
Prevalence of Peri-Implant Disease in Patients with Stage III or IV Periodontitis: Results of a Long-Term Follow-Up from a Specialized Periodontal Practice

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
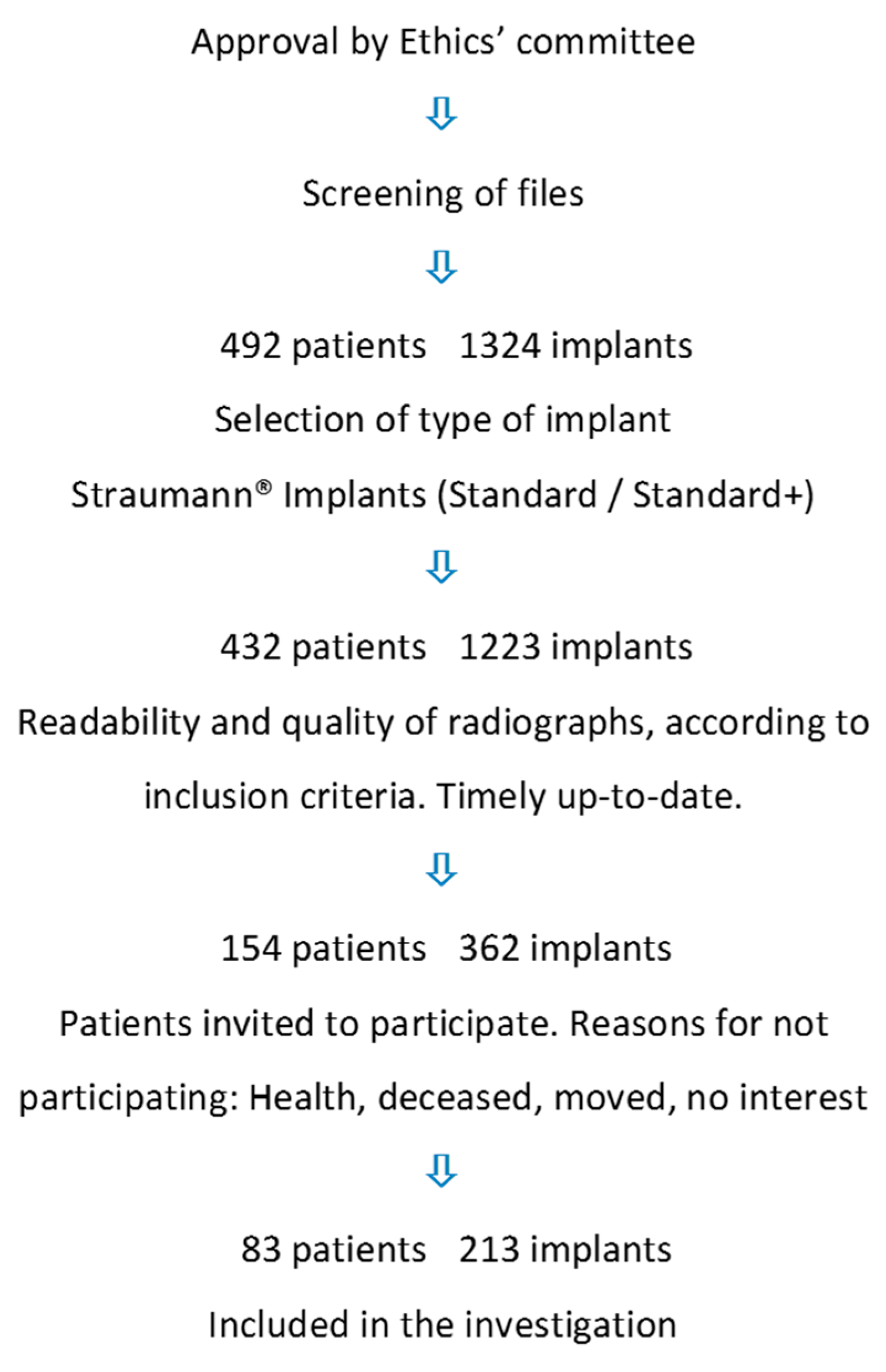
2.2. Population
- Treatment with a Straumann® tissue-level implant (Standard/Standard Plus; Straumann®, Basel, Switzerland), with the surface of the implants coated with either SLA®- or SLActive®.
- One radiograph from the time point of insertion and one from an arbitrary later date should be available. The last radiographs should be up-to-date, from within one year prior to examination.
- Insufficient radiographs;
- Other types of implants from the same manufacturer, or other brands of implants.
- Missing or unanalyzable radiographs, or radiographs failing to display the implant in full length.
2.3. Clinical Examination
2.4. Radiographic Examination
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brånemark, P.I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; de Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Sennerby, L. Dental implants: Matters of course and controversies. Periodontology 2000 2008, 47, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Fillion, M.; Aubazac, D.; Bessadet, M.; Allègre, M.; Nicolas, E. The impact of implant treatment on oral health related quality of life in a private dental practice: A prospective cohort study. Health Qual. Life Outcomes 2013, 11, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Karoussis, I.; Bürgin, W.; Brägger, U.; Lang, N.P. Patients’ satisfaction following implant therapy. A 10-year prospective cohort study. Clin. Oral Implants Res. 2005, 16, 185–193. [Google Scholar] [CrossRef]
- Smith, M.M.; Knight, E.T.; Al-Harthi, L.; Leichter, J.W. Chronic Periodontitis and implant dentistry. Periodontology 2000 2017, 74, 63–73. [Google Scholar] [CrossRef]
- Ferreira, S.D.; Martins, C.C.; Amaral, S.A.; Vieira, T.R.; Albuquerque, B.N.; Cota, L.O.M.; Esteves Lima, R.P.; Costa, F.O. Periodontitis as a risk factor for peri-implantitis: Systematic review and meta-analysis of observational studies. J. Dent. 2018, 79, 1–10. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bonino, F.; Aglietta, M.; Dalmasso, P. Ten-year results of a three arms prospective cohort study on implants in periodontally compromised patients. Part 2: Clinical results. Clin. Oral Implants Res. 2012, 23, 389–395. [Google Scholar] [CrossRef]
- Roccuzzo, A.; Imber, J.-C.; Marruganti, C.; Salvi, G.E.; Ramieri, G.; Roccuzzo, M. Clinical outcomes of dental implants in patients with and without history of periodontitis: A 20-year prospective study. J. Clin. Periodontol. 2022, 49, 1346–1356. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Scribante, A. Oral Microbiota in Patients with Peri-Implant Disease: A Narrative Review. Appl. Sci. 2022, 12, 3250–3260. [Google Scholar] [CrossRef]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, A.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Periimplant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S286–S291. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S278–S285. [Google Scholar] [CrossRef] [PubMed]
- Amodeo, A.A.; Butera, A.; Lattari, M.; Stablum, G.; Abbinante, A.; Agneta, M.T.; Lanzetti, J.; Tomassi, D.; Piscicelli, S.; Luperini, M.; et al. Consensus Report of the Technical-Scientific Associations of Italian Dental Hygienists and the Academy of Advanced Technologies in Oral Hygiene Sciences on the Non-Surgical Treatment of Peri-Implant Disease. Int. J. Environ. Res. Public Health 2023, 20, 2268–2290. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886–902. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Berglundh, T.; Schwarz, F.; Chapple, I.; Jepsen, S.; Sculean, A.; Kebschull, M.; Papapanou, P.N.; Tonetti, M.S.; Sanz, M.; et al. Prevention and treatment of peri-implant diseases—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2023, 50 (Suppl. 26), 4–76. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants; Merete Aass, A.; et al. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 40–60. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 286–291. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Heitz, F.; Lang, N.P. Implant Disease Risk Assessment IDRA—A tool for preventing peri-implant disease. Clin. Oral Implants Res. 2020, 31, 397–403. [Google Scholar] [CrossRef]
- Lang, N.P.; Tonetti, M.S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev. Dent. 2003, 1, 7–16. [Google Scholar]
- Johannsen, A.; Susin, C.; Gustafsson, A. Smoking and inflammation: Evidence for a synergistic role in chronic disease. Periodontology 2000 2014, 64, 111–126. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38–40. [Google Scholar] [CrossRef]
- Buser, D.; Weber, H.P.; Lang, N.P. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin. Oral Implants Res. 1990, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Bouri, A., Jr.; Bissada, N.; Al-Zahrani, M.S.; Faddoul, F.; Nouneh, I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int. J. Oral Maxillofac. Implants 2008, 23, 323–326. [Google Scholar] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S149–S161. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Lindhe, J. Peri-implant health. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S230–S236. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S237–S245. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S246–S266. [Google Scholar] [CrossRef]
- Aguirre-Zorzano, L.A.; Estefania-Fresco, R.; Telletxea, O.; Bravo, M. Prevalence of peri-implant inflammatory disease in patients with a history of periodontal disease who receive supportive periodontal therapy. Clin. Oral Implants Res. 2015, 26, 1338–1344. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S68–S77. [Google Scholar] [CrossRef]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S152–S157. [Google Scholar] [CrossRef] [PubMed]
- Stiesch, M.; Grischke, J.; Schaefer, P.; Heitz-Mayfield, L.J.A. Supportive care for the prevention of disease recurrence/progression following peri-implantitis treatment: A systematic review. J. Clin. Periodontol. 2023, 50 (Suppl. 26), 113–134. [Google Scholar] [CrossRef]
- Schou, S.; Holmstrup, P.; Stoltze, K.; Hjørting-Hansen, E.; Fiehn, N.E.; Skovgaard, L.T. Probing around implants and teeth with healthy or inflamed peri-implant mucosa/gingiva. Clin. Oral Implants Res. 2002, 13, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Rühling, A.; Jepsen, K.; Ohlenbusch, B.; Albers, H.K. Progressive peri-implantitis. Incidence and prediction of peri-implant attachment loss. Clin. Oral Implants Res. 1996, 7, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Langer, B. The successful use of osseointegrated implants for the treatment of the recalcitrant periodontal patient. J. Periodontol. 1995, 66, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Carra, M.C.; Rangé, H.; Swerts, P.J.; Tuand, K.; Vandamme, K.; Bouchard, P. Effectiveness of implant-supported fixed partial denture in patients with history of periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2022, 49 (Suppl. 24), 208–223. [Google Scholar] [CrossRef] [PubMed]
- Carra, M.C.; Blanc-Sylvestre, N.; Courtet, A.; Bouchard, P. Primordial and primary prevention of peri-implant diseases: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50 (Suppl. 26), 77–112. [Google Scholar] [CrossRef]
- Mameno, T.; Wada, M.; Otsuki, M.; Okuno, I.; Ozeki, K.; Tahara, A.; Ikebe, K. Risk indicators for marginal bone resorption around implants in function for at least 4 years: A retrospective longitudinal study. J. Periodontol. 2020, 91, 37–45. [Google Scholar] [CrossRef]
- Wada, M.; Mameno, T.; Onodera, Y.; Matsuda, H.; Daimon, K.; Ikebe, K. Prevalence of peri-implant disease and risk indicators in a Japanese population with at least 3 years in function—A multicentre retrospective study. Clin. Oral Implants Res. 2019, 30, 111–120. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Level | Variables | Values | |
|---|---|---|---|
| Patient | Sex | male | female |
| Smoke status | non-smoker/former smoker | smoker | |
| SPT compliance | non/infrequently | frequently | |
| FMPS | ≤20% | >20% | |
| # lost teeth | count | ||
| # implants | ≤2 implants | >2 implants | |
| Implant | Implant type | Straumann® Standard | Straumann® Standard Plus |
| Implant surface | SLA | SLAactive | |
| Years in function | years | ||
| Patient age at insertion | years | ||
| Implant location | mandible | maxilla | |
| Outcome variable: peri-implant condition | healthy | inflammation | |
| Variable | Outcome |
|---|---|
| Patients | 83 |
| age at insertion (years; mean (SD); range) | 55.8 (9.27); 32–76 |
| men/women (n) | 40/43 |
| mean residual teeth per patient (mean (SD); range) | 18.7 (4.88); 7–27 |
| implants (n) | 213 |
| mean implants per patient (mean (SD); range) | 2.6 (1.87); 1–10 |
| Smoking habits (n/% (pack years)) | |
| never smoked or former smoker (>5 years) | 72/86.7%/(-) |
| smoker | 11/13.3% (32.2) |
| Periodontal condition (n patients/%) [30] | |
| Treated periodontitis patients with stable conditions | 12/14.5% |
| Treated periodontitis patients with some inflammation | 9/10.8% |
| Treated periodontitis patients with unstable conditions | 62/74.7% |
| Implant-based diagnosis (n patients/%) [26,27,28] | |
| patients with all implants showing peri-implant healthy conditions | 20/24.1% |
| patients with at least one implant with peri- implant mucositis | 55/66.3% |
| patients with at least one implant with peri- implantitis | 8/9.6% |
| FMPS (%; mean (SD)) [22] | 25.3 (13.43) |
| FMBS (%; mean (SD)) | 16.2 (9.10) |
| Maintenance (SPT; n/%) | |
| no or sporadic maintenance | 12/14.5% |
| regular maintenance | 71/85.5% |
| Peri-Implant Diagnosis | Patients | Implants | Mean Implants/Patient |
|---|---|---|---|
| Healthy Peri-implant mucositis only | 20 | 32 | 1.6 |
| 27 | 48 | 1.8 | |
| Peri-implantitis only | 1 | 1 | 1 |
| Combination health and PI-M | 28 | 97 | 3.5 |
| Combination health and P-I | 1 | 2 | 2 |
| Combination PI-M and P-I | 2 | 7 | 3.5 |
| Combination of all 3 diagnoses | 4 | 26 | 6.5 |
| Total | 83 | 213 |
| Variable | Outcome |
|---|---|
| Implant in function (years; mean (SD), range) | 8.67 (2.57), 5–16 |
| 5–10 years (n/%) | 136/63.8% |
| ≥10 years (n/%) | 77/36.2% |
| Position (n/%) | 12/14.5% |
| maxilla | 9/10.8% |
| mandible | 62/74.7% |
| Distribution of implants in regards to the surface in jaws (n/%) | |
| maxilla/SLA® surface | 76/35.7% |
| maxilla/SLActive® surface | 75/35.2% |
| mandible/SLA® surface | 35/16.4% |
| mandible/SLActive® surface | 27/12.7% |
| Implant diagnosis (n/%) [12] | |
| implants with healthy peri-implant conditions | 79/37.1% |
| implants with peri-implant mucositis | 125/58.7% |
| implants with peri-implantitis | 9/4.2% |
| Implant Disease Risk Assessment (IDRA) [19] (n implants/%) | |
| IDRA score “low risk” | 0/0% |
| IDRA score “moderate risk” | 68/31.9% |
| IDRA score “high risk” | 145/68.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jervøe-Storm, P.-M.; Marder, M.; Hagner, M.; Menn, I.; Menn, P.; Jepsen, S. Prevalence of Peri-Implant Disease in Patients with Stage III or IV Periodontitis: Results of a Long-Term Follow-Up from a Specialized Periodontal Practice. J. Clin. Med. 2023, 12, 5547. https://doi.org/10.3390/jcm12175547
Jervøe-Storm P-M, Marder M, Hagner M, Menn I, Menn P, Jepsen S. Prevalence of Peri-Implant Disease in Patients with Stage III or IV Periodontitis: Results of a Long-Term Follow-Up from a Specialized Periodontal Practice. Journal of Clinical Medicine. 2023; 12(17):5547. https://doi.org/10.3390/jcm12175547
Chicago/Turabian StyleJervøe-Storm, Pia-Merete, Michael Marder, Martin Hagner, Ina Menn, Philipp Menn, and Søren Jepsen. 2023. "Prevalence of Peri-Implant Disease in Patients with Stage III or IV Periodontitis: Results of a Long-Term Follow-Up from a Specialized Periodontal Practice" Journal of Clinical Medicine 12, no. 17: 5547. https://doi.org/10.3390/jcm12175547