
Lung Transplantation Outcomes in Recipients Aged 70 Years or Older and the Impact of Center Volume
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Processing
2.3. Statistical Methods
3. Results
3.1. Sample
3.2. Donor Characteristics
3.3. Recipient Characteristics
3.4. Surgical and Pre-Transplant Factors
3.5. Post-Surgical Outcomes
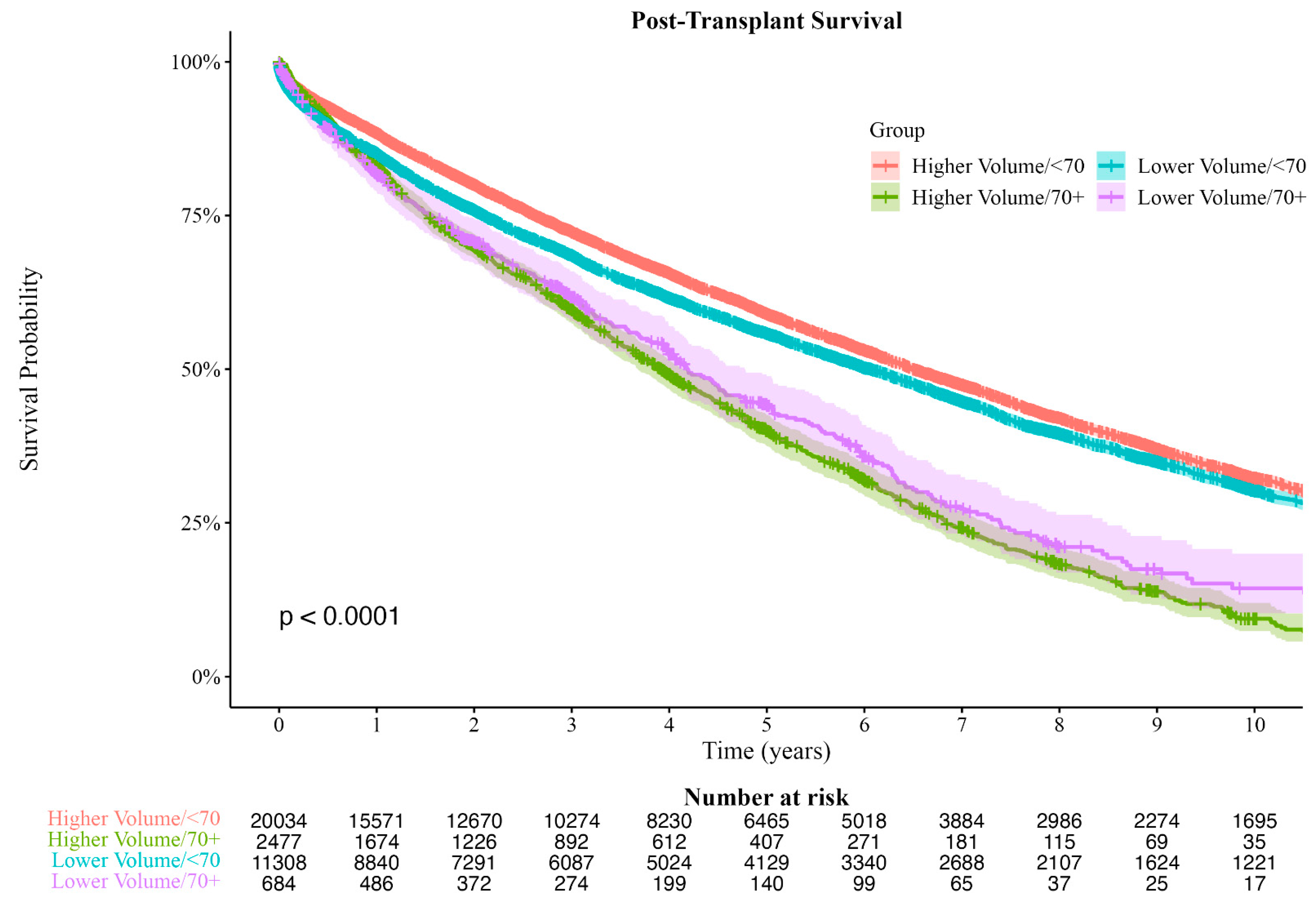
3.6. Post-Transplant Survival Time
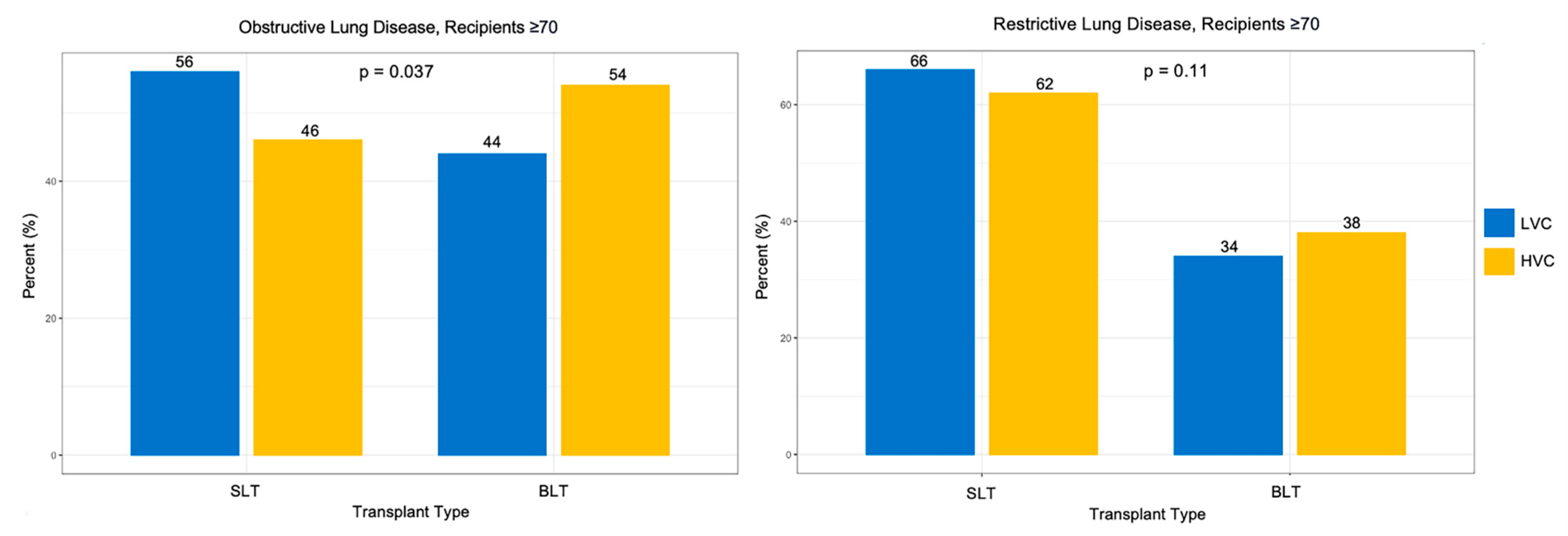
3.7. Center Volume Effects on Recipient Characteristics and Transplant Type in Recipients ≥ 70
3.8. Center Volume Effects over Time
3.9. Multivariate Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Woolf, S.H.; Schoomaker, H. Life Expectancy and Mortality Rates in the United States, 1959–2017. JAMA 2019, 322, 1996–2016. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Valapour, M.; Lehr, C.J.; Skeans, M.A.; Smith, J.M.; Miller, E.; Goff, R.; Mupfudze, T.; Gauntt, K.; Snyder, J.J. OPTN/SRTR 2020 Annual Data Report: Lung. Am. J. Transpl. 2022, 22 (Suppl. S2), 438–518. [Google Scholar] [CrossRef]
- Courtwright, A.; Cantu, E. Lung transplantation in elderly patients. J. Thorac. Dis. 2017, 9, 3346–3351. [Google Scholar] [CrossRef]
- Maurer, J.R.; Frost, A.E.; Estenne, M.; Higenbottam, T.; Glanville, A.R. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. J. Heart Lung Transplant. 1998, 17, 703–709. [Google Scholar] [PubMed]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014—An update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kilic, A.; Merlo, C.A.; Conte, J.V.; Shah, A.S. Lung transplantation in patients 70 years old or older: Have outcomes changed after implementation of the lung allocation score? J. Thorac. Cardiovasc. Surg. 2012, 144, 1133–1138. [Google Scholar] [CrossRef]
- Biswas Roy, S.; Alarcon, D.; Walia, R.; Chapple, K.M.; Bremner, R.M.; Smith, M.A. Is There an Age Limit to Lung Transplantation? Ann. Thorac. Surg. 2015, 100, 443–451. [Google Scholar] [CrossRef]
- Yusen, R.D.; Christie, J.D.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Dipchand, A.I.; Dobbels, F.; Kirk, R.; Lund, L.H.; Rahmel, A.O.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirtieth Adult Lung and Heart-Lung Transplant Report--2013; focus theme: Age. J. Heart Lung Transplant. 2013, 32, 965–978. [Google Scholar] [CrossRef]
- Wigfield, C.H.; Buie, V.; Onsager, D. “Age” in lung transplantation: Factors related to outcomes and other considerations. Curr. Pulmonol. Rep. 2016, 5, 152–158. [Google Scholar] [CrossRef]
- Olson, M.T.; Elnahas, S.; Biswas Roy, S.; Razia, D.; Kang, P.; Bremner, R.M.; Smith, M.A.; Arjuna, A.; Walia, R. Outcomes after lung transplantation in recipients aged 70 years or older. Clin. Transplant. 2022, 36, e14505. [Google Scholar] [CrossRef]
- Thabut, G.; Mal, H. Outcomes after lung transplantation. J. Thorac. Dis. 2017, 9, 2684–2691. [Google Scholar] [CrossRef] [PubMed]
- Bos, S.; Vos, R.; Van Raemdonck, D.E.; Verleden, G.M. Survival in adult lung transplantation: Where are we in 2020? Curr. Opin. Organ Transplant. 2020, 25, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Mooney, J.J.; Weill, D.; Boyd, J.H.; Nicolls, M.R.; Bhattacharya, J.; Dhillon, G.S. Effect of Transplant Center Volume on Cost and Readmissions in Medicare Lung Transplant Recipients. Ann. Am. Thorac. Soc. 2016, 13, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.S.; Allen, J.G.; Meguid, R.A.; Patel, N.D.; Merlo, C.A.; Orens, J.B.; Baumgartner, W.A.; Conte, J.V.; Shah, A.S. The impact of center volume on survival in lung transplantation: An analysis of more than 10,000 cases. Ann. Thorac. Surg. 2009, 88, 1062–1070. [Google Scholar] [CrossRef]
- Hayes, D., Jr.; Sweet, S.C.; Benden, C.; Kopp, B.T.; Goldfarb, S.B.; Visner, G.A.; Mallory, G.B.; Tobias, J.D.; Tumin, D. Transplant center volume and outcomes in lung transplantation for cystic fibrosis. Transpl. Int. 2017, 30, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Subramanian, M.P.; Yan, Y.; Meyers, B.F.; Kozower, B.D.; Patterson, G.A.; Nava, R.G.; Hachem, R.R.; Witt, C.A.; Pasque, M.K.; et al. The Impact of Center Volume on Outcomes in Lung Transplantation. Ann. Thorac. Surg. 2022, 113, 911–917. [Google Scholar] [CrossRef]
- Kilic, A.; George, T.J.; Beaty, C.A.; Merlo, C.A.; Conte, J.V.; Shah, A.S. The effect of center volume on the incidence of postoperative complications and their impact on survival after lung transplantation. J. Thorac. Cardiovasc. Surg. 2012, 144, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage Publications, Inc.: New York, NY, USA, 1991. [Google Scholar]
- Sjoberg, D.D.; Whiting, K.; Curry, M.; Lavery, J.A.; Larmarange, J. Reproducible summary tables with the gtsummary package. R J. 2021, 13, 570–580. [Google Scholar] [CrossRef]
- Hayanga, A.J.; Aboagye, J.K.; Hayanga, H.E.; Morrell, M.; Huffman, L.; Shigemura, N.; Bhama, J.K.; D’Cunha, J.; Bermudez, C.A. Contemporary analysis of early outcomes after lung transplantation in the elderly using a national registry. J. Heart Lung Transplant. 2015, 34, 182–188. [Google Scholar] [CrossRef]
- Somers, J.; Ruttens, D.; Verleden, S.E.; Cox, B.; Stanzi, A.; Vandermeulen, E.; Vos, R.; Vanaudenaerde, B.M.; Verleden, G.M.; Van Veer, H.; et al. A decade of extended-criteria lung donors in a single center: Was it justified? Transpl. Int. 2015, 28, 170–179. [Google Scholar] [CrossRef]
- Christie, I.G.; Chan, E.G.; Ryan, J.P.; Harano, T.; Morrell, M.; Luketich, J.D.; Sanchez, P.G. National Trends in Extended Criteria Donor Utilization and Outcomes for Lung Transplantation. Ann. Thorac. Surg. 2021, 111, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Van Raemdonck, D.; Keshavjee, S.; Levvey, B.; Cherikh, W.S.; Snell, G.; Erasmus, M.; Simon, A.; Glanville, A.R.; Clark, S.; D’Ovidio, F.; et al. Donation after circulatory death in lung transplantation-five-year follow-up from ISHLT Registry. J. Heart Lung Transplant. 2019, 38, 1235–1245. [Google Scholar] [CrossRef]
- Thabut, G.; Munson, J.; Haynes, K.; Harhay, M.O.; Christie, J.D.; Halpern, S.D. Geographic disparities in access to lung transplantation before and after implementation of the lung allocation score. Am. J. Transplant. 2012, 12, 3085–3093. [Google Scholar] [CrossRef] [PubMed]
- Puri, V.; Patterson, G.A.; Meyers, B.F. Single versus bilateral lung transplantation: Do guidelines exist? Thorac. Surg. Clin. 2015, 25, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, M.P.; Meyers, B.F. Bilateral versus single lung transplantation: Are two lungs better than one? J. Thorac. Dis. 2018, 10, 4588–4601. [Google Scholar] [CrossRef]
- Thabut, G.; Christie, J.D.; Ravaud, P.; Castier, Y.; Brugiere, O.; Fournier, M.; Mal, H.; Leseche, G.; Porcher, R. Survival after bilateral versus single lung transplantation for patients with chronic obstructive pulmonary disease: A retrospective analysis of registry data. Lancet 2008, 371, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.M.; Davis, R.D.; Simsir, S.A.; Lin, S.S.; Hartwig, M.; Reidy, M.F.; Steele, M.P.; Eu, P.C.; Blumenthal, J.A.; Babyak, M.A. Successful bilateral lung transplant outcomes in recipients 61 years of age and older. Transplantation 2006, 81, 862–865. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Meyer, K.; Tessmann, R.; Meyer, A.; Gohrbandt, B.; Simon, A.; Hagl, C.; Kallenbach, K.; Haverich, A.; Struber, M. Outcome following single vs. bilateral lung transplantation in recipients 60 years of age and older. Transplant. Proc. 2005, 37, 1369–1370. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age of Recipient | |||||
|---|---|---|---|---|---|
| Characteristic | N | Overall, N = 34,957 | <70, N = 31,721 | ≥70, N = 3236 | p-Value † |
| Age (years) | 34,957 | 33 (23–46) | 33 (23–46) | 34 (24–48) | <0.001 |
| Sex (%) | 34,957 | <0.001 | |||
| Female | 13,809 (40) | 12,630 (40) | 1179 (36) | ||
| Male | 21,148 (60) | 19,091 (60) | 2057 (64) | ||
| Creatinine (mg/dL) | 34,784 | 1.00 (0.73–1.40) | 1.00 (0.72–1.40) | 1.00 (0.77–1.55) | <0.001 |
| Pulmonary Infection (%) | 34,957 | 21,051 (60) | 18,865 (59) | 2186 (68) | <0.001 |
| Race (%) | 34,957 | 0.025 | |||
| Black | 6483 (19) | 5862 (18) | 621 (19) | ||
| Hispanic | 5790 (17) | 5203 (16) * | 587 (18) * | ||
| Other | 1344 (3.8) | 1231 (3.9) | 113 (3.5) | ||
| White | 21,340 (61) | 19,425 (61) * | 1915 (59) * | ||
| PO2 (mmHg) | 34,687 | 423 (311–490) | 423 (311–490) | 421 (317–488) | 0.46 |
| PaO2 < 300 (%) | 34,686 | 8338 (24) | 7596 (24) | 742 (23) | 0.18 |
| Diabetes (%) | 34,736 | 2643 (7.6) | 2369 (7.5) | 274 (8.5) | 0.040 |
| Purulent Bronchoscopy (%) | 34,957 | 8002 (23) | 7185 (23) | 817 (25) | <0.001 |
| Abnormal X-ray (%) | 34,648 | 20,580 (59) | 18,411 (59) | 2169 (68) | <0.001 |
| Cause of Death (%) | 34,956 | <0.001 | |||
| Anoxia | 8551 (24) | 7615 (24) * | 936 (29) * | ||
| CNS Tumor | 204 (0.6) | 187 (0.6) | 17 (0.5) | ||
| CVA | 10,673 (31) | 9749 (31) * | 924 (29) * | ||
| Head Trauma | 14,755 (42) | 13,460 (42) * | 1295 (40) * | ||
| Other | 773 (2.2) | 709 (2.2) | 64 (2.0) | ||
| Donor Type (%) | 34,956 | 0.002 | |||
| DBD | 33,643 (96) | 30,561 (96) | 3082 (95) | ||
| DCD | 1313 (3.8) | 1159 (3.7) | 154 (4.8) | ||
| Age of Recipient | |||||
|---|---|---|---|---|---|
| Characteristic | N | Overall, N = 34,957 | <70, N = 31,721 | ≥70, N = 3236 | p-Value † |
| Age at Listing (years) | 34,957 | 60 (51–65) | 59 (50–64) | 71 (70–73) | <0.001 |
| Sex (%) | 34,957 | <0.001 | |||
| Female | 13,986 (40) | 13,174 (42) | 812 (25) | ||
| Male | 20,971 (60) | 18,547 (58) | 2424 (75) | ||
| Race (%) | 34,957 | <0.001 | |||
| Black | 3145 (9.0) | 3049 (9.6) * | 96 (3.0) * | ||
| Hispanic | 2845 (8.1) | 2670 (8.4) * | 175 (5.4) * | ||
| Other | 1011 (2.9) | 907 (2.9) | 104 (3.2) | ||
| White | 27,956 (80) | 25,095 (79) * | 2861 (88) * | ||
| Blood Type (%) | 34,957 | 0.15 | |||
| A | 13,801 (39) | 12,463 (39) | 1338 (41) | ||
| AB | 1360 (3.9) | 1236 (3.9) | 124 (3.8) | ||
| B | 3891 (11) | 3542 (11) | 349 (11) | ||
| O | 15,905 (45) | 14,480 (46) | 1425 (44) | ||
| Diagnosis Group (%) | 34,957 | <0.001 | |||
| Obstructive | 9506 (27) | 8924 (28) * | 582 (18) * | ||
| Pulmonary Hypertension | 1370 (3.9) | 1329 (4.2) * | 41 (1.3) * | ||
| Restrictive | 20,947 (60) | 18,336 (58) * | 2611 (81) * | ||
| Suppurative | 3134 (9.0) | 3132 (9.9) * | 2 (<0.1) * | ||
| Vasodilators (%) | 34,957 | 397 (1.1) | 386 (1.2) | 11 (0.3) | <0.001 |
| Resistant Infection (%) | 33,515 | 953 (2.8) | 933 (3.1) | 20 (0.6) | <0.001 |
| Inotropes (%) | 32,110 | 1477 (4.6) | 1278 (4.4) | 199 (6.4) | <0.001 |
| History of Cigarette Use (%) | 34,403 | 20,049 (58) | 17,872 (57) | 2177 (68) | <0.001 |
| Cardiac Surgery History (%) | 33,629 | 1341 (4.0) | 1108 (3.6) | 233 (7.4) | <0.001 |
| Diabetes (%) | 34,736 | 6859 (20) | 6296 (20) | 563 (18) | <0.001 |
| Body Mass Index (kg/m2) | 34,837 | 25.9 (22.1–29.2) | 25.8 (21.9–29.2) | 26.4 (23.8–29.0) | <0.001 |
| PA Mean Pressure (mmHg) | 32,520 | 25 (20–31) | 25 (20–31) | 23 (19–28) | <0.001 |
| Wedge Pressure (mmHg) | 32,556 | 10.0 (7.0–14.0) | 10.0 (7.0–14.0) | 9.0 (6.0–12.0) | <0.001 |
| Cardiac Output (L/min) | 32,123 | 5.20 (4.40–6.13) | 5.20 (4.40–6.16) | 5.18 (4.43–5.98) | 0.040 |
| O2 Requirement (L/min) | 32,498 | 3.0 (2.0–5.0) | 3.0 (2.0–5.0) | 3.0 (2.0–5.0) | 0.90 |
| Creatinine (mg/dL) | 34,914 | 0.80 (0.70–0.99) | 0.80 (0.70–0.98) | 0.89 (0.75–1.00) | <0.001 |
| Waitlist Time (days) | 34,957 | 52 (15–165) | 55 (16–173) | 33 (11–94) | <0.001 |
| LAS at Listing | 33,885 | 38 (34–46) | 38 (34–46) | 38 (34–45) | 0.46 |
| LAS at Removal | 34,957 | 41 (35–53) | 41 (35–54) | 41 (35–50) | 0.025 |
| Pre-Tx Mechanical Ventilation (%) | 34,303 | 3307 (9.6) | 3174 (10) | 133 (4.2) | <0.001 |
| Transplant Type (%) | 34,957 | <0.001 | |||
| Double | 24,890 (71) | 23,602 (74) | 1288 (40) | ||
| Single | 10,067 (29) | 8119 (26) | 1948 (60) | ||
| Medical Condition at Transplant (%) | 34,593 | <0.001 | |||
| Hospitalized, Non-ICU | 3331 (9.6) | 3051 (9.7) | 280 (8.8) | ||
| ICU | 4306 (12) | 4090 (13) * | 216 (6.8) * | ||
| Not Hospitalized | 26,956 (78) | 24,272 (77) * | 2684 (84) * | ||
| Steroids (%) | 34,070 | 15,527 (46) | 14,305 (46) | 1222 (39) | <0.001 |
| Total Ischemic Time (hours) | 33,986 | 5.22 (4.17–6.35) | 5.25 (4.20–6.38) | 4.82 (3.90–6.03) | <0.001 |
| Center Volume (%) | 34,944 | <0.001 | |||
| High Volume | 22,870 (65) | 20,329 (64) | 2541 (79) | ||
| Lower Volume | 12,074 (35) | 11,380 (36) | 694 (21) | ||
| Age of Recipient | |||||
|---|---|---|---|---|---|
| Outcome | N | Overall, N = 34,957 | <70, N = 31,721 | ≥70, N = 3236 | p-Value † |
| Post-Tx Ventilator Support (%) | 33,743 | <0.001 | |||
| None | 1058 (3.1) | 950 (3.1) | 108 (3.4) | ||
| Ventilator support for ≤48 h | 19,945 (59) | 17,852 (58) * | 2093 (67) * | ||
| Ventilator support for >48 h but <5 days | 5634 (17) | 5174 (17) * | 460 (15) * | ||
| Ventilator support ≥ 5 days | 7106 (21) | 6630 (22) * | 476 (15) * | ||
| Airway Dehiscence (%) | 34,164 | 525 (1.5) | 480 (1.5) | 45 (1.4) | 0.58 |
| Stroke (%) | 34,249 | 811 (2.4) | 733 (2.4) | 78 (2.5) | 0.69 |
| PGD3 at 72 h (%) | 34,957 | 3488 (10.0) | 3140 (9.9) | 348 (11) | 0.12 |
| Dialysis (Post-Tx) (%) | 34,418 | 2531 (7.4) | 2354 (7.5) | 177 (5.6) | <0.001 |
| Length of Stay (days) | 34,021 | 17 (12–29) | 17 (12–29) | 16 (11–27) | <0.001 |
| Treated for Rejection in Year 1 (%) | 27,243 | 6704 (25) | 6223 (25) | 481 (21) | <0.001 |
| Recipient Cause of Death (%) | 16,044 | <0.001 | |||
| Acute Primary Graft Failure | 205 (1.3) | 189 (1.3) | 16 (1.1) | ||
| Cardiovascular | 1212 (7.6) | 1067 (7.3) * | 145 (9.6) * | ||
| Cerebrovascular | 505 (3.1) | 461 (3.2) | 44 (2.9) | ||
| Chronic Primary Graft Failure | 2635 (16) | 2480 (17) * | 155 (10) * | ||
| Hemorrhage | 260 (1.6) | 243 (1.7) | 17 (1.1) | ||
| Infection | 2617 (16) | 2387 (16) | 230 (15) | ||
| Malignancy | 1825 (11) | 1601 (11) * | 224 (15) * | ||
| Multiorgan Failure | 794 (4.9) | 725 (5.0) | 69 (4.6) | ||
| Other | 2909 (18) | 2579 (18) * | 330 (22) * | ||
| Pulmonary | 3082 (19) | 2796 (19) | 286 (19) | ||
| One-Year Survival (%) | 32,316 | 28,146 (87) | 25,789 (87) | 2357 (83) | <0.001 |
| Three-Year Survival (%) | 27,375 | 19,502 (71) | 18,164 (72) | 1338 (62) | <0.001 |
| Characteristic | Overall, N = 3235 | Lower Volume, N = 694 | High Volume, N = 2541 | p-Value † |
|---|---|---|---|---|
| Age at Listing (years) ‡ | 72 (2) | 71 (2) | 72 (2) | <0.001 |
| Race (%) | 0.026 | |||
| Black | 96 (3.0) | 31 (4.5) * | 65 (2.6) * | |
| Hispanic | 175 (5.4) | 40 (5.8) | 135 (5.3) | |
| Other | 104 (3.2) | 16 (2.3) | 88 (3.5) | |
| White | 2860 (88) | 607 (87) | 2253 (89) | |
| Blood Type (%) | 0.31 | |||
| A | 1338 (41) | 303 (44) | 1035 (41) | |
| AB | 124 (3.8) | 20 (2.9) | 104 (4.1) | |
| B | 349 (11) | 71 (10) | 278 (11) | |
| O | 1424 (44) | 300 (43) | 1124 (44) | |
| Diagnosis Group (%) | 0.037 | |||
| Obstructive | 581 (18) | 144 (21) * | 437 (17) * | |
| Pulmonary Hypertension | 41 (1.3) | 12 (1.7) | 29 (1.1) | |
| Restrictive | 2611 (81) | 537 (77) * | 2074 (82) * | |
| Suppurative | 2 (<0.1) | 1 (0.1) | 1 (<0.1) | |
| Sex (%) | 0.14 | |||
| Female | 811 (25) | 189 (27) | 622 (24) | |
| Male | 2424 (75) | 505 (73) | 1919 (76) | |
| Vasodilators (%) | 11 (0.3) | 0 (0) | 11 (0.4) | 0.14 |
| Resistant Infection (%) | 20 (0.6) | 5 (0.7) | 15 (0.6) | 0.78 |
| Inotropes (%) | 199 (6.4) | 17 (2.6) | 182 (7.5) | <0.001 |
| History of Cigarette Use (%) | 2176 (68) | 461 (67) | 1715 (68) | 0.49 |
| Cardiac Surgery History (%) | 233 (7.4) | 42 (6.2) | 191 (7.7) | 0.18 |
| Diabetes (%) | 563 (18) | 140 (20) | 423 (17) | 0.034 |
| Body Mass Index (kg/m2) | 26.4 (23.8–29.0) | 26.2 (23.7–29.2) | 26.4 (23.8–29.0) | 0.77 |
| PA Mean Pressure (mmHg) | 23 (19–28) | 24 (19–28) | 23 (19–28) | 0.18 |
| Wedge Pressure (mmHg) | 9.0 (6.0–12.0) | 10.0 (6.0–13.0) | 9.0 (6.0–12.0) | <0.001 |
| Cardiac Output (L/min) | 5.19 (4.43–5.98) | 5.17 (4.46–6.00) | 5.19 (4.43–5.96) | 0.56 |
| O2 Requirement (L/min) | 3.0 (2.0–5.0) | 3.0 (2.0–5.0) | 3.0 (2.0–5.0) | 0.35 |
| Creatinine (mg/dL) | 0.89 (0.75–1.00) | 0.88 (0.72–1.00) | 0.89 (0.75–1.00) | 0.23 |
| Days on Waitlist (days) | 32 (11–94) | 51 (17–131) | 29 (9–83) | <0.001 |
| LAS at Listing | 38 (34–45) | 38 (34–45) | 38 (34–45) | 0.58 |
| LAS at Removal | 41 (35–50) | 41 (35–51) | 41 (36–50) | 0.60 |
| Pre-Tx Mechanical Ventilation (%) | 133 (4.2) | 41 (6.0) | 92 (3.7) | 0.007 |
| Transplant Type (%) | 0.043 | |||
| Double | 1287 (40) | 253 (36) | 1034 (41) | |
| Single | 1948 (60) | 441 (64) | 1507 (59) | |
| Medical Condition at Transplant (%) | <0.001 | |||
| Hospitalized, Non-ICU | 280 (8.8) | 62 (9.1) | 218 (8.7) | |
| ICU | 216 (6.8) | 70 (10) * | 146 (5.9) * | |
| Not Hospitalized | 2683 (84) | 552 (81) | 2131 (85) | |
| Steroids (%) | 1222 (39) | 318 (47) | 904 (36) | <0.001 |
| Total Ischemic Time (hours) | 4.82 (3.90–6.03) | 4.60 (3.62–5.70) | 4.89 (4.00–6.13) | <0.001 |
| b | SE | HR (95% CI) | ETR (95% CI) | p | |
|---|---|---|---|---|---|
| Recipient Age | |||||
| <70 years | - | - | - | - | - |
| 70+ years | −0.33 | 0.03 | 1.36 (1.28–1.44) | 0.72 (0.67–0.76) | <0.001 |
| Center Volume | |||||
| High Volume | - | - | - | - | - |
| Lower Volume | −0.09 | 0.02 | 1.08 (1.05–1.12) | 0.92 (0.88–0.95) | <0.001 |
| Donor Characteristics | |||||
| Age | 0.00 | 0.00 | 1.00 (1.00–1.01) | 1.00 (0.99–1.00) | <0.001 |
| Sex | |||||
| Female | - | - | - | - | - |
| Male | 0.03 | 0.02 | 0.97 (0.94–1.01) | 1.03 (0.99–1.07) | 0.19 |
| Creatinine | −0.02 | 0.01 | 1.01 (1.00–1.03) | 0.98 (0.97–1.00) | 0.009 |
| Pulmonary Infection | |||||
| No | - | - | - | - | - |
| Yes | 0.02 | 0.02 | 0.99 (0.95–1.02) | 1.02 (0.98–1.06) | 0.42 |
| Race | |||||
| White | - | - | - | - | - |
| Black | −0.17 | 0.02 | 1.17 (1.12–1.22) | 0.84 (0.80–0.88) | <0.001 |
| Hispanic | −0.08 | 0.03 | 1.08 (1.03–1.13) | 0.91 (0.87–0.97) | 0.002 |
| Other | −0.14 | 0.05 | 1.13 (1.04–1.24) | 0.87 (0.79–0.96) | 0.01 |
| PO2 | 0.00 | 0.00 | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 0.62 |
| Diabetes | |||||
| No | - | - | - | - | - |
| Yes | −0.05 | 0.04 | 1.04 (0.98–1.12) | 0.95 (0.89–1.03) | 0.20 |
| Purulent Bronchoscopy | |||||
| No | - | - | - | - | - |
| Yes | −0.01 | 0.02 | 1.01 (0.97–1.05) | 0.99 (0.94–1.03) | 0.54 |
| Abnormal Chest X-Ray | |||||
| No | - | - | - | - | - |
| Yes | 0.03 | 0.02 | 0.97 (0.94–1.01) | 1.03 (0.99–1.07) | 0.15 |
| Donation Type | |||||
| Brain Death (DBD) | - | - | - | - | - |
| Circulatory Death (DCD) | −0.08 | 0.06 | 1.07 (0.96–1.19) | 0.93 (0.83–1.04) | 0.20 |
| Recipient Characteristics | |||||
| Race | |||||
| White | - | - | - | - | - |
| Black | 0.01 | 0.03 | 0.99 (0.93–1.05) | 1.01 (0.94–1.08) | 0.820 |
| Hispanic | 0.12 | 0.04 | 0.89 (0.83–0.96) | 1.13 (1.04–1.22) | 0.002 |
| Other | 0.13 | 0.06 | 0.89 (0.79–0.99) | 1.14 (1.01–1.28) | 0.03 |
| Diagnosis | |||||
| Obstructive | - | - | - | - | - |
| Pulmonary Hypertension | −0.12 | 0.06 | 1.12 (1.01–1.25) | 0.88 (0.79–0.99) | 0.032 |
| Restrictive | 0.05 | 0.03 | 0.95 (0.91–1.00) | 1.05 (1.00–1.11) | 0.06 |
| Suppurative | 0.34 | 0.05 | 0.73 (0.67–0.80) | 1.41 (1.27–1.55) | <0.001 |
| Sex | |||||
| Female | - | - | - | - | - |
| Male | −0.04 | 0.02 | 1.04 (1.00–1.08) | 0.96 (0.92–1.00) | 0.07 |
| Vasodilators | |||||
| No | - | - | - | - | - |
| Yes | 0.12 | 0.11 | 0.90 (0.74–1.09) | 1.12 (0.91–1.38) | 0.27 |
| Resistant Infection | |||||
| No | - | - | - | - | - |
| Yes | −0.12 | 0.07 | 1.11 (0.98–1.26) | 0.89 (0.78–1.02) | 0.09 |
| Inotropes/Vasodilators | |||||
| No | - | - | - | - | - |
| Yes | −0.05 | 0.05 | 1.05 (0.96–1.14) | 0.95 (0.87–1.04) | 0.28 |
| History of Cigarette Use | |||||
| No | - | - | - | - | - |
| Yes | −0.09 | 0.02 | 1.09 (1.04–1.13) | 0.91 (0.87–0.95) | <0.001 |
| Prior Cardiac Surgery | |||||
| No | - | - | - | - | - |
| Yes | −0.22 | 0.04 | 1.22 (1.13–1.32) | 0.81 (0.74–0.88) | <0.001 |
| Diabetes | |||||
| No | - | - | - | - | - |
| Yes | −0.13 | 0.02 | 1.13 (1.08–1.18) | 0.88 (0.84–0.92) | <0.001 |
| Body Mass Index (kg/m2) | 0.00 | 0.00 | 1.00 (1.00–1.01) | 1.00 (0.99–1.00) | 0.34 |
| Mean Pulmonary Artery Pressure | 0.00 | 0.00 | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 0.81 |
| Creatinine | −0.19 | 0.02 | 1.19 (1.15–1.24) | 0.82 (0.79–0.86) | <0.001 |
| Lung Allocation Score at Match | 0.00 | 0.00 | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 0.001 |
| Mechanical Ventilator Support | |||||
| No | - | - | - | - | - |
| Yes | −0.08 | 0.04 | 1.08 (1.00–1.16) | 0.92 (0.85–1.00) | 0.043 |
| Transplant Type | |||||
| Double | - | - | - | - | - |
| Single | −0.37 | 0.02 | 1.40 (1.34–1.46) | 0.69 (0.66–0.73) | <0.001 |
| Medical Condition at Transplant | |||||
| Not Hospitalized | - | - | - | - | - |
| Hospitalized, Non-ICU | −0.09 | 0.04 | 1.09 (1.02–1.17) | 0.91 (0.85–0.98) | 0.012 |
| ICU | −0.17 | 0.05 | 1.17 (1.08–1.27) | 0.84 (0.77–0.92) | <0.001 |
| Steroids | |||||
| No | - | - | - | - | - |
| Yes | −0.08 | 0.02 | 1.07 (1.04–1.11) | 0.93 (0.89–0.96) | <0.001 |
| Ischemic Time (Hours) | −0.03 | 0.01 | 1.02 (1.01–1.03) | 0.97 (0.96–0.98) | <0.001 |
| Model Intercept | 8.86 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyanna, N.; Chan, E.G.; Ryan, J.P.; Furukawa, M.; Coster, J.N.; Hage, C.A.; Sanchez, P.G. Lung Transplantation Outcomes in Recipients Aged 70 Years or Older and the Impact of Center Volume. J. Clin. Med. 2023, 12, 5372. https://doi.org/10.3390/jcm12165372
Iyanna N, Chan EG, Ryan JP, Furukawa M, Coster JN, Hage CA, Sanchez PG. Lung Transplantation Outcomes in Recipients Aged 70 Years or Older and the Impact of Center Volume. Journal of Clinical Medicine. 2023; 12(16):5372. https://doi.org/10.3390/jcm12165372
Chicago/Turabian StyleIyanna, Nidhi, Ernest G. Chan, John P. Ryan, Masashi Furukawa, Jenalee N. Coster, Chadi A. Hage, and Pablo G. Sanchez. 2023. "Lung Transplantation Outcomes in Recipients Aged 70 Years or Older and the Impact of Center Volume" Journal of Clinical Medicine 12, no. 16: 5372. https://doi.org/10.3390/jcm12165372