
A Deep-Learning Approach to Spleen Volume Estimation in Patients with Gaucher Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. MRI Imaging
2.2. Reference Labeling and Dataset
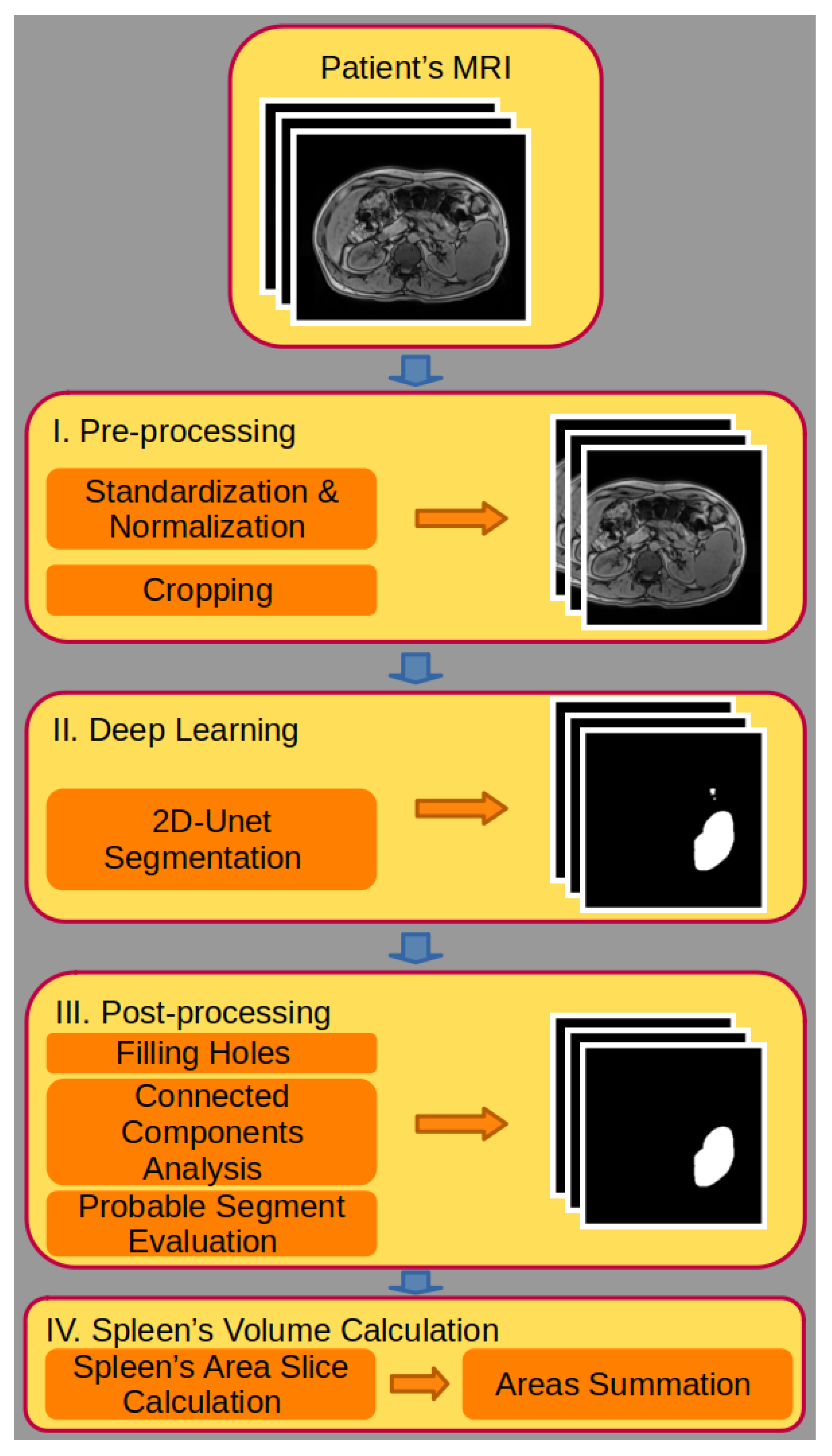
2.3. Pre-Processing
2.4. Deep-Learning Modeling for Automated Segmentation
2.5. Testing Dataset
2.6. Post-Processing
2.7. Spleen Volume Calculation
2.8. Full-Scan Spleen Volume Calculation
2.9. Dice Coefficient
2.10. Software
3. Results
3.1. Modeling Pipeline
3.2. Model Accuracy
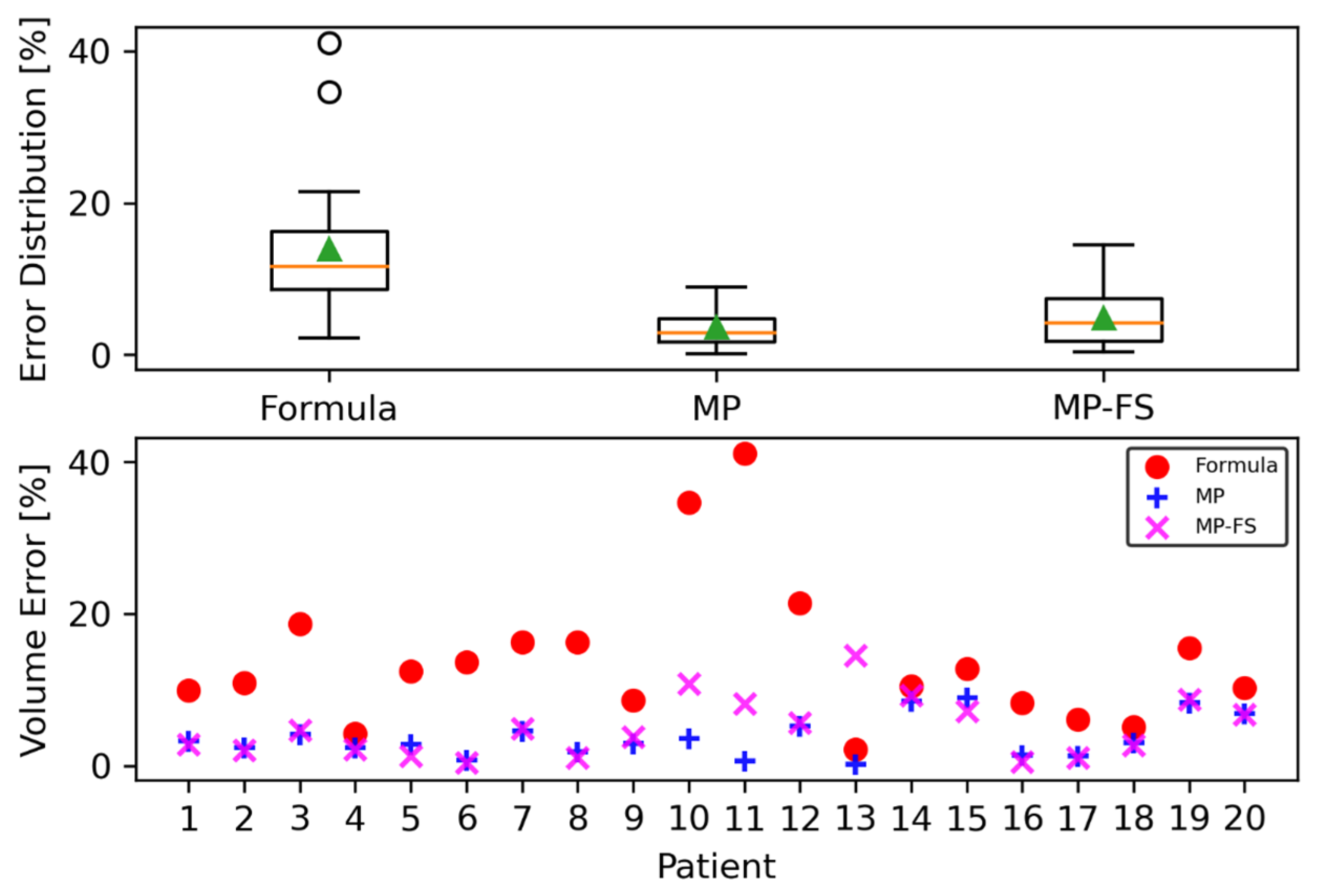
3.3. Spleen Volume Calculation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Revel-Vilk, S.; Szer, J.; Zimran, A. Gaucher disease and related lysosomal storage diseases. In Williams Hematology, 10th ed.; Kaushansky, K., Lichtman, M., Prchal, J., Levi, M., Burns, L., Eds.; McGraw-Hill: New York, NY, USA, 2021; pp. 1189–1202. [Google Scholar]
- Bennett, L.L.; Mohan, D. Gaucher disease and its treatment options. Ann. Pharmacother. 2013, 47, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.; Belmatoug, N.; Camou, F.; Serratrice, C.; Froissart, R.; Caillaud, C.; Levade, T.; Astudillo, L.; Serratrice, J.; Brassier, A.; et al. A Review of Gaucher Disease Pathophysiology, Clinical Presentation and Treatments. Int. J. Mol. Sci. 2017, 18, 441. [Google Scholar] [CrossRef] [PubMed]
- Nalysnyk, L.; Rotella, P.; Simeone, J.C.; Hamed, A.; Weinreb, N. Gaucher disease epidemiology and natural history: A comprehensive review of the literature. Hematology 2017, 22, 65–73. [Google Scholar] [CrossRef]
- Revel-Vilk, S.; Szer, J.; Mehta, A.; Zimran, A. How we manage Gaucher Disease in the era of choices. Br. J. Haematol. 2018, 182, 467–480. [Google Scholar] [CrossRef]
- Guggenbuhl, P.; Grosbois, B.; Chalès, G. Gaucher disease. Jt. Bone Spine 2008, 75, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Futerman, A.H.; Sussman, J.L.; Horowitz, M.; Silman, I.; Zimran, A. New directions in the treatment of Gaucher disease. Trends Pharmacol. Sci. 2004, 25, 147–151. [Google Scholar] [CrossRef]
- Nagral, A. Gaucher disease. J. Clin. Exp. Hepatol. 2014, 4, 37–50. [Google Scholar] [CrossRef]
- Revel-Vilk, S.; Szer, J.; Zimran, A. Hematological manifestations and complications of Gaucher disease. Expert. Rev. Hematol. 2021, 14, 347–354. [Google Scholar] [CrossRef]
- Robertson, F.; Leander, P.; Ekberg, O. Radiology of the spleen. Eur. Radiol. 2001, 11, 80–95. [Google Scholar] [CrossRef]
- Linguraru, M.G.; Sandberg, J.K.; Jones, E.C.; Summers, R.M. Assessing splenomegaly: Automated volumetric analysis of the spleen. Acad. Radiol. 2013, 20, 675–684. [Google Scholar] [CrossRef]
- Prassopoulos, P.; Daskalogiannaki, M.; Raissaki, M.; Hatjidakis, A.; Gourtsoyiannis, N. Determination of normal splenic volume on computed tomography in relation to age, gender and body habitus. Eur. Radiol. 1997, 7, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, A.S.; D’Ippolito, G.; Faintuch, S.; Szejnfeld, J.; Ahmed, M. Determination of splenomegaly by CT: Is there a place for a single measurement? AJR Am. J. Roentgenol. 2005, 184, 1510–1513. [Google Scholar] [CrossRef] [PubMed]
- Nuffer, Z.; Marini, T.; Rupasov, A.; Kwak, S.; Bhatt, S. The Best Single Measurement for Assessing Splenomegaly in Patients with Cirrhotic Liver Morphology. Acad. Radiol. 2017, 24, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Humpire-Mamani, G.E.; Bukala, J.; Scholten, E.T.; Prokop, M.; van Ginneken, B.; Jacobs, C. Fully automatic volume measurement of the spleen at CT using deep learning. Radiol. Artif. Intell. 2020, 2, e190102. [Google Scholar] [CrossRef]
- Moon, H.; Huo, Y.; Abramson, R.G.; Peters, R.A.; Assad, A.; Moyo, T.K.; Savona, M.R.; Landman, B.A. Acceleration of spleen segmentation with end-to-end deep learning method and automated pipeline. Comput. Biol. Med. 2019, 107, 109–117. [Google Scholar] [CrossRef]
- Sharbatdaran, A.; Romano, D.; Teichman, K.; Dev, H.; Raza, S.I.; Goel, A.; Moghadam, M.C.; Blumenfeld, J.D.; Chevalier, J.M.; Shimonov, D.; et al. Deep Learning Automation of Kidney, Liver, and Spleen Segmentation for Organ Volume Measurements in Autosomal Dominant Polycystic Kidney Disease. Tomography 2022, 8, 1804–1819. [Google Scholar] [CrossRef]
- Altini, N.; Prencipe, B.; Cascarano, G.D.; Brunetti, A.; Brunetti, G.; Triggiani, V.; Carnimeo, L.; Marino, F.; Guerriero, A.; Villani, L.; et al. Liver, kidney and spleen segmentation from CT scans and MRI with deep learning: A survey. Neurocomputing 2022, 490, 30–53. [Google Scholar] [CrossRef]
- Bengio, Y.; Goodfellow, I.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Ma, J.; Zhang, Y.; Gu, S.; Zhu, C.; Ge, C.; Zhang, Y.; An, X.; Wang, C.; Wang, Q.; Liu, X.; et al. AbdomenCT-1K: Is Abdominal Organ Segmentation A Solved Problem? IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 6695–6712. [Google Scholar] [CrossRef]
- Zhou, S.K.; Greenspan, H.; Davatzikos, C.; Duncan, J.S.; van Ginneken, B.; Madabhushi, A.; Prince, J.L.; Rueckert, D.; Summers, R.M. A review of deep learning in medical imaging: Image traits, technology trends, case studies with progress highlights, and future promises. Proc. IEEE 2021, 109, 820–838. [Google Scholar] [CrossRef]
- Conze, P.H.; Kavur, A.E.; Cornec-Le Gall, E.; Sinem Gezer, N.; Le Meur, Y.; Alper Selver, M.; Rousseau, F. Abdominal multi-organ segmentation with cascaded convolutional and adversarial deep networks. Artif. Intell. Med. 2021, 117, 102109. [Google Scholar] [CrossRef]
- Tang, Y.; Gao, R.; Lee, H.H.; Han, S.; Chen, Y.; Gao, D.; Nath, V.; Bermudez, C.; Savona, M.R.; Abramson, R.G.; et al. High-resolution 3D abdominal segmentation with random patch network fusion. Med. Image Anal. 2021, 69, 101894. [Google Scholar] [CrossRef]
- Hatamizadeh, A.; Tang, Y.; Nath, V.; Yang, D.; Myronenko, A.; Landman, B.; Roth, H.; Xu, D. UNETR: Transformers for 3D Medical Image Segmentation. In Proceedings of the 2022 IEEE/CVF Winter Conference on Applications of Computer Vision (WACV), Waikoloa, HI, USA, 3–8 January 2022; pp. 1748–1758. [Google Scholar] [CrossRef]
- Yang, Y.; Tang, Y.; Gao, R.; Bao, S.; Huo, Y.; McKenna, M.T.; Savona, M.R.; Abramson, R.G.; Landman, B.A. Validation and estimation of spleen volume via computer-assisted segmentation on clinically acquired CT scans. J. Med. Imaging 2021, 8, 014004. [Google Scholar] [CrossRef]
- Bobo, M.F.; Bao, S.; Huo, Y.; Yao, Y.; Virostko, J.; Plassard, A.J.; Lyu, I.; Assad, A.; Abramson, R.G.; Hilmes, M.A.; et al. Fully Convolutional Neural Networks Improve Abdominal Organ Segmentation. Proc. SPIE Int. Soc. Opt. Eng. 2018, 105742, 750–757. [Google Scholar] [CrossRef]
- Huo, Y.; Xu, Z.; Bao, S.; Bermudez, C.; Plassard, A.J.; Liu, J.; Yao, Y.; Assad, A.; Abramson, R.G.; Landman, B.A. Splenomegaly Segmentation using Global Convolutional Kernels and Conditional Generative Adversarial Networks. Proc. SPIE Int. Soc. Opt. Eng. 2018, 10574, 1057409. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Huo, Y.; Xiong, Y.; Moon, H.; Assad, A.; Moyo, T.K.; Savona, M.R.; Abramson, R.; Landman, B.A. Improving Splenomegaly Segmentation by Learning from Heterogeneous Multi-Source Labels. Proc. SPIE Int. Soc. Opt. Eng. 2019, 10949, 1094908. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Yoon, J.S.; Lee, S.S.; Suk, H.I.; Son, J.H.; Sung, Y.S.; Lee, Y.; Kang, B.K.; Kim, H.S. Deep Learning Algorithm for Automated Segmentation and Volume Measurement of the Liver and Spleen Using Portal Venous Phase Computed Tomography Images. Korean J. Radiol. 2020, 21, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Huo, Y.; Xu, Z.; Bao, S.; Bermudez, C.; Moon, H.; Parvathaneni, P.; Moyo, T.K.; Savona, M.R.; Assad, A.; Abramson, R.G.; et al. Splenomegaly Segmentation on Multi-Modal MRI Using Deep Convolutional Networks. IEEE Trans. Med. Imaging 2019, 38, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Liu, S.; Xu, S.; Dong, C.; Li, Z.; Shi Javen, Q.; Zhang, Y.; Dai, D. 3D Medical image segmentation using parallel transformers. Pattern Recognit. 2023, 138, 109432. [Google Scholar] [CrossRef]
- Meddeb, A.; Kossen, T.; Bressem, K.K.; Molinski, N.; Hamm, B.; Nagel, S.N. Two-Stage Deep Learning Model for Automated Segmentation and Classification of Splenomegaly. Cancers 2022, 14, 5476. [Google Scholar] [CrossRef]
- Chen, Y.; Ruan, D.; Xiao, J.; Wang, L.; Sun, B.; Saouaf, R.; Yang, W.; Li, D.; Fan, Z. Fully automated multiorgan segmentation in abdominal magnetic resonance imaging with deep neural networks. Med. Phys. 2020, 47, 4971–4982. [Google Scholar] [CrossRef]
- Valindria, V.V.; Pawlowski, N.; Rajchl, M.; Lavdas, I.; Aboagye, E.O.; Rockall, A.G.; Rueckert, D.; Glocker, B. Multi-modal Learning from Unpaired Images: Application to Multi-organ Segmentation in CT and MRI. In Proceedings of the IEEE Winter Conference on Applications of Computer Vision (WACV) 2018, Lake Tahoe, NV, USA, 12–15 March 2018; pp. 547–556. [Google Scholar] [CrossRef]
- Müller, L.; Kloeckner, R.; Mähringer-Kunz, A.; Stoehr, F.; Düber, C.; Arnhold, G.; Gairing, S.J.; Foerster, F.; Weinmann, A.; Galle, P.R.; et al. Fully automated AI-based splenic segmentation for predicting survival and estimating the risk of hepatic decompensation in TACE patients with HCC. Eur. Radiol. 2022, 32, 6302–6313. [Google Scholar] [CrossRef] [PubMed]
- Rickmann, A.M.; Senapati, J.; Kovalenko, O.; Peters, A.; Bamberg, F.; Wachinger, C. AbdomenNet: Deep neural network for abdominal organ segmentation in epidemiologic imaging studies. BMC Med. Imaging 2022, 22, 168. [Google Scholar] [CrossRef] [PubMed]
- Meddeb, A.; Kossen, T.; Bressem, K.K.; Hamm, B.; Nagel, S.N. Evaluation of a Deep Learning Algorithm for Automated Spleen Segmentation in Patients with Conditions Directly or Indirectly Affecting the Spleen. Tomography 2021, 7, 950–960. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Yoon, J.S.; Lee, S.S.; Suk, H.I.; Park, B.; Sung, Y.S.; Hong, S.B.; Ryu, H. Deep Learning-Based Assessment of Functional Liver Capacity Using Gadoxetic Acid-Enhanced Hepatobiliary Phase MRI. Korean J. Radiol. 2022, 23, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Lenchik, L.; Heacock, L.; Weaver, A.A.; Boutin, R.D.; Cook, T.S.; Itri, J.; Filippi, C.G.; Gullapalli, R.P.; Lee, J.; Zagurovskaya, M.; et al. Automated Segmentation of Tissues Using CT and MRI: A Systematic Review. Acad. Radiol. 2019, 26, 1695–1706. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv 2015, arXiv:1505.04597. [Google Scholar]
- Segmentation Models. Available online: https://segmentation-modelspytorch.readthedocs.io/en/latest/ (accessed on 8 July 2023).
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. arXiv 2019, arXiv:1912.01703. [Google Scholar]
- Van Rossum, G.; Drake, F.L., Jr. Python Reference Manual; Centrum voor Wiskunde en Informatica Amsterdam: Amsterdam, The Netherlands, 1995. [Google Scholar]
- Home–OpenCV. Available online: https://opencv.org (accessed on 8 July 2023).
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0 Contributors. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- van der Walt, S.; Schönberger, J.L.; Nunez-Iglesias, J.; Boulogne, F.; Warner, J.D.; Yager, N.; Gouillart, E.; Yu, T. and the scikit-image contributors. scikit-image: Image processing in Python. PeerJ 2014, 2, e453. [Google Scholar] [CrossRef]
- Umesh, P. Image Processing in Python. CSI Commun. 2012, 23, 1–48. [Google Scholar]
- Celluloid. Available online: https://github.com/jwkvam/celluloid (accessed on 8 July 2023).
- Mason, D. SU-E-T-33: Pydicom: An open source DICOM library. Med. Phys. 2011, 38, 3493. [Google Scholar] [CrossRef]
- Masoudi, S.; Harmon, S.A.; Mehralivand, S.; Walker, S.M.; Raviprakash, H.; Bagci, U.; Choyke, P.L.; Turkbey, B. Quick guide on radiology image pre-processing for deep learning applications in prostate cancer research. J. Med. Imaging 2021, 8, 010901. [Google Scholar] [CrossRef] [PubMed]
- Furtado, P. Improving Deep Segmentation of Abdominal Organs MRI by Post-Processing. BioMedInformatics 2021, 1, 88–105. [Google Scholar] [CrossRef]
- Simon, G.; Erdos, M.; Maródi, L.; Tóth, J. Gaucher-kór: A korai diagnózis és terápia jelentôsége [Gaucher disease: Importance of early diagnosis and therapy]. Orv. Hetil. 2008, 149, 743–750. (In Hungarian) [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DC [%] | |
|---|---|
| Mean | 94.1 |
| Standard deviation | 1.9 |
| Range | 89.6–96.8 |
| Formula [%] | Model Prediction [%] | Model Prediction—Full Scan [%] | |
|---|---|---|---|
| Mean | 13.9 | 3.6 | 4.9 |
| Standard deviation | 9.6 | 2.7 | 3.9 |
| Range | 2.2–41.2 | 0.12–8.91 | 0.39–14.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azuri, I.; Wattad, A.; Peri-Hanania, K.; Kashti, T.; Rosen, R.; Caspi, Y.; Istaiti, M.; Wattad, M.; Applbaum, Y.; Zimran, A.; et al. A Deep-Learning Approach to Spleen Volume Estimation in Patients with Gaucher Disease. J. Clin. Med. 2023, 12, 5361. https://doi.org/10.3390/jcm12165361
Azuri I, Wattad A, Peri-Hanania K, Kashti T, Rosen R, Caspi Y, Istaiti M, Wattad M, Applbaum Y, Zimran A, et al. A Deep-Learning Approach to Spleen Volume Estimation in Patients with Gaucher Disease. Journal of Clinical Medicine. 2023; 12(16):5361. https://doi.org/10.3390/jcm12165361
Chicago/Turabian StyleAzuri, Ido, Ameer Wattad, Keren Peri-Hanania, Tamar Kashti, Ronnie Rosen, Yaron Caspi, Majdolen Istaiti, Makram Wattad, Yaakov Applbaum, Ari Zimran, and et al. 2023. "A Deep-Learning Approach to Spleen Volume Estimation in Patients with Gaucher Disease" Journal of Clinical Medicine 12, no. 16: 5361. https://doi.org/10.3390/jcm12165361