


Changes in Parameters after High Tibial Osteotomy: Comparison of EOS System and Computed Tomographic Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
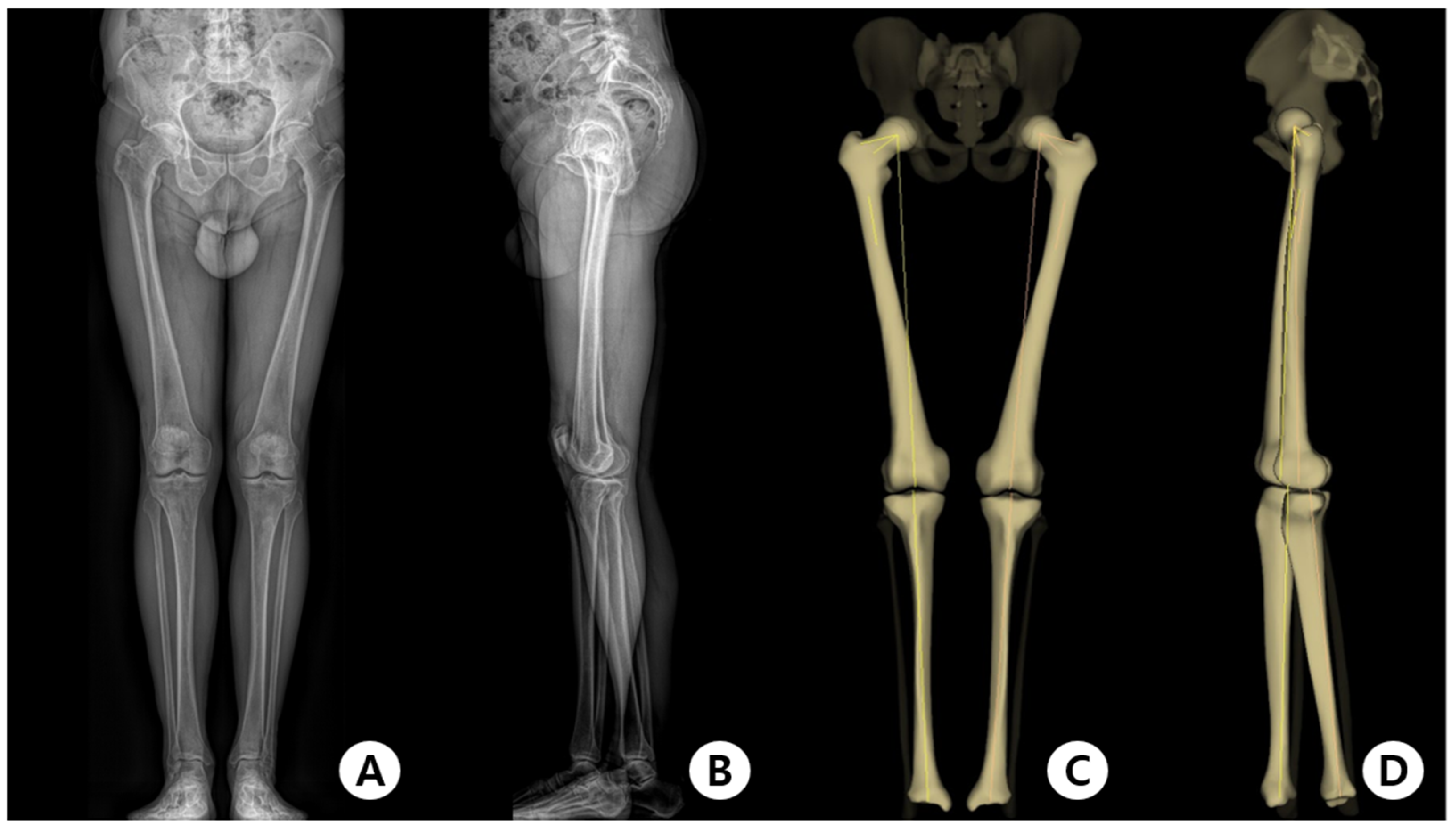
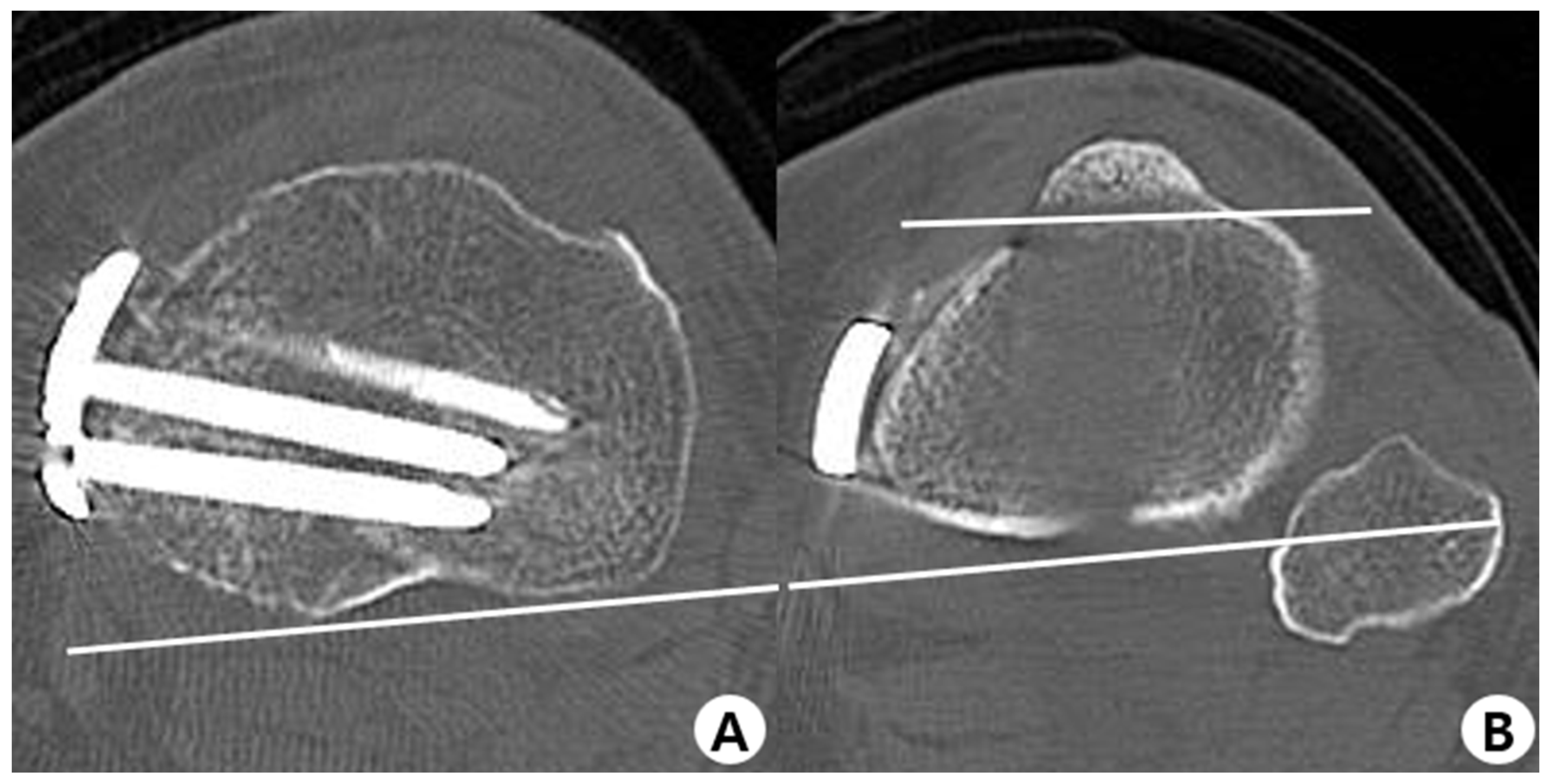
2.2. Evaluation Methods
2.3. Measurement of Parameters and Clinical Outcomes
2.4. Surgical Technique
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, D.C.; Byun, S.J. High tibial osteotomy. Knee Surg. Rel. Res. 2012, 24, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Amendola, A.; Fowler, P.J.; Litchfield, R.; Kirkley, S.; Clatworthy, M. Opening wedge high tibial osteotomy using a novel technique–early results and complications. J. Knee Surg. 2004, 17, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Jakob, R.; Murphy, S. Tibial osteotomy for varus gonarthrosis: Indication, planning, and operative technique. Instr. Course Lect. 1992, 41, 87–93. [Google Scholar] [PubMed]
- Koshino, T.; Murase, T.; Saito, T. Medial opening-wedge high tibial osteotomy with use of porous hydroxyapatite to treat medial compartment osteoarthritis of the knee. J. Bone Joint Surg. Am. 2003, 85, 78–85. [Google Scholar] [CrossRef]
- Gomoll, A.H. High tibial osteotomy for the treatment of unicompartmental knee osteoarthritis: A review of the literature, indications, and technique. Phys. Sportsmed. 2011, 39, 45–54. [Google Scholar] [CrossRef]
- Bauer, G.C.; Insall, J.; Koshino, T. Tibial osteotomy in gonarthrosis (osteo-arthritis of the knee). J. Bone Joint Surg. Am. 1969, 51, 1545–1563. [Google Scholar] [CrossRef]
- Insall, J.N.; Joseph, D.M.; Msika, C. High tibial osteotomy for varus gonarthrosis. A long-term follow-up study. J. Bone Joint Surg. Am. 1984, 66, 1040–1048. [Google Scholar] [CrossRef]
- Yasuda, K.; Majima, T.; Tsuchida, T.; Kaneda, K. A ten- to 15-year follow-up observation of high tibial osteotomy in medial compartment osteoarthrosis. Clin. Orthop. Relat. Res. 1992, 282, 186–195. [Google Scholar] [CrossRef]
- Kendoff, D.; Lo, D.; Goleski, P.; Warkentine, B.; O’Loughlin, P.F.; Pearle, A.D. Open wedge tibial osteotomies influence on axial rotation and tibial slope. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 904–910. [Google Scholar] [CrossRef]
- Hinterwimmer, S.; Feucht, M.J.; Paul, J.; Kirchhoff, C.; Sauerschnig, M.; Imhoff, A.B.; Beitzel, K. Analysis of the effects of high tibial osteotomy on tibial rotation. Int. Orthop. 2016, 40, 1849–1854. [Google Scholar] [CrossRef]
- Kawai, R.; Tsukahara, T.; Kawashima, I.; Yamada, H. Tibial rotational alignment after opening-wedge and closing-wedge high tibial osteotomy. Nagoya J. Med. Sci. 2019, 81, 621–628. [Google Scholar] [PubMed]
- Kuwashima, U.; Takeuchi, R.; Ishikawa, H.; Shioda, M.; Nakashima, Y.; Schroter, S. Comparison of torsional changes in the tibia following a lateral closed or medial open wedge high tibial osteotomy. Knee 2019, 26, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Nha, K.W.; Kim, H.J.; Ahn, H.S.; Lee, D.H. Change in posterior tibial slope after open-wedge and closed-wedge high tibial osteotomy: A meta-analysis. Am. J. Sports Med. 2016, 44, 3006–3013. [Google Scholar] [CrossRef] [PubMed]
- Jang, K.M.; Lee, J.H.; Park, H.J.; Kim, J.L.; Han, S.B. Unintended rotational changes of the distal tibia after biplane medial open-wedge high tibial osteotomy. J. Arthroplast. 2016, 31, 59–63. [Google Scholar] [CrossRef] [PubMed]
- McLaren, C.; Wootton, J.R.; Heath, P.D.; Jones, C.H. Pes planus after tibial osteotomy. Foot Ankle 1989, 9, 300–303. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, O.S.; Teo, S.H.; Lee, Y.S. Change in gait after high tibial osteotomy: A systematic review and meta-analysis. Gait Posture 2017, 57, 57–68. [Google Scholar] [CrossRef]
- Gaasbeek, R.; Welsing, R.; Barink, M.; Verdonschot, N.; van Kampen, A. The influence of open and closed high tibial osteotomy on dynamic patellar tracking: A biomechanical study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 978–984. [Google Scholar] [CrossRef]
- Baumgarten, K.M.; Meyers, K.N.; Fealy, S.; Wright, T.M.; Wickiewicz, T.L. The coronal plane high tibial osteotomy. Part II: A comparison of axial rotation with the opening wedge high tibial osteotomy. HSS J. 2007, 3, 155–158. [Google Scholar] [CrossRef]
- Ducat, A.; Sariali, E.; Lebel, B.; Mertl, P.; Hernigou, P.; Flecher, X.; Zayni, R.; Bonnin, M.; Jalil, R.; Amzallag, J.; et al. Posterior tibial slope changes after opening- and closing-wedge high tibial osteotomy: A comparative prospective multicenter study. Orthop. Traumatol. Surg. Res. 2012, 98, 68–74. [Google Scholar] [CrossRef]
- Eliasberg, C.D.; Hancock, K.J.; Swartwout, E.; Robichaud, H.; Ranawat, A.S. The Ideal Hinge Axis Position to Reduce Tibial Slope in Opening-Wedge High Tibial Osteotomy Includes Proximalization-Extension and Internal Rotation. Arthroscopy 2021, 37, 1577–1584. [Google Scholar] [CrossRef]
- Jacobi, M.; Villa, V.; Reischl, N.; Demey, G.; Goy, D.; Neyret, P.; Gautier, E.; Magnussen, R.A. Factors influencing posterior tibial slope and tibial rotation in opening wedge high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 2762–2768. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.W.; Park, S.H.; Lee, B.H.; Oh, M.; Chang, M.; Ahn, J.H.; Wang, J.H. The Effect of Hinge Position on Posterior Tibial Slope in Medial Open-Wedge High Tibial Osteotomy. Arthroscopy 2015, 31, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Bae, J.H.; Lim, H.C.; Shon, W.Y.; Kim, C.W.; Cho, J.W. Medial open wedge high tibial osteotomy: The effect of the cortical hinge on posterior tibial slope. Am. J. Sports Med. 2009, 37, 2411–2418. [Google Scholar] [CrossRef] [PubMed]
- Clementz, B.G.; Magnusson, A. Fluoroscopic measurement of tibial torsion in adults. A comparison of three methods. Arch. Orthop. Trauma Surg. 1989, 108, 150–153. [Google Scholar] [CrossRef]
- Schneider, B.; Laubenberger, J.; Jemlich, S.; Groene, K.; Weber, H.M.; Langer, M. Measurement of femoral antetorsion and tibial torsion by magnetic resonance imaging. Br. J. Radiol. 1997, 70, 575–579. [Google Scholar] [CrossRef]
- Hudson, D.; Royer, T.; Richards, J. Ultrasound measurements of torsions in the tibia and femur. J. Bone Joint Surg. Am. 2006, 88, 138–143. [Google Scholar]
- Tamari, K.; Tinley, P.; Briffa, K.; Breidahl, W. Validity and reliability of existing and modified clinical methods of measuring femoral and tibiofibular torsion in healthy subjects: Use of different reference axes may improve reliability. Clin. Anat. 2005, 18, 46–55. [Google Scholar] [CrossRef]
- Amanatullah, D.F.; Ollivier, M.P.; Pallante, G.D.; Abdel, M.P.; Clarke, H.D.; Mabry, T.M.; Taunton, M.J. Reproducibility and precision of CT scans to evaluate tibial component rotation. J. Arthroplast. 2017, 32, 2552–2555. [Google Scholar] [CrossRef]
- Dubousset, J.; Charpak, G.; Skalli, W.; Kalifa, G.; Lazennec, J.Y. EOS stereo-radiography system: Whole-body simultaneous anteroposterior and lateral radiographs with very low radiation dose. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2007, 93 (Suppl. S6), 141–143. (In French) [Google Scholar] [CrossRef]
- Kalifa, G.; Charpak, Y.; Maccia, C.; Fery-Lemonnier, E.; Bloch, J.; Boussard, J.M.; Attal, M.; Dubousset, J.; Adamsbaum, C. Evaluation of a new low-dose digital x-ray device: First dosimetric and clinical results in children. Pediatr. Radiol. 1998, 28, 557–561. [Google Scholar] [CrossRef]
- Li, Q.; Weng, W.J.; Wang, W.J.; Sun, M.H. Introduction of EOS imaging system and its current research status in evaluating clinical value of lower limb force line. China J. Orthop. Traumatol. 2019, 32, 875–878. [Google Scholar]
- Peeters, C.M.M.; Bos, G.; Kempen, D.H.R.; Jutte, P.C.; Faber, C.; Wapstra, F.H. Assessment of spine length in scoliosis patients using EOS imaging: A validity and reliability study. Eur. Spine J. 2022, 31, 3527–3535. [Google Scholar] [CrossRef] [PubMed]
- Folinais, D.; Thelen, P.; Delin, C.; Radier, C.; Catonne, Y.; Lazennec, J.Y. Measuring femoral and rotational alignment: EOS system versus computed tomography. Orthop. Traumatol. Surg. Res. 2013, 99, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Xu, X.; Xu, Q.; Yan, W.; Sun, Z.; Jiang, Q.; Shi, D. Femoral and tibial torsion measurements based on EOS imaging compared to 3D CT reconstruction measurements. Ann. Transl. Med. 2019, 7, 460. [Google Scholar] [CrossRef] [PubMed]
- Chaibi, Y.; Cresson, T.; Aubert, B.; Hausselle, J.; Neyret, P.; Hauger, O.; de Guise, J.A.; Skalli, W. Fast 3D reconstruction of the lower limb using a parametric model and statistical inferences and clinical measurements calculation from biplanar X-rays. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 457–466. [Google Scholar] [CrossRef]
- Reikeras, O.; Bjerkreim, I.; Kolbenstvedt, A. Anteversion of the acetabulum and femoral neck in normals and in patients with osteoarthritis of the hip. Acta Orthop. Scand. 1983, 54, 18–23. [Google Scholar] [CrossRef]
- Liodakis, E.; Doxastaki, I.; Chu, K.; Krettek, C.; Gaulke, R.; Citak, M.; Kenawey, M. Reliability of the assessment of lower limb torsion using computed tomography: Analysis of five different techniques. Skelet. Radiol. 2012, 41, 305–311. [Google Scholar] [CrossRef]
- Reikeras, O.; Hoiseth, A. Torsion of the leg determined by computed tomography. Acta Orthop. Scand. 1989, 60, 330–333. [Google Scholar] [CrossRef]
- Lipps, D.B.; Wilson, A.M.; Ashton-Miller, J.A.; Wojtys, E.M. Evaluation of different methods for measuring lateral tibial slope using magnetic resonance imaging. Am. J. Sports Med. 2012, 40, 2731–2736. [Google Scholar] [CrossRef]
- Hecker, A.; Lerch, T.D.; Egli, R.J.; Liechti, E.F.; Klenke, F.M. The EOS 3D imaging system reliably measures posterior tibial slope. J. Orthop. Surg. Res. 2021, 16, 388. [Google Scholar] [CrossRef]
- Suh, D.W.; Nha, K.W.; Han, S.B.; Cheong, K.; Kyung, B.S. Biplane medial opening-wedge high tibial osteotomy increases posterior tibial slope more than uniplane osteotomy. J. Knee Surg. 2022, 35, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, H.Y.; Lee, D.H. Opening gap width influences distal tibial rotation below the osteotomy site following open wedge high tibial osteotomy. PLoS ONE 2020, 15, e0227969. [Google Scholar] [CrossRef] [PubMed]
- Jo, H.S.; Park, J.S.; Byun, J.H.; Lee, Y.B.; Choi, Y.L.; Cho, S.H.; Moon, D.K.; Lee, S.H.; Hwang, S.C. The effects of different hinge positions on posterior tibial slope in medial open-wedge high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Salaha, Z.F.M.; Ammarullah, M.I.; Abdullah, N.; Aziz, A.U.A.; Gan, H.S.; Abdullah, A.H.; Abdul Kadir, M.R.; Ramlee, M.H. Biomechanical Effects of the Porous Structure of Gyroid and Voronoi Hip Implants: A Finite Element Analysis Using an Experimentally Validated Model. Materials 2023, 16, 3298. [Google Scholar] [CrossRef]
- Hayatbakhsh, Z.; Farahmand, F. Effects of plate contouring quality on the biomechanical performance of high tibial osteotomy fixation: A parametric finite element study. Proc. Inst. Mech. Eng. H 2022, 236, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.S.; Wang, X.; Ding, L.Z.; Zhu, X.P.; Xu, W.F.; Huang, L.X. The best position of bone grafts in the medial open-wedge high tibial osteotomy: A finite element analysis. Comput. Methods Programs Biomed. 2023, 228, 107253. [Google Scholar] [CrossRef]
- Ammarullah, M.I.; Hartono, R.; Supriyono, T.; Santoso, G.; Sugiharto, S.; Permana, M.S. Polycrystalline Diamond as a Potential Material for the Hard-on-Hard Bearing of Total Hip Prosthesis: Von Mises Stress Analysis. Biomedicines 2023, 11, 951. [Google Scholar] [CrossRef]
- Prakoso, A.T.; Basri, H.; Adanta, D.; Yani, I.; Ammarullah, M.I.; Akbar, I.; Ghazali, F.A.; Syahrom, A.; Kamarul, T. The Effect of Tortuosity on Permeability of Porous Scaffold. Biomedicines 2023, 11, 427. [Google Scholar] [CrossRef]
- Trad, Z.; Barkaoui, A.; Chafra, M.; Tavares, J.M.R. Finite element analysis of the effect of high tibial osteotomy correction angle on articular cartilage loading. Proc. Inst. Mech. Eng. H 2018, 232, 553–564. [Google Scholar] [CrossRef]
- Thelen, P.; Delin, C.; Folinais, D.; Radier, C. Evaluation of a new low-dose biplanar system to assess lower-limb alignment in 3D: A phantom study. Skelet. Radiol. 2012, 41, 1287–1293. [Google Scholar] [CrossRef]
- Dubousset, J.; Charpak, G.; Dorion, I.; Skalli, W.; Lavaste, F.; Deguise, J.; Kalifa, G.; Ferey, S. A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: The EOS system. Bull. Acad. Natl. Med. 2005, 189, 287–297; discussion 297–300. (In French) [Google Scholar]
- Dietrich, T.J.; Pfirrmann, C.W.; Schwab, A.; Pankalla, K.; Buck, F.M. Comparison of radiation dose, workflow, patient comfort and financial break-even of standard digital radiography and a novel biplanar low-dose X-ray system for upright full-length lower limb and whole spine radiography. Skelet. Radiol. 2013, 42, 959–967. [Google Scholar] [CrossRef]
- Flecher, X.; Ollivier, M.; Argenson, J.N. Lower limb length and offset in total hip arthroplasty. Orthop. Traumatol. Surg. Res. 2016, 102 (Suppl. S1), S9–S20. [Google Scholar] [CrossRef] [PubMed]
- Orfeuvre, B.; Tonetti, J.; Kerschbaumer, G.; Barthelemy, R.; Moreau-Gaudry, A.; Boudissa, M. EOS stereographic assessment of femoral shaft malunion after intramedullary nailing. A prospective series of 48 patients at 9 months’ follow-up. Orthop. Traumatol. Surg. Res. 2021, 107, 102805. [Google Scholar] [CrossRef] [PubMed]
- Peeters, C.M.M.; Van Houten, L.; Kempen, D.H.R.; Wapstra, F.H.; Jutte, P.C.; van den Akker-Scheek, I.; Faber, C. Assessment of pedicle size in patients with scoliosis using EOS 2D imaging: A validity and reliability study. Eur. Spine J. 2021, 30, 3473–3481. [Google Scholar] [CrossRef]
- Loppini, M.; Pisano, A.; Ruggeri, R.; Della Rocca, A.; Grappiolo, G. Pelvic tilt and functional acetabular position after total hip arthroplasty: An EOS 2D/3D radiographic study. Hip Int. 2023, 33, 365–370. [Google Scholar] [CrossRef]
- Moon, H.S.; Choi, C.H.; Jung, M.; Lee, D.Y.; Kim, J.H.; Kim, S.H. The effect of knee joint rotation in the sagittal and axial plane on the measurement accuracy of coronal alignment of the lower limb. BMC Musculoskelet. Disord. 2020, 21, 470. [Google Scholar] [CrossRef]
- Cho, B.W.; Lee, T.H.; Kim, S.; Choi, C.H.; Jung, M.; Lee, K.Y.; Kim, S.H. Evaluation of the reliability of lower extremity alignment measurements using EOS imaging system while standing in an even weight-bearing posture. Sci. Rep. 2021, 11, 22039. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Knees (n = 30) |
|---|---|
| Sex | |
| Male | 8 (27) |
| Female | 22 (73) |
| Age (years) | 59.9 |
| Height (cm) | 159.8 |
| Weight (kg) | 67.7 |
| Body mass index (kg/m2) | 26.41 |
| Side | |
| Left | 16 (53) |
| Right | 14 (47) |
| Flexion contracture (°) | 4.0 |
| Correction angle (°) | 8.25 (4–15) |
| Concomitant surgery | |
| Medial meniscus repair | 19 (63) |
| Partial medial meniscectomy | 11 (37) |
| Allogenic mesenchymal stem cell transplantation | 2 (7) |
| CT | EOS System | ||||||
|---|---|---|---|---|---|---|---|
| Before MOWHTO (SD) | After MOW1HTO (SD) | Change (SD) | Before MOWHTO (SD) | After MOWHTO (SD) | Change (SD) | p-Value | |
| Femoral torsion (°) | 14.42 (5.87) | 14.59 (6.47) | 0.17 (2.73) | 17.39 (7.28) | 14.96 (9.50) | −2.96 (9.24) | 0.142 |
| Tibial torsion (°) | 25.16 (6.86) | 21.57 (5.21) | −3.59 (2.64) | 26.29 (7.97) | 22.89 (6.37) | −3.39 (7.34) | 0.894 |
| Femorotibial rotation (°) | 0.87 (3.66) | 3.48 (5.14) | 2.61 (3.63) | −1.64 (7.50) | 0.82 (9.49) | 2.46 (10.58) | 0.947 |
| Posterior tibial slope (°) | 12.10 (3.33) | 12.92 (3.66) | 0.82(1.91) | 12.75 (4.26) | 14.64 (4.53) | 1.89 (2.10) | 0.227 |
| Preop. (SD) | Postop. (SD) | Change (SD) | p-Value | |
|---|---|---|---|---|
| Radiologic outcomes | ||||
| Tibial slope (°) | 12.10 (3.33) | 12.92 (3.66) | 0.82 (1.92) | 0.035 * |
| Tibial rotation (°) | 25.16 (6.86) | 21.57 (5.21) | −3.59 (2.64) | <0.001 * |
| Femorotibial rotation (°) | 0.87 (3.66) | 3.48 (5.14) | 2.61 (3.63) | <0.001 * |
| HKAA (°) | 6.29 (2.33) | −1.11 (2.10) | −7.39 (2.74) | <0.001 * |
| MPTA (°) | 84.54 (2.15) | 89.89 (3.29) | 5.36 (3.88) | <0.001 * |
| Clinical outcomes (POD 1Y) | ||||
| ROM (◦) | 131.64 (7.68) | 132.46 (7.39) | 0.82 (2.73) | 0.129 |
| WOMAC score | ||||
| Total | 44.50 (8.68) | 41.21 (4.97) | −3.29 (5.99) | 0.008 * |
| Pain | 9.04 (3.92) | 7.54 (2.44) | −1.50 (2.69) | 0.007 * |
| Function | 30.21 (6.75) | 28.61 (4.32) | −1.61 (4.93) | 0.102 |
| Stiffness | 5.21 (1.15) | 5.07 (1.22) | −0.14 (0.91) | 0.424 |
| HSS score | 71.18 (6.37) | 79.93 (7.13) | 8.75 (3.58) | <0.001 * |
| Change in Tibial Torsion | p | Change in Posterior Tibial Slope | p | |
|---|---|---|---|---|
| Pearson’s Correlation Coefficient (r) | Pearson’s Correlation Coefficient (r) | |||
| Correction angle (°) | 0.150 | 0.377 | 0.186 | 0.269 |
| TOA (°) | −0.060 | 0.730 | 0.027 | 0.878 |
| Flexion contracture (°) | −0.205 | 0.224 | −0.125 | 0.462 |
| Change of tibial torsion | 1.0 | 0.000 | 0.998 | |
| Change of posterior tibial slope | 0.000 | 0.998 | 1.0 | |
| Change of clinical outcomes (POD 1Y) | ||||
| ROM (°) | 0.173 | 0.306 | −0.036 | 0.834 |
| WOMAC score | ||||
| Total | 0.104 | 0.538 | −0.130 | 0.445 |
| Pain | 0.110 | 0.515 | −0.156 | 0.358 |
| Function | 0.05 | 0.769 | −0.056 | 0.742 |
| Stiffness | 0.172 | 0.309 | −0.050 | 0.770 |
| HSS score | −0.113 | 0.505 | 0.250 | 0.135 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, H.-J.; Choi, J.-K.; Heo, Y.-M.; Moon, S.-J.; Oh, B.-H. Changes in Parameters after High Tibial Osteotomy: Comparison of EOS System and Computed Tomographic Analysis. J. Clin. Med. 2023, 12, 5638. https://doi.org/10.3390/jcm12175638
Yoo H-J, Choi J-K, Heo Y-M, Moon S-J, Oh B-H. Changes in Parameters after High Tibial Osteotomy: Comparison of EOS System and Computed Tomographic Analysis. Journal of Clinical Medicine. 2023; 12(17):5638. https://doi.org/10.3390/jcm12175638
Chicago/Turabian StyleYoo, Hyun-Jin, Jae-Kyu Choi, Youn-Moo Heo, Sung-Jun Moon, and Byung-Hak Oh. 2023. "Changes in Parameters after High Tibial Osteotomy: Comparison of EOS System and Computed Tomographic Analysis" Journal of Clinical Medicine 12, no. 17: 5638. https://doi.org/10.3390/jcm12175638