 |
| LAVI, mL/m2 | 145.89 ± 75.29 | 139.26 ± 69.27 | 0.707 |
| Cn, mLmmHg | 4.82 ± 1.71 | 5.21 ± 1.99 | 0.546 |
| Mean pressure gradient mitral, mmHg | 13.23 ± 4.50 | 12.35 ± 4.48 | 0.579 |
| Systolic pulmonary artery pressure, mmHg | 64.83 ± 14.74 | 65.65 ± 22.79 | 0.902 |
| LVEF, % | 53.73 ± 10.36 | 57.20 ± 9.02 | 0.314 |
| TAPSE, mm | 18.30 ± 4.12 | 18.42 ± 7.53 | 0.954 |
| Pulmonary hypertension probability (intermediate to high), % | 15 (88.23%) | 12 (75%) | 0.398 |
| Pharmacological treatment | |||
| ACE-I/ ARB | 0 (0%) | 0 (0%) | - |
| Beta blockers | 12 (70.58%) | 8 (50%) | 0.394 |
| Furosemide | 13 (76.47%) | 12 (75%) | 1 |
| Spironolactone | 17 (100%) | 16 (100%) | - |
| Antiplatelet | 0 (0%) | 0 (0%) | - |
| Warfarin | 17 (100%) | 16 (100%) | - |
| Digoxin | 5 (29.41%) | 8 (50%) | 0.394 |
| Complication | |||
| Hypoglycemia | 1 (5.88%) | 0 (0%) | 0.303 |
| Diabetic ketoacidosis | 0 (0%) | 0 (0%) | - |
| Hypotension | 1 (5.88%) | 0 (0%) | 0.303 |
| Amputation | 0 (0%) | 0 (0%) | - |
| Genital infection | 0 (0%) | 0 (0%) | - |
| PICP (ng/mL) | MMP-1/TIMP-1 Ratio | TGF-β1 (pg/mL) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Dapagliflozin Group | Control Group | p-Value | Dapagliflozin Group | Control Group | p-Value | Dapagliflozin Group | Control Group | p-Value | |
| Pre-intervention | 67.23 ± 44.61 | 56.04 ± 22.66 | 0.614 | 0.63 ± 0.31 | 0.73 ± 0.75 | 0.540 | 1.66 ± 0.64 | 1.39 ± 0.49 | 0.195 |
| Post-intervention | 158.54 ± 71.18 | 161.45 ± 107.63 | 0.719 | 0.32 ± 0.23 | 0.23 ± 0.16 | 0.171 | 3.38 ± 2.26 | 2.25 ± 1.77 | 0.058 |
| p-value (post-pre) | 0.000 | 0.000 | 0.005 | 0.002 | 0.005 | 0.044 | |||
| Delta (Δ) | 91.30 ± 59.83 | 105.41 ± 94.88 | 0.943 | 0.31 ± 0.35 | 0.50 ± 0.68 | 0.885 | 1.73 ± 2.34 | 0.86 ± 1.77 | 0.207 |
| Mitral-Valve Mean Pressure Gradient (pg/mL) | p-Value | ||
|---|---|---|---|
| Dapagliflozin Group | Control Group | ||
| Pre-intervention | 7045.29 ± 3182.26 | 6928.12 ± 3690.44 | 0.857 |
| Post-intervention | 3210.88 ± 1019.46 | 4971.87 ± 3634.65 | 0.449 |
| p-value (post-pre) | 0.000 | 0.002 | |
| Delta (Δ) | 3832.42 ± 2857.52 | 1956.25 ± 1755.42 | 0.034 |
| Echocardiography Parameters | Dapagliflozin Group (n = 17) | Control Group (n = 16) | p-Value (between Pre-Intervention Group) | p-Value (between Post-Intervention Group) | ||||
|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | p | Pre-Intervention | Post-Intervention | p | |||
| MVA planimetry, cm2 | 0.75 ± 0.13 | 0.73 ± 0.03 | 0.403 | 0.77 ± 0.13 | 0.72 ± 0.03 | 0.099 | 0.616 | 0.905 |
| LA diameter, mm | 56.14 ± 9.26 | 56.06 ± 1.84 | 0.529 | 53.52 ± 8.36 | 53.72 ± 2.11 | 0.702 | 0.402 | 0.952 |
| RV diameter, mm | 36.29 ± 4.51 | 34.58 ± 4.95 | 0.057 | 33.46 ± 7.09 | 34.09 ± 1.14 | 0.679 | 0.177 | 0.822 |
| LVIDd, mm | 47.34 ± 7.21 | 49.34 ± 6.21 | 0.091 | 45.99 ± 5.81 | 45.14 ± 5.91 | 0.275 | 0.665 | 0.113 |
| LAVI, mL/m2 | 145.89 ± 75.29 | 139.26 ± 69.27 | 0.055 | 139.26 ± 69.27 | 149.63 ± 105.89 | 0.326 | 0.707 | 0.744 |
| Cn, mL/mmHg | 4.82 ± 1.71 | 5.73 ± 2.19 | 0.017 | 5.21 ± 1.99 | 4.68 ± 1.73 | 0.379 | 0.546 | 0.121 |
| Mean pressure gradient mitral, mmHg | 13.23 ± 4.50 | 9.88 ± 3.87 | 0.001 | 12.35 ± 4.48 | 11.88 ± 4.01 | 0.756 | 0.579 | 0.155 |
| Systolic pulmonary artery pressure, mmHg | 64.83 ± 14.74 | 67.89 ± 9.78 | 0.446 | 65.65 ± 22.79 | 73.49 ± 22.32 | 0.335 | 0.902 | 0.353 |
| LVEF, % | 53.73 ± 10.36 | 50.31 ± 8.75 | 0.215 | 57.20 ± 9.02 | 56.02 ± 6.96 | 0.682 | 0.314 | 0.046 |
| TAPSE, mm | 18.30 ± 4.12 | 17.51 ± 3.76 | 0.568 | 18.42 ± 7.53 | 18.00 ± 4.22 | 0.480 | 0.954 | 0.423 |
| Pulmonary hypertension probability (intermediate to high), % | 15 (88.23%) | 14 (82.35%) | 1.00 | 12 (75.00%) | 11 (64.71%) | 1.00 | 0.398 | 0.362 |
| Cn (mL/mmHg) | p-Value | ||
|---|---|---|---|
| Dapagliflozin Group | Control Group | ||
| Pre-intervention | 4.82 ± 1.71 | 5.21 ± 1.99 | 0.546 |
| Post-intervention | 5.73 ± 2.19 | 4.68 ± 1.73 | 0.121 |
| p-value (post-pre) | 0.017 | 0.379 | |
| Delta (Δ) | 0.90 ± 1.29 | −0.53 ± 2.57 | 0.049 |
| Mitral Valve Mean Pressure Gradient (mmHg) | p-Value | ||
|---|---|---|---|
| Dapagliflozin Group | Control Group | ||
| Pre-intervention | 13.23 ± 4.50 | 12.35 ± 4.48 | 0.579 |
| Post-intervention | 9.88 ± 3.87 | 11.88 ± 4.01 | 0.155 |
| p-value (post-pre) | 0.001 | 0.756 | |
| Delta (Δ) | 3.34 ± 3.11 | 0.46 ± 4.15 | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asrial, A.A.; Reviono, R.; Soetrisno, S.; Setianto, B.Y.; Widyaningsih, V.; Nurwati, I.; Wasita, B.; Pudjiastuti, A. Effect of Dapagliflozin on Patients with Rheumatic Heart Disease Mitral Stenosis. J. Clin. Med. 2023, 12, 5898. https://doi.org/10.3390/jcm12185898
Asrial AA, Reviono R, Soetrisno S, Setianto BY, Widyaningsih V, Nurwati I, Wasita B, Pudjiastuti A. Effect of Dapagliflozin on Patients with Rheumatic Heart Disease Mitral Stenosis. Journal of Clinical Medicine. 2023; 12(18):5898. https://doi.org/10.3390/jcm12185898
Chicago/Turabian StyleAsrial, An Aldia, Reviono Reviono, Soetrisno Soetrisno, Budi Yuli Setianto, Vitri Widyaningsih, Ida Nurwati, Brian Wasita, and Anggit Pudjiastuti. 2023. "Effect of Dapagliflozin on Patients with Rheumatic Heart Disease Mitral Stenosis" Journal of Clinical Medicine 12, no. 18: 5898. https://doi.org/10.3390/jcm12185898