
Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
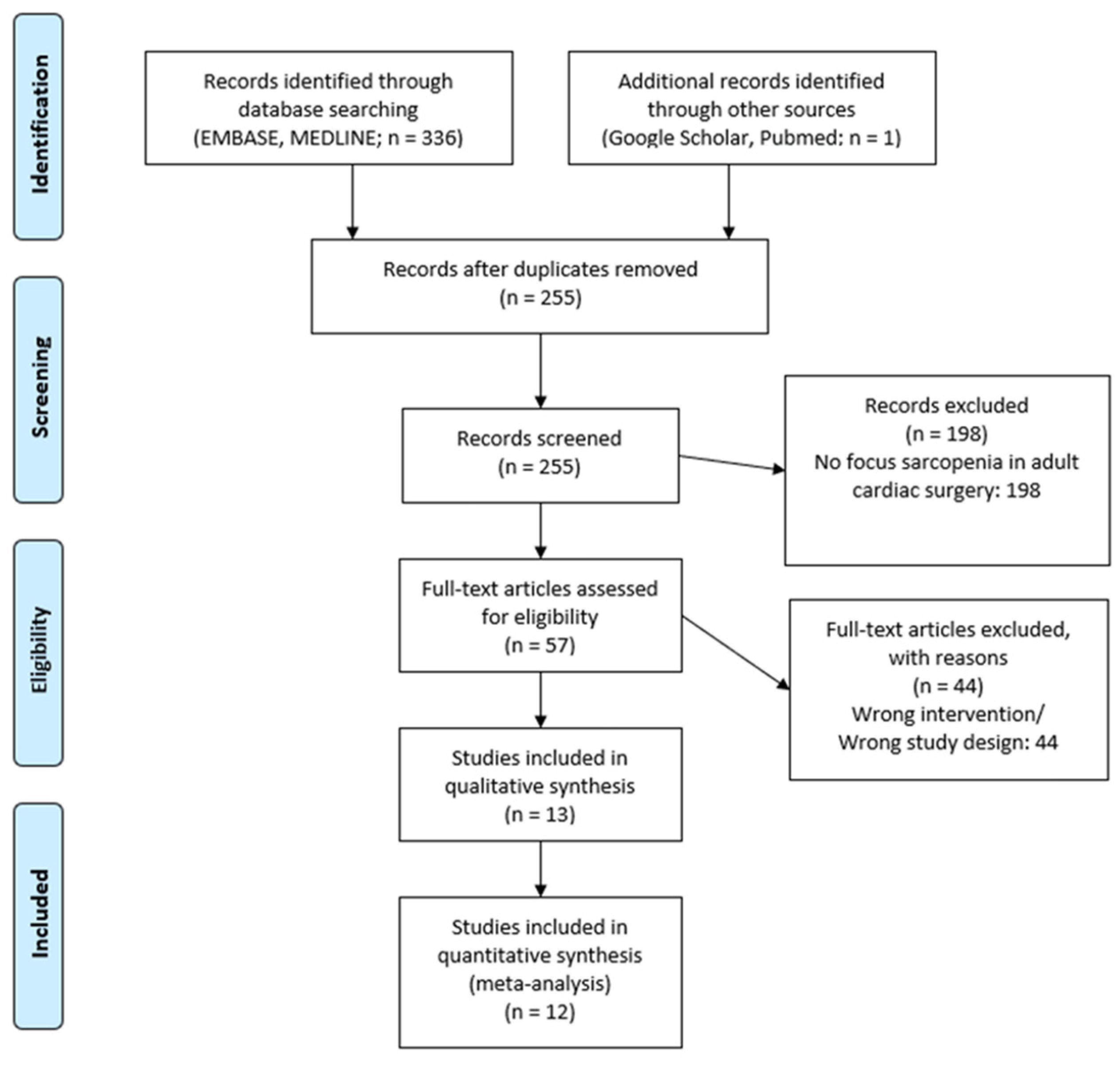
2.1. Literature Search Strategy
2.2. Study Inclusion and Exclusion Criteria
2.3. Data Extraction and Critical Appraisal
2.4. Data Analysis
2.5. Sensitivity Analysis
3. Results
3.1. Description of Studies
3.2. Baseline Characteristics
3.3. Primary and Secondary Outcomes
3.3.1. Early Mortality and Late Mortality
3.3.2. Overall Surgery Time
3.3.3. CBP Time
3.3.4. CC Time
3.3.5. Hospital LOS
3.3.6. ICU LOS
3.3.7. Intubation Time
3.3.8. Postoperative Arrhythmia
3.3.9. Stroke
3.3.10. Sternal Wound Infection
3.3.11. Postoperative Need for Dialysis
3.3.12. Discharge to Care Home
3.4. Sensitivity Analysis: Hospital LOS
3.5. Risk of Bias across the Studies
4. Discussion
4.1. Sarcopenia and Mortality
4.2. Surgical Time
4.3. Infection Rates
4.4. Functional Outcomes
- (a)
- ICU Length of Stay: The longer ICU stay for sarcopenic patients may be due to their lower physiological reserve and increased vulnerability to complications. Sarcopenia, characterised by a loss of muscle mass and function, can lead to frailty, which is associated with a higher risk of adverse outcomes, including prolonged ICU stay. This is supported by a study by Moisey et al., 2013 [34], which found that sarcopenic patients had a longer ICU stay after emergency abdominal surgery.
- (b)
- Dialysis: The higher likelihood of requiring dialysis in sarcopenic patients probably relates to their increased risk of acute kidney injury (AKI) postoperatively. Sarcopenia may contribute to AKI through various mechanisms, including inflammatory pathway activation following chronic inflammation and increased susceptibility to nephrotoxic agents [35]. A study by Bang et al. [35] found that sarcopenia was an independent risk factor for AKI in patients undergoing abdominal aortic aneurysm surgery.
- (c)
- Care Home discharge: The higher rate of care home discharge for sarcopenic patients may reflect their poorer functional status and increased need for assistance with daily activities postoperatively. Sarcopenia is associated with physical disability and reduced independence, which may necessitate care home admission. This is consistent with a study by Landi et al., 2012 [36], which found that sarcopenic older adults were more likely to be institutionalised.
- (d)
- Intubation Time: The longer intubation time for sarcopenic patients may be due to their increased risk of respiratory complications. Sarcopenia can impair respiratory muscle function, leading to reduced lung volumes and ineffective cough, which can prolong the need for mechanical ventilation. A study by Puthucheary et al., 2013 [37] found that ICU-acquired weakness, which is often associated with sarcopenia, was a predictor of prolonged mechanical ventilation.
4.5. Measurements of Sarcopenia in Clinical Practice
4.6. Sarcopenia and Frailty
4.7. Recommendations for Optimising Cardiac Surgery Outcomes in Sarcopenic Patients
- Preoperative identification of sarcopenia: Early identification of sarcopenia can allow for preoperative interventions to improve patient outcomes. This can be achieved through simple screening tools or more comprehensive assessments such as CT or MRI scans.
- Preoperative optimisation: Once sarcopenia is identified, preoperative optimisation strategies should be implemented. This could include nutritional supplementation, physical therapy, and exercise programs aimed at increasing muscle mass and strength.
- Risk stratification: Sarcopenic patients should be considered high-risk surgical candidates. This should be considered when planning the surgical approach and postoperative care.
- Intraoperative care: Consideration should be given to minimizing operative time and blood loss, as sarcopenic patients may be more susceptible to intraoperative complications.
- Postoperative rehabilitation: Early mobilisation and physical therapy should be initiated postoperatively to prevent further muscle loss and to promote recovery.
- Nutritional support: Postoperative nutritional support should be provided to meet the increased protein and calorie needs of sarcopenic patients and to support muscle recovery.
- Multidisciplinary approach: The care of sarcopenic patients should involve a multidisciplinary team, including surgeons, anaesthesiologists, dietitians, physical therapists, and geriatricians. This can ensure a comprehensive approach to the management of sarcopenia and its associated risks.
- Patient education: Patients should be educated about the implications of sarcopenia and the steps they can take to improve their muscle health. This can empower patients to take an active role in their care and recovery.
- Research: Further research should be conducted to better understand the impact of sarcopenia on cardiac surgery outcomes and to develop effective interventions for this patient population.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Xia, L.; Zhao, R.; Wan, Q.; Wu, Y.; Zhou, Y.; Wang, Y.; Cui, Y.; Shen, X.; Wu, X. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med. 2020, 9, 7964–7978. [Google Scholar] [CrossRef]
- He, N.; Zhang, Y.; Zhang, L.; Zhang, S.; Ye, H. Relationship Between Sarcopenia and Cardiovascular Diseases in the Elderly: An Overview. Front. Cardiovasc. Med. 2021, 8, 743710. [Google Scholar] [CrossRef]
- Pring, E.T.; Gould, L.E.; Malietzis, G.; Lung, P.; Bharal, M.; Fadodun, T.; Bassett, P.; Naghibi, M.; Taylor, C.; Drami, I.; et al. BiCyCLE NMES—Neuromuscular electrical stimulation in the perioperative treatment of sarcopenia and myosteatosis in advanced rectal cancer patients: Design and methodology of a phase II randomised controlled trial. Trials 2021, 22, 621. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.-C.; Hwang, A.-C.; Liu, L.-K.; Lee, W.-J.; Chen, L.-Y.; Wu, Y.-H.; Huang, C.-Y.; Hung, C.-H.; Wang, C.-J.; Lin, M.-H.; et al. FNIH-defined Sarcopenia Predicts Adverse Outcomes Among Community-Dwelling Older People in Taiwan: Results From I-Lan Longitudinal Aging Study. J. Gerontol. Ser. A 2017, 73, 828–834. [Google Scholar] [CrossRef] [PubMed]
- De Santo, L.S.; Moscariello, C.; Zebele, C. Implications of obesity in cardiac surgery: Pattern of referral, physiopathology, complications, prognosis. J. Thorac. Dis. 2018, 10, 4532–4539. [Google Scholar] [CrossRef] [PubMed]
- Zhigalov, K.; Oliveira Sá, M.P.B.; Rad, A.A.; Vardanyan, R.; Goerdt, L.; Chrosch, T.; Zubarevich, A.; Wendt, D.; Pizanis, N.; Koch, A.; et al. The Impact of Obesity on Left Ventricular Assist Device Outcomes. Medicina 2020, 56, 556. [Google Scholar] [CrossRef]
- Rothman, K.J. BMI-related errors in the measurement of obesity. Int. J. Obes. 2008, 32, S56–S59. [Google Scholar] [CrossRef]
- Zhang, X.; Xie, X.; Dou, Q.; Liu, C.; Zhang, W.; Yang, Y.; Deng, R.; Cheng, A.S.K. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: A updated meta-analysis. BMC Geriatr. 2019, 19, 183. [Google Scholar] [CrossRef]
- Shibasaki, I.; Ouchi, M.; Fukuda, T.; Tsuchiya, G.; Ogawa, H.; Takei, Y.; Tezuka, M.; Kanazawa, Y.; Katayanagi, S.; Nozawa, N.; et al. Effect of sarcopenia on hospital stay from post cardiac surgery to discharge. IJC Heart Vasc. 2022, 39, 101003. [Google Scholar] [CrossRef]
- Kondo, Y.; Suzuki, T.; Enomoto, M.; Takashima, N.; Kinoshita, T. Psoas muscle size, possible sarcopenia and frailty, and long-term survival in elderly patients after isolated surgical aortic valve replacement for aortic stenosis. Indian J. Thorac. Cardiovasc. Surg. 2022, 38, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Okamura, H.; Kimura, N.; Mieno, M.; Yuri, K.; Yamaguchi, A. Preoperative sarcopenia is associated with late mortality after off-pump coronary artery bypass grafting. Eur. J. Cardio-Thorac. Surg. 2020, 58, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Yuenyongchaiwat, K.; Kulchanarat, C.; Satdhabudha, O. Sarcopenia in open heart surgery patients: A cohort study. Heliyon 2020, 6, e05759. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Song, I.-K.; Nam, J.-S.; Lee, S.-W.; Lee, E.-H.; Choi, I.-C. Sarcopenia as a prognostic factor for outcomes after isolated tricuspid valve surgery. J. Cardiol. 2020, 76, 585–592. [Google Scholar] [CrossRef]
- Kurumisawa, S.; Kawahito, K. The psoas muscle index as a predictor of long-term survival after cardiac surgery for hemodialysis-dependent patients. J. Artif. Organs 2019, 22, 214–221. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Kern, J.A.; Lim, D.S.; Teman, N.R.; Ailawadi, G. Psoas Muscle Size Predicts Risk-Adjusted Outcomes After Surgical Aortic Valve Replacement. Ann. Thorac. Surg. 2018, 106, 39–45. [Google Scholar] [CrossRef]
- Yamashita, M.; Kamiya, K.; Matsunaga, A.; Kitamura, T.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Nakamura, T.; Maekawa, E.; et al. Prognostic Value of Psoas Muscle Area and Density in Patients Who Undergo Cardiovascular Surgery. Can. J. Cardiol. 2017, 33, 1652–1659. [Google Scholar] [CrossRef]
- Ikeno, Y.; Koide, Y.; Abe, N.; Matsueda, T.; Izawa, N.; Yamazato, T.; Miyahara, S.; Nomura, Y.; Sato, S.; Takahashi, H.; et al. Impact of sarcopenia on the outcomes of elective total arch replacement in the elderly†. Eur. J. Cardio-Thorac. Surg. 2017, 51, 1135–1141. [Google Scholar] [CrossRef]
- Teng, C.-H.; Chen, S.-Y.; Wei, Y.-C.; Hsu, R.-B.; Chi, N.-H.; Wang, S.-S.; Chen, Y.-S.; Chen, C.C.-H. Effects of sarcopenia on functional improvement over the first year after cardiac surgery: A cohort study. Eur. J. Cardiovasc. Nurs. 2019, 18, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.-L.; Liu, Z.; Zang, W.-F.; Zhang, P.; Zou, H.-B.; Dong, W.-X.; Chen, W.-H.; Yan, X.-L.; Yu, Z. Thoracic sarcopenia predicts clinical outcomes in patients undergoing coronary artery bypass grafting: A 6-year cohort study. Asian J. Surg. 2023, 46, 291–298. [Google Scholar] [CrossRef]
- Kiriya, Y.; Toshiaki, N.; Shibasaki, I.; Ogata, K.; Ogawa, H.; Takei, Y.; Tezuka, M.; Seki, M.; Kato, T.; Lefor, A.K.; et al. Sarcopenia assessed by the quantity and quality of skeletal muscle is a prognostic factor for patients undergoing cardiac surgery. Surg. Today 2020, 50, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.K. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef] [PubMed]
- Englesbe, M.J.; Patel, S.P.; He, K.; Lynch, R.J.; Schaubel, D.E.; Harbaugh, C.; Holcombe, S.A.; Wang, S.C.; Segev, D.L.; Sonnenday, C.J. Sarcopenia and Mortality after Liver Transplantation. J. Am. Coll. Surg. 2010, 211, 271–278. [Google Scholar] [CrossRef]
- Malietzis, G.; Currie, A.C.; Athanasiou, T.; Johns, N.; Anyamene, N.; Glynne-Jones, R.; Kennedy, R.H.; Fearon, K.C.H.; Jenkins, J.T. Influence of body composition profile on outcomes following colorectal cancer surgery. Br. J. Surg. 2016, 103, 572–580. [Google Scholar] [CrossRef]
- Wayda, B.; Clemons, A.; Givens, R.C.; Takeda, K.; Takayama, H.; Latif, F.; Restaino, S.; Naka, Y.; Farr, M.A.; Colombo, P.C.; et al. Socioeconomic Disparities in Adherence and Outcomes After Heart Transplant: A UNOS (United Network for Organ Sharing) Registry Analysis. Circ. Heart Fail. 2018, 11, e004173. [Google Scholar] [CrossRef]
- Swan, L.; Warters, A.; O’Sullivan, M. Socioeconomic Inequality and Risk of Sarcopenia in Community-Dwelling Older Adults. Clin. Interv. Aging 2021, 16, 1119–1129. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Koster, A.; Schols, J.M.G.A.; Meijers, J.M.M.; Halfens, R.J.G.; Gudnason, V.; Eiriksdottir, G.; Siggeirsdottir, K.; Sigurdsson, S.; Jónsson, P.V.; et al. Physical activity and incidence of sarcopenia: The population-based AGES—Reykjavik Study. Age Ageing 2016, 45, 614–620. [Google Scholar] [CrossRef]
- Fukuda, Y.; Yamamoto, K.; Hirao, M.; Nishikawa, K.; Nagatsuma, Y.; Nakayama, T.; Tanikawa, S.; Maeda, S.; Uemura, M.; Miyake, M.; et al. Sarcopenia is associated with severe postoperative complications in elderly gastric cancer patients undergoing gastrectomy. Gastric Cancer 2015, 19, 986–993. [Google Scholar] [CrossRef]
- Lieffers, J.R.; Bathe, O.F.; Fassbender, K.; Winget, M.; Baracos, V.E. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br. J. Cancer 2012, 107, 931–936. [Google Scholar] [CrossRef]
- Thelwall, S.; Harrington, P.; Sheridan, E.; Lamagni, T.; Thelwall, S.; Harrington, P.; Sheridan, E.; Lamagni, T. Impact of obesity on the risk of wound infection following surgery: Results from a nationwide prospective multicentre cohort study in England. Clin. Microbiol. Infect. 2015, 21, 1008.e1–1008.e8. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, R.; Syrjänen, J. Obesity and the risk and outcome of infection. Int. J. Obes. 2013, 37, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Mourtzakis, M.; Cotton, A.B.; Premji, T.; Heyland, D.K.; Wade, E.C.; Bulger, E.; Kozar, A.R. Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit. Care 2013, 17, R206. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.-Y.; Jun, I.-G.; Lee, J.-B.; Ko, Y.-S.; Kim, K.-W.; Jeong, J.-H.; Kim, S.-H.; Song, J.-G. Impact of Sarcopenia on Acute Kidney Injury after Infrarenal Abdominal Aortic Aneurysm Surgery: A Propensity Matching Analysis. Nutrients 2021, 13, 2212. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin. Nutr. 2012, 31, 652–658. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef]
- Lanza, E.; Masetti, C.; Messana, G.; Muglia, R.; Pugliese, N.; Ceriani, R.; de Nalda, A.L.; Rimassa, L.; Torzilli, G.; Poretti, D.; et al. Sarcopenia as a predictor of survival in patients undergoing bland transarterial embolization for unresectable hepatocellular carcinoma. PLoS ONE 2020, 15, e0232371. [Google Scholar] [CrossRef]
- Van der Werf, A.; Langius, J.A.; De Van Der Schueren, M.A.; Nurmohamed, S.A.; Van Der Pant, K.A.; Blauwhoff-Buskermolen, S.; Wierdsma, N.L. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef]
- Gingrich, A.; Volkert, D.; Kiesswetter, E.; Thomanek, M.; Bach, S.; Sieber, C.C.; Zopf, Y. Prevalence and overlap of sarcopenia, frailty, cachexia and malnutrition in older medical inpatients. BMC Geriatr. 2019, 19, 120. [Google Scholar] [CrossRef]
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Patient Numbers (SP.NSP) | Sarcopenia Definition | Study Design | Country | AGE | BMI | LVEF % | Psoas Muscle Area Index (mm2/m2) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean SP | SD SP | Mean NSP | SD NSP | Mean SP | SD SP | Mean NSP | SD NSP | Mean SP | SD SP | Mean NSP | SD NSP | Mean SP | SD SP | Mean NSP | SD NSP | |||||
| Shibasaki et al., 2022 | 72/120 | SMI: total body muscle | R | Japan | 73.8 | 8.8 | 67.0 | 10.1 | 21.5 | 3.0 | 24.5 | 4.3 | 56.2 | 13.3 | 59.4 | 12.3 | NA | NA | NA | NA |
| Kondo et al., 2022 | 29/111 | PMI | R | Japan | 81.0 | 5.8 | 77.3 | 4.7 | 21.6 | 4.2 | 22.8 | 3.7 | 62.2 | 9.0 | 62.1 | 9.0 | 704.0 | 112.0 | 1083.0 | 290.0 |
| Okamura et al., 2020 | 76/228 | PMI | P | Japan | 69.9 | 8.9 | 66.6 | 9.7 | 21.6 | 3.0 | 24.1 | 3.3 | 55.5 | 14.4 | 56.4 | 13.9 | 168.0 | 37.0 | 283.0 | 65.0 |
| Yuenyongchaiwat et al., 2020 | 43/117 | AWGS | R | Thailand | 66.4 | 10.7 | 59.1 | 11.2 | NA | NA | NA | NA | 53.3 | 15.1 | 51.9 | 13.7 | NA | NA | NA | NA |
| Oh et al., 2020 | 73/71 | SMI: pec. major & erector spinae | R | South Korea | 59.5 | 13.1 | 60.4 | 10.6 | 22.6 | 3.2 | 24.4 | 3.0 | 60.0 | 3.0 | 60.0 | 3.0 | NA | NA | NA | NA |
| Kurumisawa et al., 2019 | 35/103 | PMI | R | Japan | 67 | 10 | 66 | 9 | 19.5 | 2.9 | 22.6 | 3.8 | 50 | 15 | 52 | 16 | NA | NA | NA | NA |
| Hawkins et al., 2018 | 60/180 | PMI | R | USA | 81 | 2 | 80 | 2.5 | NA | NA | NA | NA | 57 | 3 | 57 | 2.5 | 670.0 | 220.0 | 1060.0 | 280.0 |
| Yamashita et al., 2017 | 387/386 | PMI | R | Japan | 65.5 | 13.2 | 64.4 | 13.1 | 23.4 | 3.53 | 21.1 | 3.45 | 57.8 | 12.5 | 56.7 | 13.1 | 401 | 78 | 667 | 111 |
| Ikeno et al., 2017 | 81/185 | PMI | R | Japan | 76.2 | 5.6 | 45.7 | 5.7 | 22.5 | 3.4 | 23.8 | 2.9 | NA | NA | NA | NA | NA | NA | NA | NA |
| Teng et al., 2019 | 67/175 | EWGSOP | R | Japan | 66.4 | 12.4 | 58.9 | 11.2 | 21.7 | 2.7 | 26.2 | 3.5 | 64.1 | 11.8 | 62.3 | 13.1 | NA | NA | NA | NA |
| Shen et al., 2023 | 44/294 | SMI: T12 level muscle | P | China | 65.0 | 8.2 | 65.0 | 7.4 | 25.0 | 2.9 | 24.4 | 3.1 | NA | NA | NA | NA | NA | NA | NA | NA |
| Kiriya et al., 2020 | 63/143 | PMI | R | Japan | 75.1 | 5.5 | 73.9 | 5.5 | 22.7 | 3.4 | 23.4 | 3.7 | 57.1 | 13.6 | 60.8 | 34.9 | 448.0 | 143.5 | 1005.0 | 312.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansaripour, A.; Arjomandi Rad, A.; Koulouroudias, M.; Angouras, D.; Athanasiou, T.; Kourliouros, A. Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5573. https://doi.org/10.3390/jcm12175573
Ansaripour A, Arjomandi Rad A, Koulouroudias M, Angouras D, Athanasiou T, Kourliouros A. Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(17):5573. https://doi.org/10.3390/jcm12175573
Chicago/Turabian StyleAnsaripour, Ali, Arian Arjomandi Rad, Marinos Koulouroudias, Dimitrios Angouras, Thanos Athanasiou, and Antonios Kourliouros. 2023. "Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 17: 5573. https://doi.org/10.3390/jcm12175573