
Clinical and Therapeutic Implications of Male Obesity

Abstract
:1. Introduction
2. The Psychological Aspect of Obesity and the Influence of Cortisol
3. Male Obesity Overview
4. Pathogenetic Factors of Obesity
5. Clinical Consequences of Male Obesity
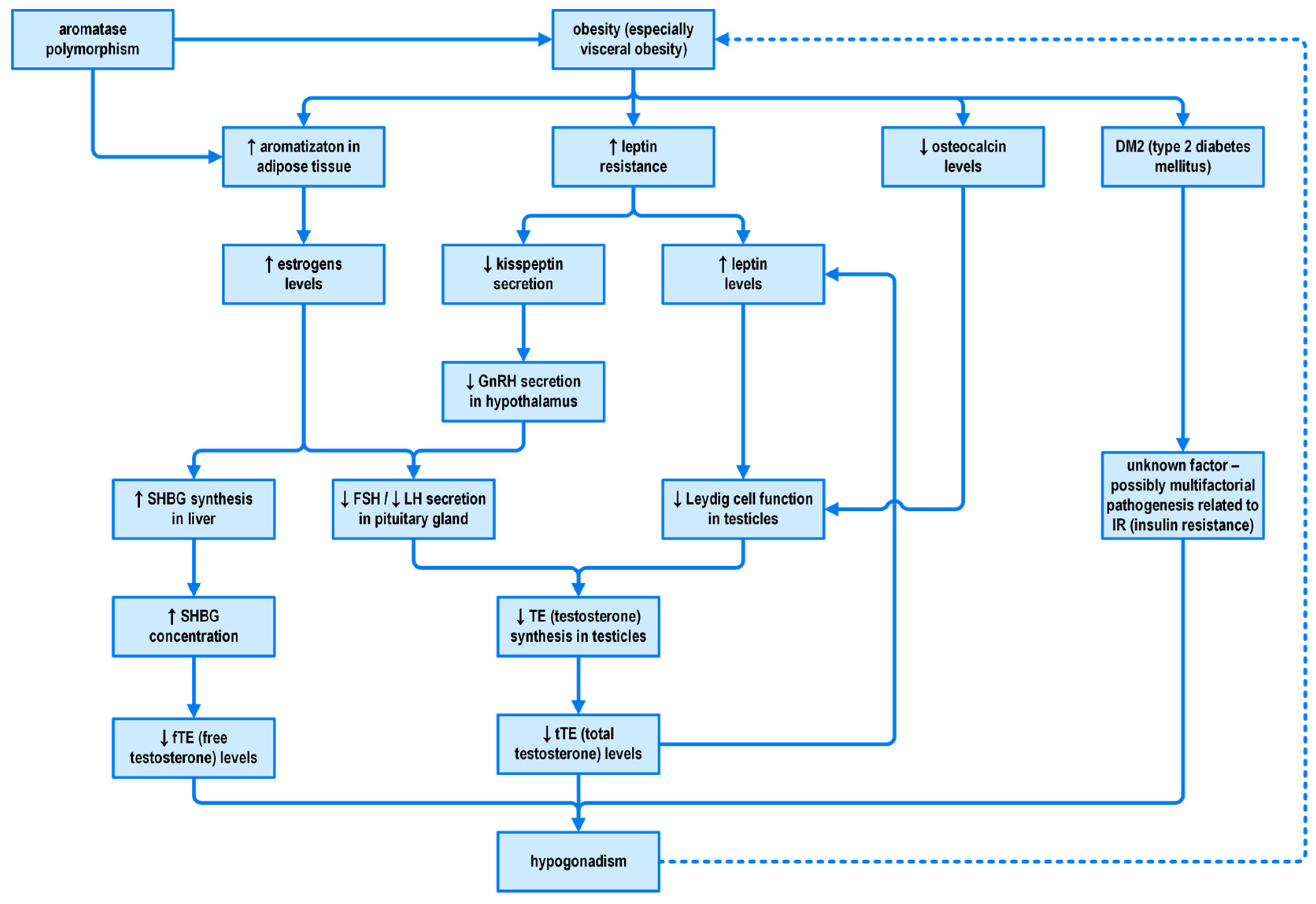
5.1. Obesity, Hypogonadism and Infertility in Men with Obesity
5.2. Diabetes Mellitus and Cardiovascular Disorders
5.3. Cancer
5.4. Metabolic Associated Fatty Liver Disease (MAFLD)
6. Obesity Treatment
6.1. Diet and Lifestyle Interventions
6.2. Pharmacotherapy of Obesity
6.3. Bariatric Surgery
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed]
- WHO. Noncommunicable Diseases: Risk Factors. World Health Organization. 2021. p. 1. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/ncd-risk-factors (accessed on 8 May 2023).
- World Obesity Federation. World Obesity Atlas 2023. Available online: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2023 (accessed on 27 July 2023).
- Lovejoy, J.C.; Sainsbury, A.; Stock Conference 2008 Working Group. Sex differences in obesity and the regulation of energy homeostasis. Obes. Rev. 2009, 10, 154–167. [Google Scholar] [CrossRef]
- Fuchs, H.F.; Broderick, R.C.; Harnsberger, C.R.; Chang, D.C.; Sandler, B.J.; Jacobsen, G.R.; Horgan, S. Benefits of bariatric surgery do not reach obese men. J. Laparoendosc. Adv. Surg. Tech. A 2015, 25, 196–201. [Google Scholar] [CrossRef]
- Kroll, D.S.; Feldman, D.E.; Biesecker, C.L.; McPherson, K.L.; Manza, P.; Joseph, P.V.; Volkow, N.D.; Wang, G.-J. Neuroimaging of Sex/Gender Differences in Obesity: A Review of Structure, Function, and Neurotransmission. Nutrients 2020, 12, 1942. [Google Scholar] [CrossRef]
- Chao, A.M.; Loughead, J.; Bakizada, Z.M.; Hopkins, C.M.; Geliebter, A.; Gur, R.C.; Wadden, T.A. Sex/gender differences in neural correlates of food stimuli: A systematic review of functional neuroimaging studies. Obes. Rev. 2017, 18, 687–699. [Google Scholar] [CrossRef]
- Dekkers, I.A.; Jansen, P.R.; Lamb, H.J. Obesity, Brain Volume, and White Matter Microstructure at MRI: A Cross-sectional UK Biobank Study. Radiology 2019, 291, 763–771. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Dallman, M.F.; Epel, E.S. Comfort food is comforting to those most stressed: Evidence of the chronic stress response network in high stress women. Psychoneuroendocrinology 2011, 36, 1513–1519. [Google Scholar] [CrossRef]
- Frayn, M.; Livshits, S.; Knäuper, B. Emotional eating and weight regulation: A qualitative study of compensatory behaviors and concerns. J. Eat. Disord. 2018, 6, 23. [Google Scholar] [CrossRef]
- Dallman, M.F.; Pecoraro, N.C.; La Fleur, S.E.; Warne, J.P.; Ginsberg, A.B.; Akana, S.F.; Laugero, K.C.; Houshyar, H.; Strack, A.M.; Bhatnagar, S.; et al. Chapter 4: Glucocorticoids, chronic stress, and obesity. Prog. Brain Res. 2006, 153, 75–105. [Google Scholar]
- Puhl, R.M.; Peterson, J.L.; Luedicke, J. Weight-Based Victimization: Bullying Experiences of Weight Loss Treatment–Seeking Youth. Pediatrics 2013, 131, e1–e9. [Google Scholar] [CrossRef]
- Romeo, R.D. Pubertal maturation and programming of hypothalamic-pituitary-adrenal reactivity. Front. Neuroendocr. 2010, 31, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.P.; McKlveen, J.M.; Ghosal, S.; Kopp, B.; Wulsin, A.; Makinson, R.; Scheimann, J.; Myersr, B. Regulation of the hypothalamic-pituitary-adrenocortical stress response. Compr. Physiol. 2016, 6, 603–621. [Google Scholar] [PubMed]
- Coderre, L.; Srivastava, A.K.; Chiasson, J.L. Role of glucocorticoid in the regulation of glycogen metabolism in skeletal muscle. Am. J. Physiol.-Endocrinol. Metab. 1991, 260, E927–E932. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Balland, E.; Cowley, M.A. Hypothalamic Insulin Resistance in Obesity: Effects on Glucose Homeostasis. Neuroendocrinology 2017, 104, 364–381. Available online: https://www.karger.com/Article/FullText/455865 (accessed on 6 January 2022). [CrossRef]
- Toufexis, D.; Rivarola, M.A.; Lara, H.; Viau, V. Stress and the Reproductive Axis. J. Neuroendocr. 2014, 26, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Adam, T.C.; Epel, E.S. Stress, eating and the reward system. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef]
- Hackett, R.A.; Steptoe, A. Type 2 diabetes mellitus and psychological stress—A modifiable risk factor. Nat. Rev. Endocrinol. 2017, 13, 547–560. [Google Scholar] [CrossRef]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. BMJ 2006, 332, 521–525. Available online: https://www.bmj.com/content/332/7540/521 (accessed on 6 January 2022). [CrossRef]
- Tryon, M.S.; Carter, C.S.; DeCant, R.; Laugero, K.D. Chronic stress exposure may affect the brain’s response to high calorie food cues and predispose to obesogenic eating habits. Physiol. Behav. 2013, 120, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics 2014, 33, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Himmelstein, M.S. Weight Bias Internalization Among Adolescents Seeking Weight Loss: Implications for Eating Behaviors and Parental Communication. Front. Psychol. 2018, 9, 2271. [Google Scholar] [CrossRef] [PubMed]
- Copeland, W.E.; Bulik, C.M.; Zucker, N.; Wolke, D.; Lereya, S.T.; Costello, E.J. Does childhood bullying predict eating disorder symptoms? A prospective, longitudinal analysis. Int. J. Eat. Disord. 2015, 48, 1141–1149. [Google Scholar] [CrossRef]
- Holder, M.K.; Blaustein, J.D. Puberty and adolescence as a time of vulnerability to stressors that alter neurobehavioral processes. Front. Neuroendocr. 2013, 35, 89–110. [Google Scholar] [CrossRef]
- Uliaszek, A.A.; Zinbarg, R.E.; Mineka, S.; Craske, M.G.; Sutton, J.M.; Griffith, J.W.; Rose, R.; Waters, A.; Hammen, C. The role of neuroticism and extraversion in the stress-anxiety and stress-depression relationships. Anxiety Stress. Coping 2010, 23, 363–381. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Rosselli, F.; Perrin, N.; DeBar, L.; Wilson, G.T.; May, A.; Kraemer, H.C. Gender difference in the prevalence of eating disorder symptoms. Int. J. Eat. Disord. 2009, 42, 471–474. [Google Scholar] [CrossRef]
- Culbert, K.M.; Shope, M.M.; Sisk, C.L.; Klump, K.L. Low testosterone is associated with dysregulated eating symptoms in young adult men. Int. J. Eat. Disord. 2020, 53, 1469–1479. [Google Scholar] [CrossRef]
- Gray, C.M.; Anderson, A.S.; Clarke, A.M.; Dalziel, A.; Hunt, K.; Leishman, J.; Wyke, S.; Poolsup, N.; Suksomboon, N.; Jiamsathit, W.; et al. Addressing male obesity: An evaluation of a group-based weight management intervention for Scottish men. J. Men’s Health 2009, 6, 70–81. [Google Scholar] [CrossRef]
- Gough, B.; Conner, M.T. Barriers to healthy eating amongst men: A qualitative analysis. Soc. Sci. Med. 2006, 62, 387–395. [Google Scholar] [CrossRef]
- Palmer, B.F.; Clegg, D.J. The sexual dimorphism of obesity. Mol. Cell. Endocrinol. 2015, 402, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Ley, C.J.; Lees, B.; Stevenson, J.C. Sex- and menopause-associated changes in body-fat distribution. Am. J. Clin. Nutr. 1992, 55, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Min, K.-B.; Min, J.-Y. Android and gynoid fat percentages and serum lipid levels in United States adults. Clin. Endocrinol. 2015, 82, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Llorens, S.; Pourbagher-Shahri, A.M.; Ashrafizadeh, M.; Talebi, M.; Shakibaei, M.; Samarghandian, S. An Overview of the Role of Adipokines in Cardiometabolic Diseases. Molecules 2020, 25, 5218. [Google Scholar] [CrossRef]
- Plaisance, E.P.; Grandjean, P.W.; Judd, R.L.; Jones, K.W.; Taylor, J.K. The influence of sex, body composition, and nonesterified fatty acids on serum adipokine concentrations. Metabolism 2009, 58, 1557–1563. [Google Scholar] [CrossRef]
- Rosenbaum, M.; Pietrobelli, A.; Vasselli, J.; Heymsfield, S.; Leibel, R. Sexual dimorphism in circulating leptin concentrations is not accounted for by differences in adipose tissue distribution. Int. J. Obes. 2001, 25, 1365–1371. [Google Scholar] [CrossRef]
- Kawano, J.; Arora, R. The Role of Adiponectin in Obesity, Diabetes, and Cardiovascular Disease. J. CardioMetabolic Syndr. 2009, 4, 44–49. [Google Scholar] [CrossRef]
- Cnop, M.; Havel, P.J.; Utzschneider, K.M.; Carr, D.B.; Sinha, M.K.; Boyko, E.J.; Retzlaff, B.M.; Knopp, R.H.; Brunzell, J.D.; Kahn, S.E. Relationship of adiponectin to body fat distribution, insulin sensitivity and plasma lipoproteins: Evidence for independent roles of age and sex. Diabetologia 2003, 46, 459–469. Available online: https://link.springer.com/article/10.1007/s00125-003-1074-z (accessed on 6 January 2022). [CrossRef]
- Alissa, E.M.; Alzughaibi, L.S.; Marzouki, Z.M. Association between serum resistin, adiposity measures and inflammatory makers in women without cardiovascular diseases. Chem. Phys. Lipids. 2019, 218, 136–140. [Google Scholar] [CrossRef]
- Kern, P.A.; Ranganathan, S.; Li, C.; Wood, L.; Ranganathan, G.; Aparicio-Siegmund, S.; Garbers, Y.; Flynn, C.M.; Waetzig, G.H.; Gouni-Berthold, I.; et al. Adipose tissue tumor necrosis factor and interleukin-6 expression in human obesity and insulin resistance. Am. J. Physiol.-Endocrinol. Metab. 2001, 280, E745–E751. [Google Scholar] [CrossRef]
- Himmerich, H.; Fulda, S.; Linseisen, J.; Seiler, H.; Wolfram, G.; Himmerich, S.; Gedrich, K.; Pollmächer, T. TNF-alpha, soluble TNF receptor and interleukin-6 plasma levels in the general population. Eur. Cytokine Netw. 2006, 17, 196–201. [Google Scholar] [PubMed]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef]
- Chen, K.-H.E.; Lainez, N.M.; Coss, D. Sex Differences in Macrophage Responses to Obesity-Mediated Changes Determine Migratory and Inflammatory Traits. J. Immunol. 2020, 206, 141–153. [Google Scholar] [CrossRef]
- Tung, Y.L.; Yeo, G.S.; O’rahilly, S.; Coll, A.P. Obesity and FTO: Changing Focus at a Complex Locus. Cell Metab. 2014, 20, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Vaisse, C.; Clement, K.; Guy-Grand, B.; Froguel, P. A frameshift mutation in human MC4R is associated with a dominant form of obesity. Nat. Genet. 1998, 20, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Yeo, G.S.; Farooqi, I.S.; Aminian, S.; Halsall, D.J.; Stanhope, R.G.; O’Rahilly, S. A frameshift mutation in MC4R associated with dominantly inherited human obesity. Nat. Genet. 1998, 20, 111–112. [Google Scholar] [CrossRef]
- Collet, T.H.; Dubern, B.; Mokrosinski, J.; Connors, H.; Keogh, J.M.; de Oliveira, E.M.; Henning, E.; Poitou-Bernert, C.; Oppert, J.-M.; Tounian, P.; et al. Evaluation of a melanocortin-4 receptor (MC4R) agonist (Setmelanotide) in MC4R deficiency. Mol. Metab. 2017, 6, 1321–1329. [Google Scholar] [CrossRef]
- Farooqi, I.S.; Matarese, G.; Lord, G.M.; Keogh, J.M.; Lawrence, E.; Agwu, C.; Sanna, V.; Jebb, S.A.; Perna, F.; Fontana, S.; et al. Beneficial effects of leptin on obesity, T cell hyporesponsiveness, and neuroendocrine/metabolic dysfunction of human congenital leptin deficiency. J. Clin. Investig. 2002, 110, 1093–1103. [Google Scholar] [CrossRef]
- Farooqi, I.S.; O’Rahilly, S. Human disorders of leptin action. J. Endocrinol. 2014, 223, T63–T70. [Google Scholar] [CrossRef]
- Tacer, K.F.; Potts, P.R. Cellular and disease functions of the prader-willi syndrome gene magel2. Biochem. J. 2017, 474, 2177–2190. [Google Scholar] [CrossRef]
- Kershaw, E.E.; Flier, J.S. Adipose Tissue as an Endocrine Organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.S.; Hoermann, R.; Dupuis, P.; Joon, D.L.; Zajac, J.D.; Grossmann, M. Relationships between insulin resistance and frailty with body composition and testosterone in men undergoing androgen deprivation therapy for prostate cancer. Eur. J. Endocrinol. 2016, 175, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Pellitero, S.; Olaizola, I.; Alastrue, A.; Martínez, E.; Granada, M.L.; Balibrea, J.M.; Moreno, P.; Serra, A.; Navarro-Díaz, M.; Romero, R.; et al. Hypogonadotropic Hypogonadism in Morbidly Obese Males Is Reversed After Bariatric Surgery. Obes. Surg. 2012, 22, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ding, Z. Obesity, a serious etiologic factor for male subfertility in modern society. Reproduction 2017, 154, R123–R131. [Google Scholar] [CrossRef] [PubMed]
- Calderón, B.; Gómez-Martín, J.M.; Vega-Piñero, B.; Martín-Hidalgo, A.; Galindo, J.; Luque-Ramírez, M.; Escobar-Morreale, H.F.; Botella-Carretero, J.I. Prevalence of male secondary hypogonadism in moderate to severe obesity and its relationship with insulin resistance and excess body weight. Andrology 2016, 4, 62–67. [Google Scholar] [CrossRef]
- Schneider, G.; Kirschner, M.A.; Berkowitz, R.; Ertel, N.H. Increased Estrogen Production in Obese Men. J. Clin. Endocrinol. Metab. 1979, 48, 633–638. [Google Scholar] [CrossRef]
- Barakat, R.; Oakley, O.; Kim, H.; Jin, J.; Ko, C.J. Extra-gonadal sites of estrogen biosynthesis and function. BMB Rep. 2016, 49, 488–496. [Google Scholar] [CrossRef]
- Corona, G.; Rastrelli, G.; Monami, M.; Saad, F.; Luconi, M.; Lucchese, M.; Facchiano, E.; Sforza, A.; Forti, G.; Mannucci, E.; et al. Body weight loss reverts obesity-associated hypogonadotropic hypogonadism: A systematic review and meta-analysis. Eur. J. Endocrinol. 2013, 168, 829–843. [Google Scholar] [CrossRef]
- Loves, S.; Ruinemans-Koerts, J.; de Boer, H. Letrozole once a week normalizes serum testosterone in obesity-related male hypogonadism. Eur. J. Endocrinol. 2008, 158, 741–747. [Google Scholar] [CrossRef]
- Dhindsa, S.; Furlanetto, R.; Vora, M.; Ghanim, H.; Chaudhuri, A.; Dandona, P. Low Estradiol Concentrations in Men with Subnormal Testosterone Concentrations and Type 2 Diabetes. Diabetes Care 2011, 34, 1854–1859. [Google Scholar] [CrossRef]
- Dhindsa, S.; Miller, M.G.; McWhirter, C.L.; Mager, D.E.; Ghanim, H.; Chaudhuri, A.; Dandona, P. Testosterone Concentrations in Diabetic and Nondiabetic Obese Men. Diabetes Care 2010, 33, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Hammond, R.; Levine, R. The economic impact of obesity in the United States. Diabetes Metab. Syndr. Obesity Targets Ther. 2010, 3, 285–295. [Google Scholar] [CrossRef]
- Ghanim, H.; Dhindsa, S.; Abuaysheh, S.; Batra, M.; Kuhadiya, N.D.; Makdissi, A.; Chaudhuri, A.; Dandona, P. Diminished androgen and estrogen receptors and aromatase levels in hypogonadal diabetic men: Reversal with testosterone. Eur. J. Endocrinol. 2018, 178, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Huhtaniemi, I.T.; Tajar, A.; Lee, D.M.; O’Neill, T.W.; Finn, J.D.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; Giwercman, A.; Han, T.S.; et al. Comparison of serum testosterone and estradiol measurements in 3174 European men using platform immunoassay and mass spectrometry; relevance for the diagnostics in aging men. Eur. J. Endocrinol. 2012, 166, 983–991. [Google Scholar] [CrossRef]
- Pan, W.W.; Myers, M.G., Jr. Leptin and the maintenance of elevated body weight. Nat. Rev. Neurosci. 2018, 19, 95–105. [Google Scholar] [CrossRef]
- Parent, A.; Lebrethon, M.; Gérard, A.; Vandersmissen, E.; Bourguignon, J. Leptin effects on pulsatile gonadotropin releasing hormone secretion from the adult rat hypothalamus and interaction with cocaine and amphetamine regulated transcript peptide and neuropeptide Y. Regul. Pept. 2000, 92, 17–24. [Google Scholar] [CrossRef]
- Myers, M.G., Jr.; Leibel, R.L.; Seeley, R.J.; Schwartz, M.W. Obesity and leptin resistance: Distinguishing cause from effect. Trends Endocrinol. Metab. TEM 2010, 21, 643–651. [Google Scholar] [CrossRef]
- Isidori, A.M.; Caprio, M.; Strollo, F.; Moretti, C.; Frajese, G.; Isidori, A.; Fabbri, A. Leptin and Androgens in Male Obesity: Evidence for Leptin Contribution to Reduced Androgen Levels*. J. Clin. Endocrinol. Metab. 1999, 84, 3673–3680. [Google Scholar] [CrossRef]
- Ishikawa, T.; Fujioka, H.; Ishimura, T.; Takenaka, A.; Fujisawa, M. Expression of leptin and leptin receptor in the testis of fertile and infertile patients. Andrologia 2007, 39, 22–27. [Google Scholar] [CrossRef]
- Jockenhövel, F.; Blum, W.F.; Vogel, E.; Englaro, P.; Müller-Wieland, D.; Reinwein, D.; Rascher, W.; Krone, W. Testosterone Substitution Normalizes Elevated Serum Leptin Levels in Hypogonadal Men. J. Clin. Endocrinol. Metab. 1997, 82, 2510–2513. [Google Scholar] [CrossRef]
- Fui, M.N.T.; Hoermann, R.; Grossmann, M. Effect of testosterone treatment onadipokines and gut hormones in obese men on a hypocaloric diet. J. Endocr. Soc. 2017, 1, 302–312. [Google Scholar]
- Pasquali, R.; Casanueva, F.; Haluzik, M.; van Hulsteijn, L.; Ledoux, S.; Monteiro, M.P.; Salvador, J.; Santini, F.; Toplak, H.; Dekkers, O.M. European Society of Endocrinology Clinical Practice Guideline: Endocrine work-up in obesity. Eur. J. Endocrinol. 2020, 182, G1–G32. [Google Scholar] [CrossRef] [PubMed]
- Sermondade, N.; Faure, C.; Fezeu, L.; Shayeb, A.G.; Bonde, J.P.; Jensen, T.K.; Van Wely, M.; Cao, J.; Martini, A.C.; Eskandar, M.; et al. BMI in relation to sperm count: An updated systematic review and collaborative meta-analysis. Hum. Reprod. Updat. 2012, 19, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Executive summary: Heart disease and stroke statistics-2016 update: A Report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef]
- National Diabetes Statistics Report, 2020|CDC. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 8 May 2023).
- Quesenberry, C.P.; Caan, B.; Jacobson, A. Obesity, Health Services Use, and Health Care Costs Among Members of a Health Maintenance Organization. Arch. Intern. Med. 1998, 158, 466–472. [Google Scholar] [CrossRef]
- Spieker, E.A.; Pyzocha, N. Economic Impact of Obesity. Prim. Care Clin. Off. Pract. 2016, 43, 83–95. [Google Scholar] [CrossRef]
- Hodgson, T.A. Costs of Illness in Cost-Effectiveness Analysis: A Review of the Methodology. Pharmacoeconomics 1994, 6, 536–552. [Google Scholar] [CrossRef]
- Trogdon, J.G.; Finkelstein, E.A.; Hylands, T.; Dellea, P.S.; Kamal-Bahl, S.J. Indirect costs of obesity: A review of the current literature. Obes. Rev. 2008, 9, 489–500. [Google Scholar] [CrossRef]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of Modest Weight Loss in Improving Cardiovascular Risk Factors in Overweight and Obese Individuals with Type 2 Diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef]
- The Look Ahead Research. Eight-year weight losses with an intensive lifestyle intervention: The look AHEAD study. Obesity 2014, 22, 5–13. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, Obesity, and Mortality from Cancer in a Prospectively Studied Cohort of U.S. Adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef] [PubMed]
- Kolb, R.; Sutterwala, F.S.; Zhang, W. Obesity and cancer: Inflammation bridges the two. Curr. Opin. Pharmacol. 2016, 29, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Anisimov, V.N.; Bartke, A. The key role of growth hormone-insulin-IGF-1 signaling in aging and cancer. Crit. Rev. Oncol. 2013, 87, 201–223. [Google Scholar] [CrossRef] [PubMed]
- VanSaun, M.N. Molecular Pathways: Adiponectin and Leptin Signaling in Cancer. Clin. Cancer Res. 2013, 19, 1926–1932. [Google Scholar] [CrossRef]
- Gutiérrez-Cuevas, J.; Santos, A.; Armendariz-Borunda, J. Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases. Int. J. Mol. Sci. 2021, 22, 11629. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, X. Diet and gut microbiome in fatty liver and its associated liver cancer. J. Gastroenterol. Hepatol. 2021, 37, 7–14. [Google Scholar] [CrossRef]
- Mino, M.; Kakazu, E.; Sano, A.; Katsuyama, H.; Hakoshima, M.; Yanai, H.; Aoki, Y.; Imamura, M.; Yamazoe, T.; Mori, T.; et al. Effects of sodium glucose cotransporter 2 inhibitors and pioglitazone on FIB-4 index in metabolic-associated fatty liver disease. Hepatol. Res. 2023, 53, 618–628. [Google Scholar] [CrossRef]
- He, K.; Li, J.; Xi, W.; Ge, J.; Sun, J.; Jing, Z. Dapagliflozin for nonalcoholic fatty liver disease: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2022, 185, 109791. [Google Scholar] [CrossRef]
- Polidorir, D.; Sanghvi, A.; Seeley, R.J.; Hall, K.D. How Strongly Does Appetite Counter Weight Loss? Quantification of the Feedback Control of Human Energy Intake. Obesity 2016, 24, 2289–2295. [Google Scholar] [CrossRef]
- Löffler, M.C.; Betz, M.J.; Blondin, D.P.; Augustin, R.; Sharma, A.K.; Tseng, Y.-H.; Scheele, C.; Zimdahl, H.; Mark, M.; Hennige, A.M.; et al. Challenges in tackling energy expenditure as obesity therapy: From preclinical models to clinical application. Mol. Metab. 2021, 51, 101237. [Google Scholar] [CrossRef]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med Assoc. J. 2020, 192, E875–E891. Available online: https://www.cmaj.ca/content/192/31/E875 (accessed on 24 January 2022). [CrossRef] [PubMed]
- Müller, T.D.; Clemmensen, C.; Finan, B.; DiMarchi, R.D.; Tschöp, M.H. Anti-Obesity Therapy: From Rainbow Pills to Polyagonists. Pharmacol. Rev. 2018, 70, 712–746. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.S.; Dixon, A.F.; Dixon, J.B. Obesity management: Update on orlistat. Vasc. Health Risk Manag. 2007, 3, 817–821. [Google Scholar] [PubMed]
- Greig, S.L.; Keating, G.M. Naltrexone ER/Bupropion ER: A Review in Obesity Management. Drugs 2015, 75, 1269–1280. [Google Scholar] [CrossRef]
- Secher, A.; Jelsing, J.; Baquero, A.F.; Hecksher-Sørensen, J.; Cowley, M.A.; Dalbøge, L.S.; Hansen, G.; Grove, K.L.; Pyke, C.; Raun, K.; et al. The arcuate nucleus mediates GLP-1 receptor agonist liraglutide-dependent weight loss. J. Clin. Investig. 2014, 124, 4473–4488. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.; Brown-Frandsen, K. Liraglutide and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Frias, J.P.; Jastreboff, A.M.; le Roux, C.W.; Sattar, N.; Aizenberg, D.; Mao, H.; Zhang, S.; Ahmad, N.N.; Bunck, M.C.; Benabbad, I.; et al. Tirzepatide Once Weekly for the Treatment of Obesity. Lancet 2023, 387, 205–216. [Google Scholar] [CrossRef]
- Frias, J.P.; Wynne, A.G.; Matyjaszek-Matuszek, B.; Bartaskova, D.; Cox, D.A.; Woodward, B.; Li, Y.G.; Tham, L.S.; Milicevic, Z. Efficacy and safety of an expanded dulaglutide dose range: A phase 2, placebo-controlled trial in patients with type 2 diabetes using metformin. Diabetes Obes. Metab. 2019, 21, 2048–2057. [Google Scholar] [CrossRef]
- Inagaki, N.; Takeuchi, M.; Oura, T.; Imaoka, T.; Seino, Y. Efficacy and safety of tirzepatide monotherapy compared with dulaglutide in Japanese patients with type 2 diabetes (SURPASS J-mono): A double-blind, multicentre, randomised, phase 3 trial. Lancet Diabetes Endocrinol. 2022, 10, 623–633. [Google Scholar] [CrossRef]
- Harris, E. Triple-Hormone Combination Retatrutide Induces 24% Body Weight Loss. JAMA 2023, 330, 306. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, A.M.; Kaplan, L.M.; Frías, J.P.; Wu, Q.; Du, Y.; Gurbuz, S.; Coskun, T.; Haupt, A.; Milicevic, Z.; Hartman, M.L.; et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity—A Phase 2 Trial. N. Engl. J. Med. 2023; online ahead of print. [Google Scholar]
- Pilitsi, E.; Farr, O.M.; Polyzos, S.A.; Perakakis, N.; Nolen-Doerr, E.; Papathanasiou, A.-E.; Mantzoros, C.S. Pharmacotherapy of obesity: Available medications and drugs under investigation. Metabolism 2019, 92, 170–192. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of obesity. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Fildes, A.; Charlton, J.; Rudisill, C.; Littlejohns, P.; Prevost, A.T.; Gulliford, M.C. Probability of an Obese Person Attaining Normal Body Weight: Cohort Study Using Electronic Health Records. Am. J. Public Health 2015, 105, e54–e59. [Google Scholar] [CrossRef] [PubMed]
- Kochkodan, J.; Telem, D.A.; Ghaferi, A.A. Physiologic and psychological gender differences in bariatric surgery. Surg. Endosc. 2017, 32, 1382–1388. [Google Scholar] [CrossRef] [PubMed]
- Young, M.T.; Phelan, M.J.; Nguyen, N.T. A Decade Analysis of Trends and Outcomes of Male vs Female Patients Who Underwent Bariatric Surgery. J. Am. Coll. Surg. 2016, 222, 226–231. [Google Scholar] [CrossRef]
- O’brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2018, 29, 3–14. [Google Scholar] [CrossRef]
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Practical Recommendations of the Obesity Management Task Force of the European Association for the Study of Obesity for the Post-Bariatric Surgery Medical Management. Obes. Facts 2017, 10, 597–632. [Google Scholar] [CrossRef]
- Carrasco, F.; Papapietro, K.; Csendes, A.; Salazar, G.; Echenique, C.; Lisboa, C.; Díaz, E.; Rojas, J. Changes in Resting Energy Expenditure and Body Composition after Weight Loss following Roux-en-Y Gastric Bypass. Obes. Surg. 2007, 17, 608–616. [Google Scholar] [CrossRef]
- Braga, T.G.; das Graças Coelho de Souza, M.; Maranhão, P.A.; Menezes, M.; Dellatorre-Teixeira, L.; Bouskela, E.; Le Roux, C.W.; Kraemer-Aguiar, L.G. Evaluation of Heart Rate Variability and Endothelial Function 3 Months After Bariatric Surgery. Obes Surg. 2020, 30, 2450–2453. [Google Scholar] [CrossRef]
- Iannelli, A.; Anty, R.; Schneck, A.; Tran, A.; Hébuterne, X.; Gugenheim, J. Evolution of low-grade systemic inflammation, insulin resistance, anthropometrics, resting energy expenditure and metabolic syndrome after bariatric surgery: A comparative study between gastric bypass and sleeve gastrectomy. J. Visc. Surg. 2013, 150, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Maser, R.E.; Lenhard, M.J.; Irgau, I.; Wynn, G.M. Impact of surgically induced weight loss on cardiovascular autonomie function: One-year follow-up. Obesity 2007, 15, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-M.; Yu, H.-J.; Lai, H.-S.; Yang, P.-J.; Lin, M.-T.; Lai, F. Improvement of heart rate variability after decreased insulin resistance after sleeve gastrectomy for morbidly obesity patients. Surg. Obes. Relat. Dis. 2014, 11, 557–563. [Google Scholar] [CrossRef]
- Julve, J.; Pardina, E.; Pérez-Cuéllar, M.; Ferrer, R.; Rossell, J.; Baena-Fustegueras, J.A.; Fort, J.M.; Lecube, A.; Blanco-Vaca, F.; Sánchez-Quesada, J.L.; et al. Bariatric surgery in morbidly obese patients improves the atherogenic qualitative properties of the plasma lipoproteins. Atherosclerosis 2014, 234, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Pillar, G.; Peled, R.; Lavie, P. Recurrence of Sleep Apnea Without Concomitant Weight Increase 7.5 Years After Weight Reduction Surgery. Chest 1994, 106, 1702–1704. [Google Scholar] [CrossRef]
- Tremmel, M.; Gerdtham, U.-G.; Nilsson, P.M.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. Available online: https://www.mdpi.com/1660-4601/14/4/435/htm (accessed on 6 January 2022). [CrossRef]
- Finkelstein, E.A.; Trogdon, J.G.; Cohen, J.W.; Dietz, W.H. Annual Medical Spending Attributable to Obesity: Payer-And Service-Specific Estimates. Health Aff. 2009, 28, w822–w831. [Google Scholar] [CrossRef]
- Cawley, J.; Meyerhoefer, C. The medical care costs of obesity: An instrumental variables approach. J. Health Econ. 2012, 31, 219–230. [Google Scholar] [CrossRef]


{kind=link}
| Drug | Mechanism of Action | Dosage | Average Weight Loss | Side Effects | Additional Benefits |
|---|---|---|---|---|---|
| Orlistat | Pancreatic and gastric lipase inhibitor | 120 mg three times daily with meals | Around 5–10% of initial body weight | Gastrointestinal side effects (diarrhea, bloating flatulence) | Improves lipid profile; low risk of systemic side effects |
| Phentermine /Topiramate | Combination of sympathomimetic amine, anorectic and antiepileptic drug | Varies based on titration schedule | Around 5–10% of initial body weight | Dyspepsia, insomnia, constipation, dry mouth, transient peripheral neuropathy | Improves glycemic control; reduces blood pressure |
| Bupropion /Naltrexone | Combination of antidepressant and an opiod receptor antagonist, affecting appetite and reward pathways in hypothalamus | Gradual titration to target dose (varies, maximal daily dose bupropion 360 mg/32 mg naltroxone) | Around 5–10% of initial body weight | Nausea, headache, constipation, insomnia, dry mouth | May improve mood and emotional eating behaviors |
| Liraglutide | GLP-1 receptor agonist | Once daily sc. injection, 3.0 mg | Around 5–10% of initial body weight | Nausea, diarrhea, vomiting, headache, constipation | Improves glycemic control; reduces cardiovascular risk |
| Semaglutide | GLP-1 receptor agonist | 2.4 mg once weekly s.c. | Around 15–20% of initial body weight | Nausea, diarrhea, vomiting, headache, constipation | Improves glycemic control; reduces cardiovascular risk |
| Tirzepatide | Dual GIP/GLP-1/receptor agonist | Once-weekly s.c injection, 15 mg | Around 13–20% of initial body weight | Nausea, diarrhea, vomiting, headache, constipation | Improves glycemic control; cardiovascular risk under investigation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenart-Lipińska, M.; Łuniewski, M.; Szydełko, J.; Matyjaszek-Matuszek, B. Clinical and Therapeutic Implications of Male Obesity. J. Clin. Med. 2023, 12, 5354. https://doi.org/10.3390/jcm12165354
Lenart-Lipińska M, Łuniewski M, Szydełko J, Matyjaszek-Matuszek B. Clinical and Therapeutic Implications of Male Obesity. Journal of Clinical Medicine. 2023; 12(16):5354. https://doi.org/10.3390/jcm12165354
Chicago/Turabian StyleLenart-Lipińska, Monika, Michał Łuniewski, Joanna Szydełko, and Beata Matyjaszek-Matuszek. 2023. "Clinical and Therapeutic Implications of Male Obesity" Journal of Clinical Medicine 12, no. 16: 5354. https://doi.org/10.3390/jcm12165354