
The Impact of a Twelve-Week Moderate Aerobic Exercise Program on Gastrointestinal Symptom Profile and Psychological Well-Being of Irritable Bowel Syndrome Patients: Preliminary Data from a Southern Italy Cohort

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
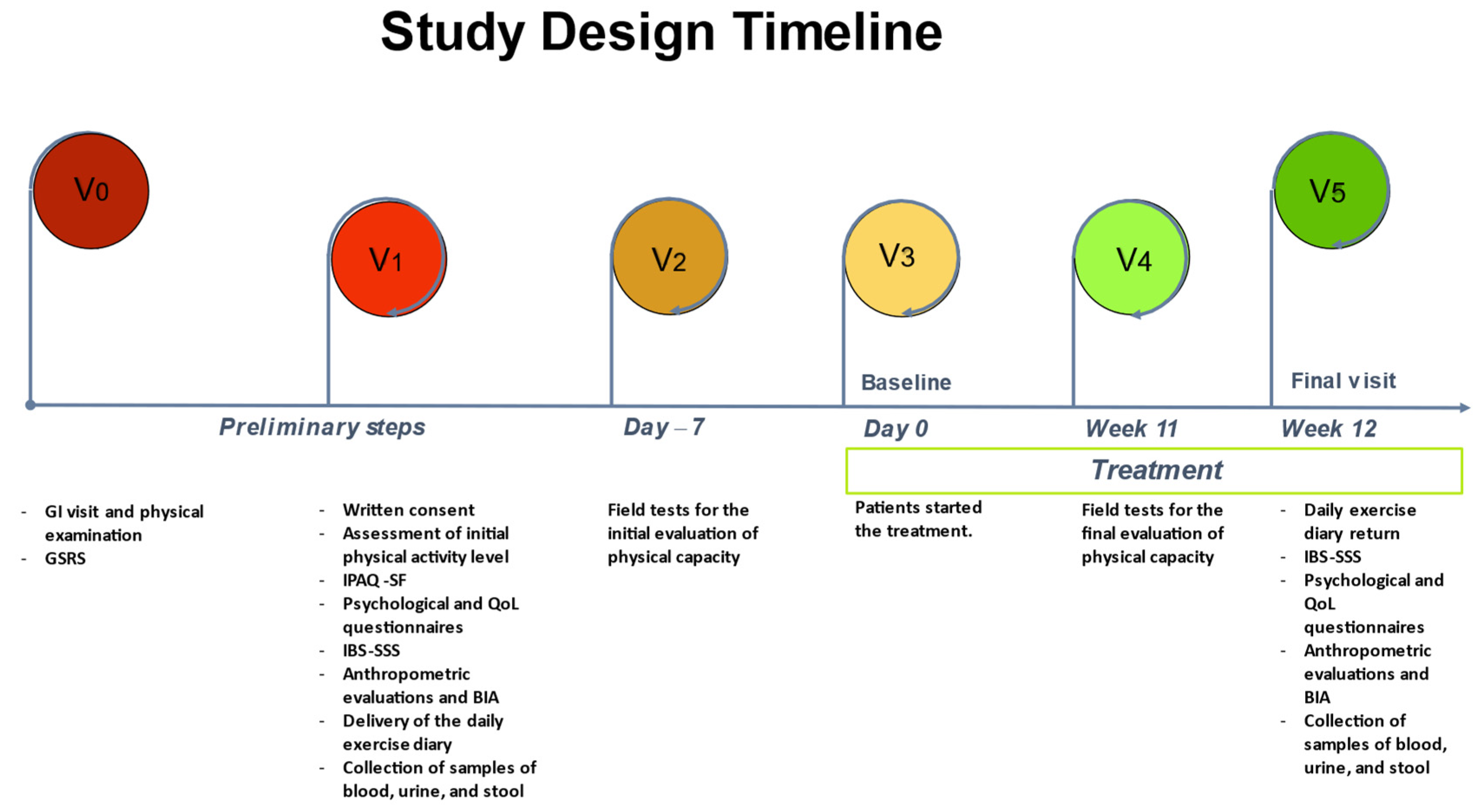
2.2. Study Design
2.3. Anthropometric and Bioelectrical Impedance Analysis (BIA) Parameters
2.4. Gastrointestinal Questionnaires
2.4.1. Irritable Bowel Syndrome Severity Scoring System (IBS-SSS)
2.5. Psychological Questionnaires
2.5.1. Irritable Bowel Syndrome Quality of Life Questionnaire (IBS-QoL)
2.5.2. Thirty-Six-Item Short-Form Health Survey (SF-36)
2.5.3. Symptom Checklist-90-Revised (SCL-90-R)
2.5.4. Psychophysiological Questionnaire (QPF/R)
2.6. Evaluation of Physical Capacity
2.6.1. Field Tests
2.6.2. Characteristics of the Exercise Program
- Frequency: walking exercise was carried out outdoors on an urban route three times a week on non-consecutive days for 12 weeks.
- Intensity: the intensity of the exercise was 60–75% of HRmax; it was monitored using a heart-rate monitor and customized using Tanaka’s formula [30]. In addition, a talk test (a standardized and validated survey instrument based on the exercise subject’s ability to hold a conversation) was used to measure pace [31] and a modified Borg scale was used to measure the perception of fatigue (on a scale of 0–10, a perception of 5–6 was required) [32].
- Type: the type of exercise was moderate aerobic, with speeds ranging from 5 to 10 km/h.
- Time: A single outing, lasting 60′, was structured as follows: warm-up, 5′; normal walk, 10′; sustained walking, 30′; fast walking, 10′; cool-down, 5′.
- Volume: participants in the project performed 180 min per week of moderate-intensity aerobic exercise, following indications from the American College of Sports Medicine (ACSM) guidance on preventive health [33]. However, participants could also increase their exercise volume through activities outside the project. All exercise data within and outside the project were recorded in the daily diary to evaluate energy expenditure.
2.7. Statistical Analysis
3. Results
3.1. Patients’ Demographic, Anthropometric, and Bioelectrical Impedance Characteristics
3.2. Gastrointestinal (GI) Symptoms
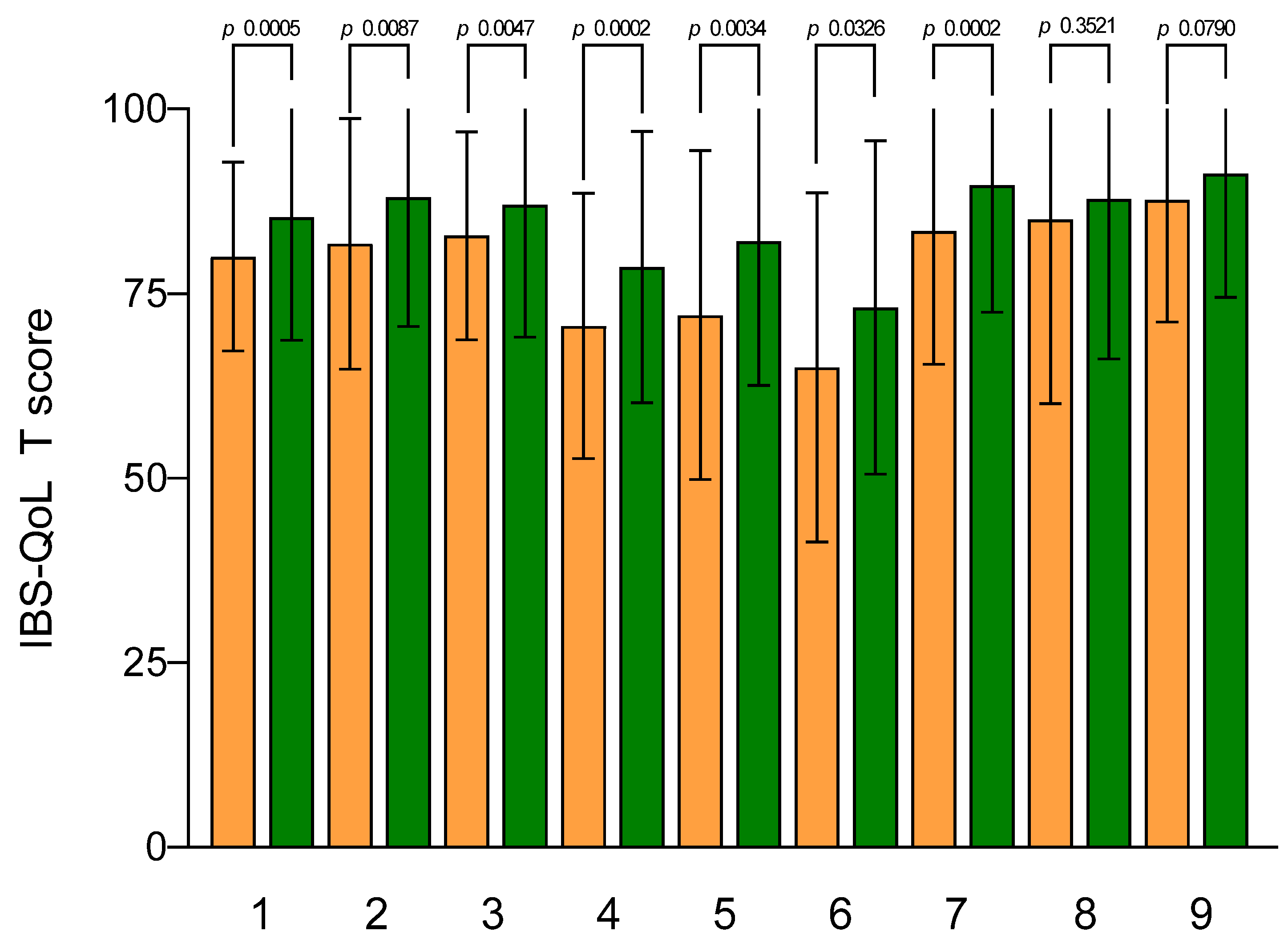
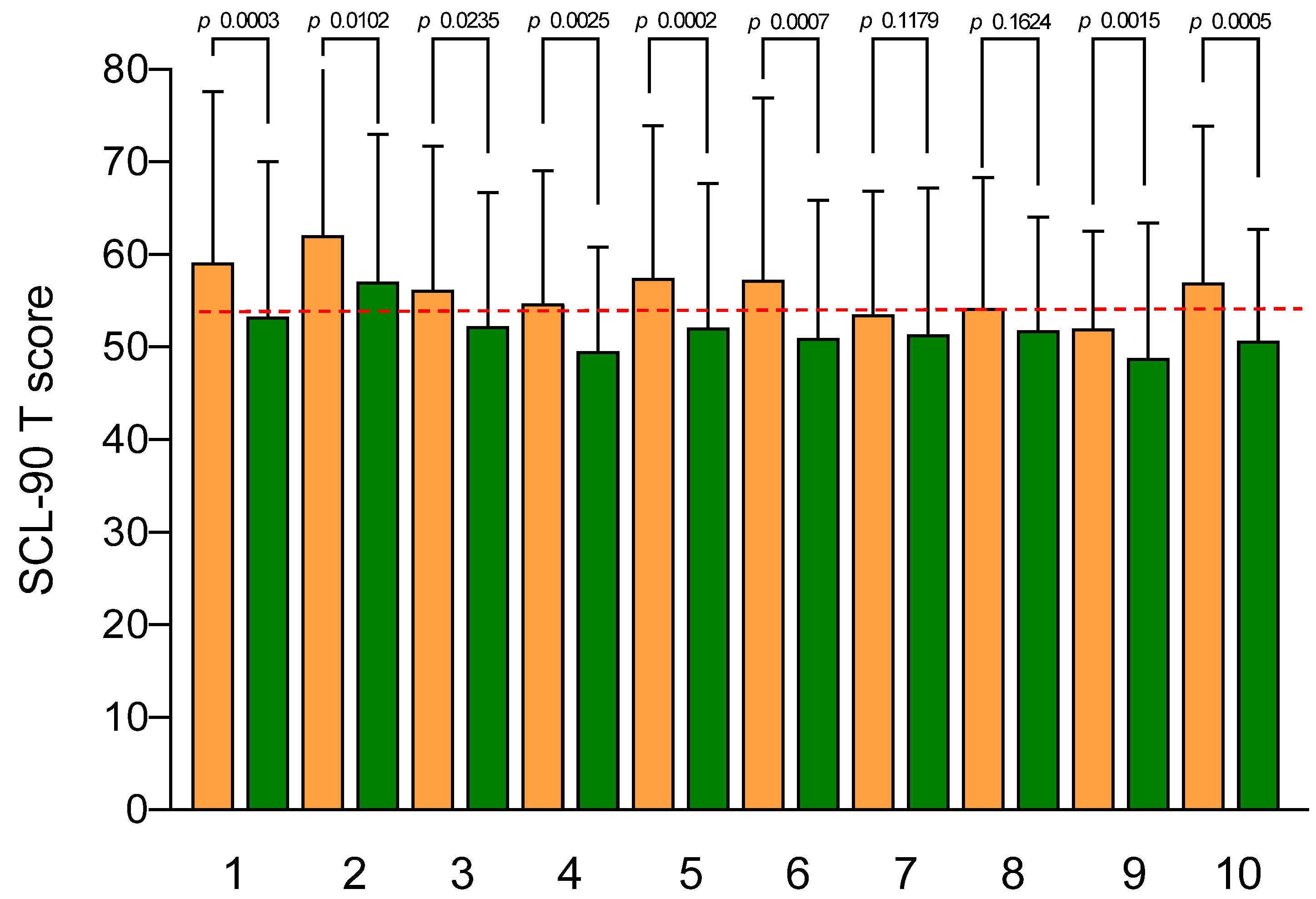
3.3. Psychological and Quality of Life Profiles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drossman, D.A. The functional gastrointestinal disorders and the Rome III process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Yadav, Y.S.; Eslick, G.D.; Talley, N.J. Review article: Irritable bowel syndrome: Natural history, bowel habit stability and overlap with other gastrointestinal disorders. Aliment. Pharmacol. Ther. 2021, 54 (Suppl. S1), S24–S32. [Google Scholar] [CrossRef] [PubMed]
- Adriani, A.; Ribaldone, D.G.; Astegiano, M.; Durazzo, M.; Saracco, G.M.; Pellicano, R. Irritable bowel syndrome: The clinical approach. Panminerva Med. 2018, 60, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Omagari, K.; Murayama, T.; Tanaka, Y.; Yoshikawa, C.; Inoue, S.; Ichimura, M.; Hatanaka, M.; Saimei, M.; Muto, K.; Tobina, T.; et al. Mental, physical, dietary, and nutritional effects on irritable bowel syndrome in young Japanese women. Intern. Med. 2013, 52, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Nee, J.; Lembo, A. Review Article: Current and future treatment approaches for IBS with diarrhoea (IBS-D) and IBS mixed pattern (IBS-M). Aliment. Pharmacol. Ther. 2021, 54 (Suppl. S1), S63–S74. [Google Scholar] [CrossRef]
- Black, C.J.; Staudacher, H.M.; Ford, A.C. Efficacy of a low FODMAP diet in irritable bowel syndrome: Systematic review and network meta-analysis. Gut 2022, 71, 1117–1126. [Google Scholar] [CrossRef]
- Russo, F.; Riezzo, G.; Orlando, A.; Linsalata, M.; D’Attoma, B.; Prospero, L.; Ignazzi, A.; Giannelli, G. A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial. Nutrients 2022, 14, 1544. [Google Scholar] [CrossRef]
- Prospero, L.; Riezzo, G.; Linsalata, M.; Orlando, A.; D’Attoma, B.; Russo, F. Psychological and Gastrointestinal Symptoms of Patients with Irritable Bowel Syndrome Undergoing a Low-FODMAP Diet: The Role of the Intestinal Barrier. Nutrients 2021, 13, 2469. [Google Scholar] [CrossRef]
- Orlando, A.; Tutino, V.; Notarnicola, M.; Riezzo, G.; Linsalata, M.; Clemente, C.; Prospero, L.; Martulli, M.; D’Attoma, B.; De Nunzio, V.; et al. Improved Symptom Profiles and Minimal Inflammation in IBS-D Patients Undergoing a Long-Term Low-FODMAP Diet: A Lipidomic Perspective. Nutrients 2020, 12, 1652. [Google Scholar] [CrossRef]
- Russo, F.; Riezzo, G.; Linsalata, M.; Orlando, A.; Tutino, V.; Prospero, L.; D’Attoma, B.; Giannelli, G. Managing Symptom Profile of IBS-D Patients With Tritordeum-Based Foods: Results From a Pilot Study. Front. Nutr. 2022, 9, 797192. [Google Scholar] [CrossRef]
- Berry, S.K.; Chey, W.D. Integrated Care for Irritable Bowel Syndrome: The Future Is Now. Gastroenterol. Clin. 2021, 50, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Dainese, R.; Serra, J.; Azpiroz, F.; Malagelada, J.R. Effects of physical activity on intestinal gas transit and evacuation in healthy subjects. Am. J. Med. 2004, 116, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo-Alventosa, R.; Ingles, M.; Cortes-Amador, S.; Gimeno-Mallench, L.; Chirivella-Garrido, J.; Kropotov, J.; Serra-Ano, P. Low-Intensity Physical Exercise Improves Pain Catastrophizing and Other Psychological and Physical Aspects in Women with Fibromyalgia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3634. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Raglin, J.S. Exercise and mental health. Beneficial and detrimental effects. Sports Med. 1990, 9, 323–329. [Google Scholar] [CrossRef]
- Gao, X.; Tian, S.; Huang, N.; Sun, G.; Huang, T. Associations of daily sedentary behavior, physical activity, and sleep with irritable bowel syndrome: A prospective analysis of 362,193 participants. J. Sport Health Sci. 2023. epub ahead of print. [Google Scholar] [CrossRef]
- Costantino, A.; Pessarelli, T.; Vecchiato, M.; Vecchi, M.; Basilisco, G.; Ermolao, A. A practical guide to the proper prescription of physical activity in patients with irritable bowel syndrome. Dig. Liver Dis. 2022, 54, 1600–1604. [Google Scholar] [CrossRef]
- Johannesson, E.; Simren, M.; Strid, H.; Bajor, A.; Sadik, R. Physical activity improves symptoms in irritable bowel syndrome: A randomized controlled trial. Am. J. Gastroenterol. 2011, 106, 915–922. [Google Scholar] [CrossRef]
- Bianco, A.; Franco, I.; Osella, A.R.; Giannelli, G.; Riezzo, G.; Bonfiglio, C.; Prospero, L.; Sorino, P.; Russo, F. Physical Activity Reduction and the Worsening of Gastrointestinal Health Status during the Second COVID-19 Home Confinement in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 9554. [Google Scholar] [CrossRef] [PubMed]
- Kulich, K.R.; Madisch, A.; Pacini, F.; Pique, J.M.; Regula, J.; Van Rensburg, C.J.; Ujszaszy, L.; Carlsson, J.; Halling, K.; Wiklund, I.K. Reliability and validity of the Gastrointestinal Symptom Rating Scale (GSRS) and Quality of Life in Reflux and Dyspepsia (QOLRAD) questionnaire in dyspepsia: A six-country study. Health Qual Life Outcomes 2008, 6, 12. [Google Scholar] [CrossRef]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Andrae, D.A.; Patrick, D.L.; Drossman, D.A.; Covington, P.S. Evaluation of the Irritable Bowel Syndrome Quality of Life (IBS-QOL) questionnaire in diarrheal-predominant irritable bowel syndrome patients. Health Qual. Life Outcomes 2013, 11, 208. [Google Scholar] [CrossRef]
- Barile, J.P.; Horner-Johnson, W.; Krahn, G.; Zack, M.; Miranda, D.; DeMichele, K.; Ford, D.; Thompson, W.W. Measurement characteristics for two health-related quality of life measures in older adults: The SF-36 and the CDC Healthy Days items. Disabil. Health J. 2016, 9, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Jensen, H.H.; Mortensen, E.L.; Lotz, M. Scl-90-R symptom profiles and outcome of short-term psychodynamic group therapy. Int. Sch. Res. Not. 2013, 2013, 540134. [Google Scholar] [CrossRef] [PubMed]
- Bertolotti, G.; Michielin, P.; Vidotto, G.; Sanavio, E.; Bottesi, G.; Bettinardi, O.; Zotti, A.M. Metric qualities of the cognitive behavioral assessment for outcome evaluation to estimate psychological treatment effects. Neuropsychiatr. Dis. Treat. 2015, 11, 2449–2460. [Google Scholar] [CrossRef]
- Hanson, S.; Jones, A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 710–715. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Foster, C.; Porcari, J.P.; Anderson, J.; Paulson, M.; Smaczny, D.; Webber, H.; Doberstein, S.T.; Udermann, B. The talk test as a marker of exercise training intensity. J. Cardiopulm. Rehabil. Prev. 2008, 28, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.C.; Jones, P.W. A comparison of the visual analogue scale and modified Borg scale for the measurement of dyspnoea during exercise. Clin. Sci. 1989, 76, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Baggish, A.L.; Franklin, B.; Jaworski, C.; Riebe, D. American College of Sports Medicine Expert Consensus Statement to Update Recommendations for Screening, Staffing, and Emergency Policies to Prevent Cardiovascular Events at Health Fitness Facilities. Curr. Sports Med. Rep. 2020, 19, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Berthoud, H.R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H.; et al. Neurobiology of exercise. Obesity 2006, 14, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Johannesson, E.; Jakobsson Ung, E.; Sadik, R.; Ringstrom, G. Experiences of the effects of physical activity in persons with irritable bowel syndrome (IBS): A qualitative content analysis. Scand. J. Gastroenterol. 2018, 53, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Shahabi, L.; Naliboff, B.D.; Shapiro, D. Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: A pilot study. Psychol. Health Med. 2016, 21, 176–188. [Google Scholar] [CrossRef]
- Nunan, D.; Cai, T.; Gardener, A.D.; Ordonez-Mena, J.M.; Roberts, N.W.; Thomas, E.T.; Mahtani, K.R. Physical activity for treatment of irritable bowel syndrome. Cochrane Database Syst. Rev. 2022, 6, CD011497. [Google Scholar] [CrossRef]
- Williams, P.T.; Thompson, P.D. Walking versus running for hypertension, cholesterol, and diabetes mellitus risk reduction. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1085–1091. [Google Scholar] [CrossRef]
- Hong, H.R.; Jeong, J.O.; Kong, J.Y.; Lee, S.H.; Yang, S.H.; Ha, C.D.; Kang, H.S. Effect of walking exercise on abdominal fat, insulin resistance and serum cytokines in obese women. J. Exerc. Nutr. Biochem. 2014, 18, 277–285. [Google Scholar] [CrossRef]
- Fani, M.; Mostamand, J.; Fani, M.; Chitsaz, N.; Feizi, A. The effect of aerobic exercises among women with mild and moderate irritable bowel syndrome: A pilot study. J. Bodyw. Mov. Ther. 2019, 23, 161–165. [Google Scholar] [CrossRef]
- Hajizadeh Maleki, B.; Tartibian, B.; Mooren, F.C.; FitzGerald, L.Z.; Kruger, K.; Chehrazi, M.; Malandish, A. Low-to-moderate intensity aerobic exercise training modulates irritable bowel syndrome through antioxidative and inflammatory mechanisms in women: Results of a randomized controlled trial. Cytokine 2018, 102, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Johannesson, E.; Jakobsson Ung, E.; Ringstrom, G.; Sadik, R. The experiences of physical activity in irritable bowel syndrome-A qualitative study. J. Clin. Nurs. 2019, 28, 3189–3199. [Google Scholar] [CrossRef] [PubMed]
- Groenendijk, D.W.; Witteman, B.J.; Mulder, B.C. The Experiences of Female IBS Patients Concerning Physical Activity as Treatment Modality: A Qualitative Study. Qual. Health Res. 2022, 32, 1690–1700. [Google Scholar] [CrossRef] [PubMed]
- Riezzo, G.; Prospero, L.; Orlando, A.; Linsalata, M.; D’Attoma, B.; Ignazzi, A.; Giannelli, G.; Russo, F. A Tritordeum-Based Diet for Female Patients with Diarrhea-Predominant Irritable Bowel Syndrome: Effects on Abdominal Bloating and Psychological Symptoms. Nutrients 2023, 15, 1361. [Google Scholar] [CrossRef]
- Franklin, B.A.; Rusia, A.; Haskin-Popp, C.; Tawney, A. Chronic Stress, Exercise and Cardiovascular Disease: Placing the Benefits and Risks of Physical Activity into Perspective. Int. J. Environ. Res. Public Health 2021, 18, 9922. [Google Scholar] [CrossRef]
- Kandola, A.; Stubbs, B. Exercise and Anxiety. Adv. Exp. Med. Biol. 2020, 1228, 345–352. [Google Scholar]
- Saeed, S.A.; Cunningham, K.; Bloch, R.M. Depression and Anxiety Disorders: Benefits of Exercise, Yoga, and Meditation. Am. Fam. Physician 2019, 99, 620–627. [Google Scholar]
- Abdin, S.; Welch, R.K.; Byron-Daniel, J.; Meyrick, J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: A systematic review. Public Health 2018, 160, 70–76. [Google Scholar] [CrossRef]
- Elsenbruch, S.; Enck, P. Placebo effects and their determinants in gastrointestinal disorders. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 472–485. [Google Scholar] [CrossRef]
- Aragón-Vela, J.; Solis-Urra, P.; Ruiz-Ojeda, F.J.; Álvarez-Mercado, A.I.; Olivares-Arancibia, J.; Plaza-Diaz, J. Impact of Exercise on Gut Microbiota in Obesity. Nutrients 2021, 13, 3999. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre | Post | p-Value | |
|---|---|---|---|
| Height (m) | 164.2 ± 1.50 | // | // |
| Weight (kg) | 78.5 ± 2.49 | 77.9 ± 2.57 | 0.0847 |
| BMI (kg/m2) | 29.0 ± 0.81 | 28.8 ± 0.81 | 0.0580 |
| Mid-upper arm circumference (cm) | 33.6 ± 0.60 | 32.9 ± 0.61 | 0.0002 |
| Waist circumference (cm) | 93.0 ± 2.12 | 92.8 ± 2.16 | 0.2204 |
| Hip circumference (cm) | 106.3 ± 1.59 | 105.6 ± 1.58 | 0.0474 |
| PhA (degrees) | 6.4 ± 0.17 | 6.4 ± 0.15 | 0.9284 |
| BCM (kg) | 29.1 ± 1.11 | 28.9 ± 1.06 | 0.6538 |
| FM (kg) | 27.4 ± 1.70 | 27 ± 1.72 | 0.2200 |
| FFM (kg) | 52.0 ± 1.48 | 51.5 ± 1.43 | 0.1206 |
| TBW (liters) | 37.8 ± 1.08 | 37.7 ± 1.04 | 0.1976 |
| ECW (liters) | 16.6 ± 0.43 | 16.5 ± 0.41 | 0.6436 |
| Item | Pre | Post | % Reduction | p-Value |
|---|---|---|---|---|
| Severity of abdominal pain | 24.5 ± 4.31 | 12.6 ± 3.46 | 48.6% | 0.0001 |
| Frequency of abdominal pain | 21.7 ± 4.72 | 8.6 ± 2.87 | 60.4% | 0.0003 |
| Severity of abdominal bloating | 45.7 ± 3.79 | 27.8 ± 3.38 | 39.2% | 0.0001 |
| Dissatisfaction with bowel habit | 47.7 ± 5.09 | 31.2 ± 3.78 | 34.6% | 0.0002 |
| Interference with life in general | 43.4 ± 4.06 | 31.5 ± 4.30 | 27.4% | 0.0077 |
| Total score | 183.1 ± 12.56 | 111.8 ± 12.15 | 38.9% | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riezzo, G.; Prospero, L.; D’Attoma, B.; Ignazzi, A.; Bianco, A.; Franco, I.; Curci, R.; Campanella, A.; Bonfiglio, C.; Osella, A.R.; et al. The Impact of a Twelve-Week Moderate Aerobic Exercise Program on Gastrointestinal Symptom Profile and Psychological Well-Being of Irritable Bowel Syndrome Patients: Preliminary Data from a Southern Italy Cohort. J. Clin. Med. 2023, 12, 5359. https://doi.org/10.3390/jcm12165359
Riezzo G, Prospero L, D’Attoma B, Ignazzi A, Bianco A, Franco I, Curci R, Campanella A, Bonfiglio C, Osella AR, et al. The Impact of a Twelve-Week Moderate Aerobic Exercise Program on Gastrointestinal Symptom Profile and Psychological Well-Being of Irritable Bowel Syndrome Patients: Preliminary Data from a Southern Italy Cohort. Journal of Clinical Medicine. 2023; 12(16):5359. https://doi.org/10.3390/jcm12165359
Chicago/Turabian StyleRiezzo, Giuseppe, Laura Prospero, Benedetta D’Attoma, Antonia Ignazzi, Antonella Bianco, Isabella Franco, Ritanna Curci, Angelo Campanella, Caterina Bonfiglio, Alberto Ruben Osella, and et al. 2023. "The Impact of a Twelve-Week Moderate Aerobic Exercise Program on Gastrointestinal Symptom Profile and Psychological Well-Being of Irritable Bowel Syndrome Patients: Preliminary Data from a Southern Italy Cohort" Journal of Clinical Medicine 12, no. 16: 5359. https://doi.org/10.3390/jcm12165359