
Cytomegalovirus Disease as a Risk Factor for Invasive Fungal Infections in Liver Transplant Recipients under Targeted Antiviral and Antimycotic Prophylaxis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
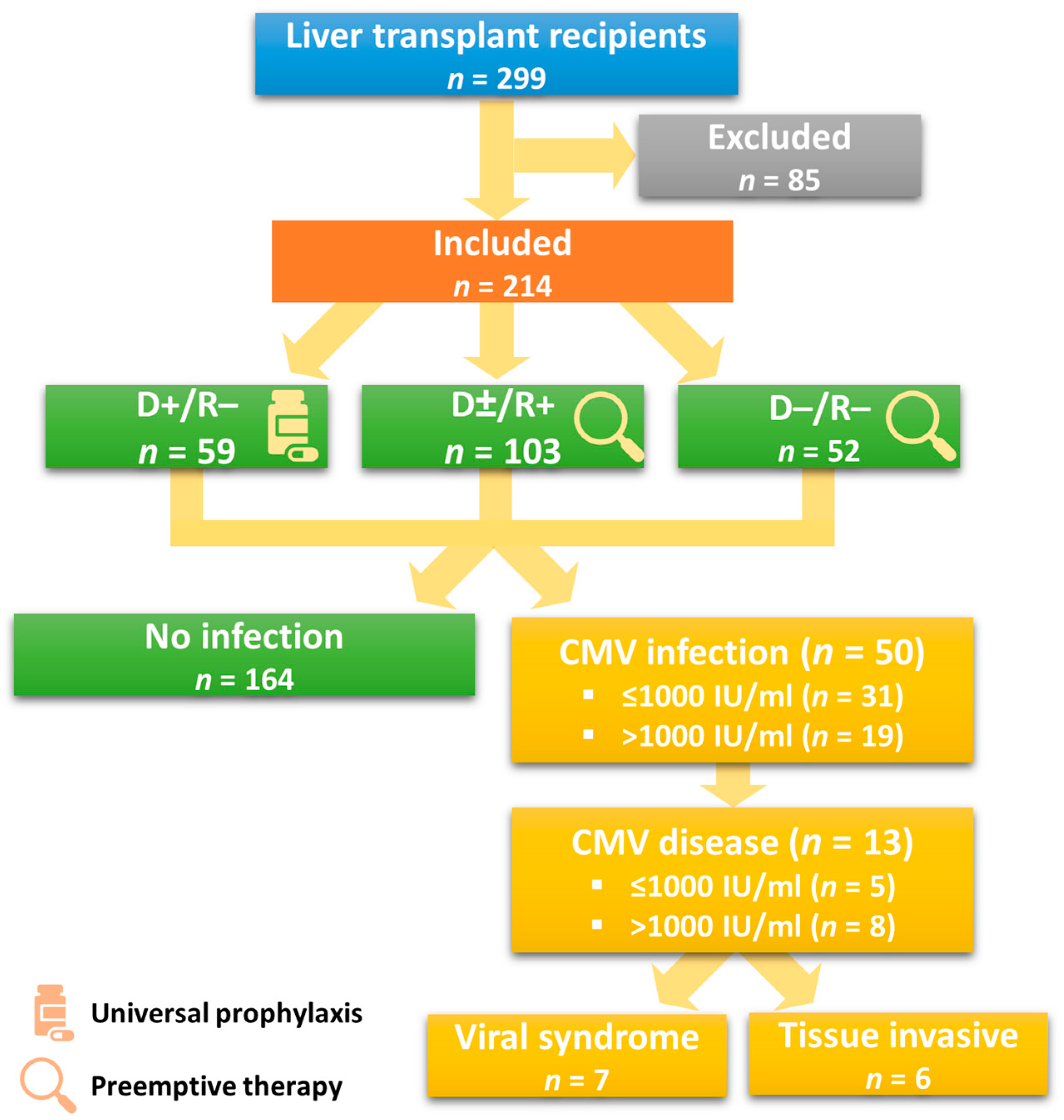
2.1. Patient Selection
2.2. Study Design and Definitions
2.3. Surgical Technique and Immunosuppression
2.4. Antimicrobial Prophylaxis and Surveillance
2.5. Statistical Analyses
3. Results
3.1. Donor, Recipient, and Procedural Characteristics
3.2. Early-Onset CMV-Infection
3.2.1. Incidence and Clinical Characteristics
3.2.2. Direct Effects
3.3. Postoperative Complications
3.4. One-Year Outcome
3.4.1. Mortality
3.4.2. Graft Survival
3.4.3. CMV-Relapse Rate
3.5. Indirect Effects of Early-Onset CMV Infection
3.5.1. Immunological Complications
3.5.2. Vascular Complications
3.5.3. Non-Anastomotic Biliary Strictures (NAS) and Post-Transplant Lymphoproliferative Disorder (PTLD)
4. Discussion
4.1. Future Perspectives and Outlook
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramanan, P.; Razonable, R.R. Cytomegalovirus Infections in Solid Organ Transplantation: A Review. Infect. Chemother. 2013, 45, 260–271. [Google Scholar] [CrossRef] [Green Version]
- Bruminhent, J.; Razonable, R.R. Management of Cytomegalovirus Infection and Disease in Liver Transplant Recipients. World J. Hepatol. 2014, 6, 370–383. [Google Scholar] [CrossRef] [PubMed]
- Humar, A.; Snydman, D. Cytomegalovirus in Solid Organ Transplant Recipients. Am. J. Transplant. 2009, 9 (Suppl. 4), S78–S86. [Google Scholar] [CrossRef] [PubMed]
- Sagedal, S.; Hartmann, A.; Nordal, K.P.; Osnes, K.; Leivestad, T.; Foss, A.; Degré, M.; Fauchald, P.; Rollag, H. Impact of Early Cytomegalovirus Infection and Disease on Long-Term Recipient and Kidney Graft Survival. Kidney Int. 2004, 66, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalil, R.S.N.; Hudson, S.L.; Gaston, R.S. Determinants of Cardiovascular Mortality after Renal Transplantation: A Role for Cytomegalovirus? Am. J. Transplant. 2003, 3, 79–81. [Google Scholar] [CrossRef]
- Fishman, J.A.; Rubin, R.H. Infection in Organ-Transplant Recipients. N. Engl. J. Med. 1998, 338, 1741–1751. [Google Scholar] [CrossRef]
- Rubin, R.H. The Pathogenesis and Clinical Management of Cytomegalovirus Infection in the Organ Transplant Recipient: The End of the “Silo Hypothesis”. Curr. Opin. Infect. Dis. 2007, 20, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, F.; Pimpinelli, F.; Di Domenico, E.G.; Renzi, D.; Gallo, M.T.; Regazzo, G.; Rizzo, M.G.; Gumenyuk, S.; Toma, L.; Marino, M.; et al. Association between CMV and Invasive Fungal Infections After Autologous Stem Cell Transplant in Lymphoproliferative Malignancies: Opportunistic Partnership or Cause-Effect Relationship? Int. J. Mol. Sci. 2019, 20, 1373. [Google Scholar] [CrossRef] [Green Version]
- Yong, M.K.; Ananda-Rajah, M.; Cameron, P.U.; Morrissey, C.O.; Spencer, A.; Ritchie, D.; Cheng, A.C.; Lewin, S.R.; Slavin, M. Cytomegalovirus Reactivation Is Associated with Increased Risk of Late-Onset Invasive Fungal Disease after Allogeneic Hematopoietic Stem Cell Transplantation: A Multicenter Study in the Current Era of Viral Load Monitoring. Biol. Blood Marrow Transplant. 2017, 23, 1961–1967. [Google Scholar] [CrossRef]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [Green Version]
- Green, M.L.; Leisenring, W.; Stachel, D.; Pergam, S.A.; Sandmaier, B.M.; Wald, A.; Corey, L.; Boeckh, M. Efficacy of a Viral Load-Based, Risk-Adapted, Preemptive Treatment Strategy for Prevention of Cytomegalovirus Disease after Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2012, 18, 1687–1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, J.E.; Hyun, S.Y.; Kim, Y.D.; Yoon, S.H.; Hwang, D.Y.; Kim, S.J.; Kim, Y.; Kim, J.S.; Cheong, J.W.; Min, Y.H. Risk Factors for Progression from Cytomegalovirus Viremia to Cytomegalovirus Disease after Allogeneic Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2012, 18, 881–886. [Google Scholar] [CrossRef] [Green Version]
- Boeckh, M.; Leisenring, W.; Riddell, S.R.; Bowden, R.A.; Huang, M.L.; Myerson, D.; Stevens-Ayers, T.; Flowers, M.E.D.; Cunningham, T.; Corey, L. Late Cytomegalovirus Disease and Mortality in Recipients of Allogeneic Hematopoietic Stem Cell Transplants: Importance of Viral Load and T-Cell Immunity. Blood 2003, 101, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Green, M.L.; Leisenring, W.; Xie, H.; Mast, T.C.; Cui, Y.; Sandmaier, B.M.; Sorror, M.L.; Goyal, S.; Özkök, S.; Yi, J.; et al. CMV Viral Load and Mortality after Hematopoietic Cell Transplantation: A Cohort Study in the Era of Preemptive Therapy. Lancet Haematol. 2016, 3, e119–e127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peter Donnelly, J.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Humar, A.; Michaels, M. American Society of Transplantation Recommendations for Screening, Monitoring and Reporting of Infectious Complications in Immunosuppression Trials in Recipients of Organ Transplantation. Am. J. Transplant. 2006, 6, 262–274. [Google Scholar] [CrossRef]
- Ljungman, P.; Boeckh, M.; Hirsch, H.H.; Josephson, F.; Lundgren, J.; Nichols, G.; Pikis, A.; Razonable, R.R.; Miller, V.; Griffiths, P.D. Definitions of Cytomegalovirus Infection and Disease in Transplant Patients for Use in Clinical Trials. Clin. Infect. Dis. 2017, 64, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Lodding, I.P.; Schultz, H.H.; Jensen, J.U.; Kirkby, N.; Perch, M.; Andersen, C.; Lundgren, J.D.; Iversen, M. Cytomegalovirus Viral Load in Bronchoalveolar Lavage to Diagnose Lung Transplant Associated CMV Pneumonia. Transplantation 2018, 102, 326–332. [Google Scholar] [CrossRef]
- Boeckh, M.; Stevens-Ayers, T.; Travi, G.; Huang, M.L.; Cheng, G.S.; Xie, H.; Leisenring, W.; Erard, V.; Seo, S.; Kimball, L.; et al. Cytomegalovirus (CMV) DNA Quantitation in Bronchoalveolar Lavage Fluid From Hematopoietic Stem Cell Transplant Recipients With CMV Pneumonia. J. Infect. Dis. 2017, 215, 1514. [Google Scholar] [CrossRef]
- Rajsic, S.; Breitkopf, R.; Bachler, M.; Treml, B. Diagnostic Modalities in Critical Care: Point-of-Care Approach. Diagnostics 2021, 11, 2202. [Google Scholar] [CrossRef]
- Chemaly, R.F.; Chou, S.; Einsele, H.; Griffiths, P.; Avery, R.; Razonable, R.R.; Mullane, K.M.; Kotton, C.; Lundgren, J.; Komatsu, T.E.; et al. Definitions of Resistant and Refractory Cytomegalovirus Infection and Disease in Transplant Recipients for Use in Clinical Trials. Clin. Infect. Dis. 2019, 68, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Demetris, A.J.; Bellamy, C.; Hübscher, S.G.; O’Leary, J.; Randhawa, P.S.; Feng, S.; Neil, D.; Colvin, R.B.; McCaughan, G.; Fung, J.J.; et al. 2016 Comprehensive Update of the Banff Working Group on Liver Allograft Pathology: Introduction of Antibody-Mediated Rejection. Am. J. Transplant. 2016, 16, 2816–2835. [Google Scholar] [CrossRef] [Green Version]
- Koval, C. Echinocandins for Antifungal Prophylaxis in Liver Transplant Recipients: Advance in the Field or Variation on a Theme? Liver Transplant. 2016, 22, 396–398. [Google Scholar] [CrossRef]
- Breitkopf, R.; Treml, B.; Simmet, K.; Bukumirić, Z.; Fodor, M.; Senoner, T.; Rajsic, S. Incidence of Invasive Fungal Infections in Liver Transplant Recipients under Targeted Echinocandin Prophylaxis. J. Clin. Med. 2023, 12, 1520. [Google Scholar] [CrossRef] [PubMed]
- Breitkopf, R.; Treml, B.; Senoner, T.; Bukumirić, Z.; Rajsic, S. Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients. J. Fungi 2023, 9, 272. [Google Scholar] [CrossRef]
- Damlaj, M.; Khalid, F.; Alahmari, B.; Alaskar, A.; Ghazi, S.; Johani, S.; AlSaedy, A.; Bosaeed, M.; Alhejazi, A.; Al-Zahrani, M. Optimal Pre-Emptive Cytomegalovirus Therapy Threshold in a Patient Population with High Prevalence of Seropositive Status. Curr. Res. Transl. Med. 2020, 68, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Acquier, M.; Taton, B.; Alain, S.; Garrigue, I.; Mary, J.; Pfirmann, P.; Visentin, J.; Hantz, S.; Merville, P.; Kaminski, H.; et al. Cytomegalovirus DNAemia Requiring (Val)Ganciclovir Treatment for More Than 8 Weeks Is a Key Factor in the Development of Antiviral Drug Resistance. Open Forum Infect. Dis. 2023, 10, ofad018. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/ (accessed on 6 June 2023).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 6 June 2023).
- Plachouras, D.; Lepape, A.; Suetens, C. ECDC Definitions and Methods for the Surveillance of Healthcare-Associated Infections in Intensive Care Units. Intensiv. Care Med. 2018, 44, 2216–2218. [Google Scholar] [CrossRef] [Green Version]
- Zuhair, M.; Smit, G.S.A.; Wallis, G.; Jabbar, F.; Smith, C.; Devleesschauwer, B.; Griffiths, P. Estimation of the Worldwide Seroprevalence of Cytomegalovirus: A Systematic Review and Meta-Analysis. Rev. Med. Virol. 2019, 29, e2034. [Google Scholar] [CrossRef] [Green Version]
- Desai, A.N.; Malani, P.N. Preventing Cytomegalovirus Infection after Liver Transplant: An Evolving Approach. JAMA 2020, 323, 1388. [Google Scholar] [CrossRef]
- Razonable, R.R. Epidemiology of Cytomegalovirus Disease in Solid Organ and Hematopoietic Stem Cell Transplant Recipients. Am. J. Health Pharm. 2005, 62, S7–S13. [Google Scholar] [CrossRef] [PubMed]
- Winston, D.J.; Emmanouilides, C.; Busuttil, R.W. Infections in Liver Transplant Recipients. Clin. Infect. Dis. 1995, 21, 1077–1091. [Google Scholar] [CrossRef] [PubMed]
- Paya, C.V.; Marin, E.; Keating, M.; Dickson, R.; Porayko, M.; Wiesner, R. Solid Organ Transplantation: Results and Implications of Acyclovir Use in Liver Transplants. J. Med. Virol. 1993, 41 (Suppl. 1), 123–127. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, I.; Halme, L.; Höckerstedt, K.; Krogerus, L.; Taskinen, E. Cytomegalovirus Infection of the Liver Transplant: Virological, Histological, Immunological, and Clinical Observations. Transpl. Infect. Dis. 2006, 8, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Kotton, C.N.; Kamar, N. New Insights on CMV Management in Solid Organ Transplant Patients: Prevention, Treatment, and Management of Resistant/Refractory Disease. Infect. Dis. Ther. 2023, 12, 333. [Google Scholar] [CrossRef]
- Young, P.G.; Rubin, J.; Angarone, M.; Flaherty, J.; Penugonda, S.; Stosor, V.; Ison, M.G. Ganciclovir-Resistant Cytomegalovirus Infection in Solid Organ Transplant Recipients: A Single-Center Retrospective Cohort Study. Transpl. Infect. Dis. 2016, 18, 390–395. [Google Scholar] [CrossRef]
- Hantz, S.; Garnier-Geoffroy, F.; Mazeron, M.C.; Garrigue, I.; Merville, P.; Mengelle, C.; Rostaing, L.; Saint Marcoux, F.; Essig, M.; Rerolle, J.P.; et al. Drug-Resistant Cytomegalovirus in Transplant Recipients: A French Cohort Study. J. Antimicrob. Chemother. 2010, 65, 2628–2640. [Google Scholar] [CrossRef] [Green Version]
- Myhre, H.A.; Haug Dorenberg, D.; Kristiansen, K.I.; Rollag, H.; Leivestad, T.; Åsberg, A.; Hartmann, A. Incidence and Outcomes of Ganciclovir-Resistant Cytomegalovirus Infections in 1244 Kidney Transplant Recipients. Transplantation 2011, 92, 217–223. [Google Scholar] [CrossRef]
- Fisher, C.E.; Knudsen, J.L.; Lease, E.D.; Jerome, K.R.; Rakita, R.M.; Boeckh, M.; Limaye, A.P. Risk Factors and Outcomes of Ganciclovir-Resistant Cytomegalovirus Infection in Solid Organ Transplant Recipients. Clin. Infect. Dis. 2017, 65, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Lurain, N.S.; Chou, S. Antiviral Drug Resistance of Human Cytomegalovirus. Clin. Microbiol. Rev. 2010, 23, 689–712. [Google Scholar] [CrossRef] [Green Version]
- Rolling, K.E.; Jorgenson, M.R.; Descourouez, J.L.; Mandelbrot, D.A.; Redfield, R.R.; Smith, J.A. Ganciclovir-Resistant Cytomegalovirus Infection in Abdominal Solid Organ Transplant Recipients: Case Series and Review of the Literature. Pharmacotherapy 2017, 37, 1258–1271. [Google Scholar] [CrossRef]
- Cherrier, L.; Nasar, A.; Goodlet, K.J.; Nailor, M.D.; Tokman, S.; Chou, S. Emergence of Letermovir Resistance in a Lung Transplant Recipient with Ganciclovir-Resistant Cytomegalovirus Infection. Am. J. Transplant. 2018, 18, 3060–3064. [Google Scholar] [CrossRef] [Green Version]
- Strauss, R.G. Optimal Prevention of Transfusion-Transmitted Cytomegalovirus (TTCMV) Infection by Modern Leukocyte Reduction Alone: CMV Sero/Antibody-Negative Donors Needed Only for Leukocyte Products. Transfusion 2016, 56, 1921–1924. [Google Scholar] [CrossRef]
- Singh, N.; Wannstedt, C.; Keyes, L.; Wagener, M.M.; Cacciarelli, T.V. Who among Cytomegalovirus-Seropositive Liver Transplant Recipients Is at Risk for Cytomegalovirus Infection? Liver Transplant. 2005, 11, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Gane, E.; Saliba, F.; Valdecasas, G.J.C.; O’Grady, J.; Pescovitz, M.D.; Lyman, S.; Robinson, C.A. Randomised Trial of Efficacy and Safety of Oral Ganciclovir in the Prevention of Cytomegalovirus Disease in Liver-Transplant Recipients. Lancet 1997, 350, 1729–1733. [Google Scholar] [CrossRef]
- Croen, K.D. Latency of the Human Herpesviruses. Annu. Rev. Med. 1991, 42, 61–67. [Google Scholar] [CrossRef]
- Lautenschlager, I.; Loginov, R.; Mäkisalo, H.; Höckerstedt, K. Prospective Study on CMV-Reactivations under Preemptive Strategy in CMV-Seropositive Adult Liver Transplant Recipients. J. Clin. Virol. 2013, 57, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Beam, E.; Razonable, R.R. Cytomegalovirus in Solid Organ Transplantation: Epidemiology, Prevention, and Treatment. Curr. Infect. Dis. Rep. 2012, 14, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Breitkopf, R.; Treml, B.; Bukumiric, Z.; Innerhofer, N.; Fodor, M.; Rajsic, S. Invasive Fungal Infections: The Early Killer after Liver Transplantation. J. Fungi 2023, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- Senoner, T.; Breitkopf, R.; Treml, B.; Rajsic, S. Invasive Fungal Infections after Liver Transplantation. J. Clin. Med. 2023, 12, 3238. [Google Scholar] [CrossRef]
- Ingold, L.; Halter, J.; Martinez, M.; Amico, P.; Wehmeier, C.; Hirt-Minkowski, P.; Steiger, J.; Dickenmann, M.; Schaub, S. Short- and Long-Term Impact of Neutropenia within the First Year after Kidney Transplantation. Transpl. Int. 2021, 34, 1875–1885. [Google Scholar] [CrossRef]
- Zafrani, L.; Truffaut, L.; Kreis, H.; Etienne, D.; Rafat, C.; Lechaton, S.; Anglicheau, D.; Zuber, J.; Ciroldi, M.; Thervet, E.; et al. Incidence, Risk Factors and Clinical Consequences of Neutropenia Following Kidney Transplantation: A Retrospective Study. Am. J. Transplant. 2009, 9, 1816–1825. [Google Scholar] [CrossRef]
- Jorgenson, M.R.; Descourouez, J.L.; Garg, N.; Parajuli, S.; Mandelbrot, D.A.; Odorico, J.S.; Saddler, C.M.; Smith, J.A. The Addition of Adjunctive Letermovir to Valganciclovir for Refractory Cytomegalovirus Viremia in Kidney Transplant Recipients. Transpl. Infect. Dis. 2021, 23, e13693. [Google Scholar] [CrossRef]
- Kotton, C.N. CMV: Prevention, Diagnosis and Therapy. Am. J. Transplant. 2013, 13 (Suppl. 3), 24–40. [Google Scholar] [CrossRef]
- Brar, S.; Berry, R.; Raval, A.D.; Tang, Y.; Vincenti, F.; Skartsis, N. Outcomes among CMV-Mismatched and Highly Sensitized Kidney Transplants Recipients Who Develop Neutropenia. Clin. Transplant. 2022, 36, e14583. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, R.P.; Akin, B.; Henry, M.L.; Bumgardner, G.L.; Elkhammas, E.A.; Rajab, A.; Ferguson, R.M. The Impact of Mycophenolate Mofetil Dosing Patterns on Clinical Outcome after Renal Transplantation. Clin. Transplant. 2003, 17, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Glander, P.; Hambach, P.; Braun, K.P.; Fritsche, L.; Giessing, M.; Mai, I.; Einecke, G.; Waiser, J.; Neumayer, H.H.; Budde, K. Pre-Transplant Inosine Monophosphate Dehydrogenase Activity Is Associated with Clinical Outcome after Renal Transplantation. Am. J. Transplant. 2004, 4, 2045–2051. [Google Scholar] [CrossRef]
- Knoll, G.A.; Macdonald, I.; Khan, A.; Van Walraven, C. Mycophenolate Mofetil Dose Reduction and the Risk of Acute Rejection after Renal Transplantation. J. Am. Soc. Nephrol. 2003, 14, 2381–2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasullo, M.; Patel, M.; Khanna, L.; Shah, T. Post-Transplant Biliary Complications: Advances in Pathophysiology, Diagnosis, and Treatment. BMJ Open Gastroenterol. 2022, 9, e000778. [Google Scholar] [CrossRef]
- Seehofer, D.; Eurich, D.; Veltzke-Schlieker, W.; Neuhaus, P. Biliary Complications After Liver Transplantation: Old Problems and New Challenges. Am. J. Transplant. 2013, 13, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Buis, C.I.; Verdonk, R.C.; Van Der Jagt, E.J.; Van Der Hilst, C.S.; Slooff, M.J.H.; Haagsma, E.B.; Porte, R.J. Nonanastomotic Biliary Strictures After Liver Transplantation, Part 1: Radiological Features and Risk Factors for Early Vs. Late Presentation. Liver Transplant. 2007, 13, 708–718. [Google Scholar] [CrossRef]
- Rauber, C.; Bartelheimer, K.; Zhou, T.; Rupp, C.; Schnitzler, P.; Schemmer, P.; Sauer, P.; Weiss, K.H.; Gotthardt, D.N. Prevalence of Human Herpesviruses in Biliary Fluid and Their Association with Biliary Complications after Liver Transplantation. BMC Gastroenterol. 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sun, L.Y.; Zhu, Z.J.; Qu, W. Novel Approach for the Diagnosis of Occult Cytomegalovirus Cholangitis after Pediatric Liver Transplantation: A Case Report. World J. Clin. Cases 2020, 8, 2597–2602. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Y.; Zhang, J.R.; Sun, L.Y.; Zhu, Z.J.; Wei, L.; Qu, W.; Zeng, Z.G.; Liu, Y.; Zhao, X.Y. Impact of Cytomegalovirus Infection on Biliary Disease after Liver Transplantation—Maybe an Essential Factor. World J. Clin. Cases 2021, 9, 10792. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Sullivan, T.; Ali, M.; Dunn, D.; Patel, G.; Huprikar, S. Low-Dose Valganciclovir for Cytomegalovirus Prophylaxis in Intermediate-Risk Liver Transplantation Recipients. Liver Transplant. 2018, 24, 616–622. [Google Scholar] [CrossRef] [Green Version]
- El Helou, G.; Razonable, R.R. Letermovir for the Prevention of Cytomegalovirus Infection and Disease in Transplant Recipients: An Evidence-Based Review. Infect. Drug Resist. 2019, 12, 1481. [Google Scholar] [CrossRef] [Green Version]
- Kropeit, D.; von Richter, O.; Stobernack, H.P.; Rübsamen-Schaeff, H.; Zimmermann, H. Pharmacokinetics and Safety of Letermovir Coadministered With Cyclosporine A or Tacrolimus in Healthy Subjects. Clin. Pharmacol. Drug Dev. 2018, 7, 9–21. [Google Scholar] [CrossRef]
- Ziemann, M.; Thiele, T. Transfusion-Transmitted CMV Infection—Current Knowledge and Future Perspectives. Transfus. Med. 2017, 27, 238–248. [Google Scholar] [CrossRef]
- Gotthardt, D.N.; Senft, J.; Sauer, P.; Weiss, K.H.; Flechtenmacher, C.; Eckerle, I.; Schaefer, Y.; Schirmacher, P.; Stremmel, W.; Schemmer, P.; et al. Occult Cytomegalovirus Cholangitis as a Potential Cause of Cholestatic Complications after Orthotopic Liver Transplantation? A Study of Cytomegalovirus DNA in Bile. Liver Transplant. 2013, 19, 1142–1150. [Google Scholar] [CrossRef]
- Griffiths, P.D.; Stanton, A.; McCarrell, E.; Smith, C.; Osman, M.; Harber, M.; Davenport, A.; Jones, G.; Wheeler, D.C.; OBeirne, J.; et al. Cytomegalovirus Glycoprotein-B Vaccine with MF59 Adjuvant in Transplant Recipients: A Phase 2 Randomised Placebo-Controlled Trial. Lancet 2011, 377, 1256–1263. [Google Scholar] [CrossRef] [Green Version]
- Berencsi, K.; Gyulai, Z.; Gönczöl, E.; Pincus, S.; Cox, W.I.; Michelson, S.; Kari, L.; Meric, C.; Cadoz, M.; Zahradnik, J.; et al. A Canarypox Vector-Expressing Cytomegalovirus (CMV) Phosphoprotein 65 Induces Long-Lasting Cytotoxic T Cell Responses in Human CMV-Seronegative Subjects. J. Infect. Dis. 2001, 183, 1171–1179. [Google Scholar] [CrossRef]
- Schleiss, M.R.; Lacayo, J.C.; Belkaid, Y.; McGregor, A.; Stroup, G.; Rayner, J.; Alterson, K.; Chulay, J.D.; Smith, J.F. Preconceptual Administration of an Alphavirus Replicon UL83 (Pp65 Homolog) Vaccine Induces Humoral and Cellular Immunity and Improves Pregnancy Outcome in the Guinea Pig Model of Congenital Cytomegalovirus Infection. J. Infect. Dis. 2007, 195, 789–798. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Reap, E.A.; Katen, K.; Watson, A.; Smith, K.; Norberg, P.; Olmsted, R.A.; Hoeper, A.; Morris, J.; Negri, S.; et al. Randomized, Double-Blind, Phase 1 Trial of an Alphavirus Replicon Vaccine for Cytomegalovirus in CMV Seronegative Adult Volunteers. Vaccine 2009, 28, 484–493. [Google Scholar] [CrossRef]
- Flatz, L.; Hegazy, A.N.; Bergthaler, A.; Verschoor, A.; Claus, C.; Fernandez, M.; Gattinoni, L.; Johnson, S.; Kreppel, F.; Kochanek, S.; et al. Development of Replication-Defective Lymphocytic Choriomeningitis Virus Vectors for the Induction of Potent CD8+ T Cell Immunity. Nat. Med. 2010, 16, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Kirchmeier, M.; Fluckiger, A.C.; Soare, C.; Bozic, J.; Ontsouka, B.; Ahmed, T.; Diress, A.; Pereira, L.; Schödel, F.; Plotkin, S.; et al. Enveloped Virus-like Particle Expression of Human Cytomegalovirus Glycoprotein B Antigen Induces Antibodies with Potent and Broad Neutralizing Activity. Clin. Vaccine Immunol. 2014, 21, 174–180. [Google Scholar] [CrossRef] [Green Version]
- La Rosa, C.; Longmate, J.; Martinez, J.; Zhou, Q.; Kaltcheva, T.I.; Tsai, W.; Drake, J.; Carroll, M.; Wussow, F.; Chiuppesi, F.; et al. MVA Vaccine Encoding CMV Antigens Safely Induces Durable Expansion of CMV-Specific T Cells in Healthy Adults. Blood 2017, 129, 114–125. [Google Scholar] [CrossRef]
- Zhong, J.; Khanna, R. Delineating the Role of CD4+ T Cells in the Activation of Human Cytomegalovirus-Specific Immune Responses Following Immunization with Ad-GBCMVpoly Vaccine: Implications for Vaccination of Immunocompromised Individuals. J. Gen. Virol. 2010, 91, 2994–3001. [Google Scholar] [CrossRef]
- Binjawadagi, B.; Ma, Y.; Binjawadagi, R.; Brakel, K.; Harder, O.; Peeples, M.; Li, J.; Niewiesk, S. Mucosal Delivery of Recombinant Vesicular Stomatitis Virus Vectors Expressing Envelope Proteins of Respiratory Syncytial Virus Induces Protective Immunity in Cotton Rats. J. Virol. 2021, 95, e02345-20. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | All Patients (n = 214) | No CMV Infection (n = 164) | CMV Infection (n = 50) | p-Value | Missing (n/Total) | |
|---|---|---|---|---|---|---|
| Age (years) | 57.3 ± 11.1 | 57.9 ± 10.6 | 55.5 ± 12.8 | 0.189 | 0/214 | |
| Male sex | 163 (76.2) | 127 (77.4) | 36 (72.0) | 0.451 | 0/214 | |
| Height (cm) | 174.2 ± 8.5 | 174.5 ± 8.2 | 173.3 ± 9.4 | 0.405 | 0/214 | |
| Weight (kg) | 81.4 ± 16.3 | 82.4 ± 16.0 | 78.4 ± 17.2 | 0.131 | 0/214 | |
| Body mass index (kg/m2) | 26.8 ± 5.0 | 27.0 ± 5.0 | 26.0 ± 4.7 | 0.182 | 0/214 | |
| SAPS III score | 44.8 ± 8.5 | 44.9 ± 8.5 | 44.7 ± 8.7 | 0.897 | 6/214 | |
| MELD score | 13 (6–40) | 13 (6–40) | 13 (6–40) | 0.525 | 10/214 | |
| Charlson comorbidity index | 4 (0–10) | 4 (0–10) | 4 (0–8) | 0.968 | 2/214 | |
| ICU length of stay (days) | 5 (1–117) | 5 (1–117) | 5.5 (3–40) | 0.425 | 0/214 | |
| Invasive fungal infection | 26 (12.1) | 18 (11.0) | 8 (16.0) | 0.332 | 0/214 | |
| Underlying Disease | 0.855 | 0/214 | ||||
| Acute liver failure | 10 (4.7) | 7 (4.3) | 3 (6.0) | 0.702 | 0/214 | |
| Tumors | 89 (41.6) | 68 (41.5) | 21 (42.0) | 1.000 | 0/214 | |
| Hepatocellular carcinoma | 82 (92.1) | 62 (37.8) | 20 (40.0) | 0.868 | 0/214 | |
| Cholangiocellular carcinoma | 3 (3.4) | 2 (1.2) | 1 (2.0) | 0.552 | 0/214 | |
| Neuroendocrine tumor | 3 (3.4) | 3 (1.8) | 0 (0) | 1.000 | 0/214 | |
| Polycystic liver disease | 1 (1.1) | 1 (0.6) | 0 (0) | 1.000 | 0/214 | |
| Cirrhosis | 68 (31.8) | 52 (31.7) | 16 (32.0) | 1.000 | 0/214 | |
| Alcoholic cirrhosis | 51 (23.8) | 41 (25.0) | 10 (20.0) | 0.571 | 0/214 | |
| Virus related cirrhosis | 9 (4.2) | 6 (3.7) | 3 (6.0) | 0.439 | 0/214 | |
| Autoimmune cirrhosis | 8 (3.7) | 5 (3.0) | 3 (6.0) | 0.393 | 0/214 | |
| Cholestatic disease | 15 (7.0) | 12 (7.3) | 3 (6.0) | 1.000 | 0/214 | |
| Nonalcoholic steatohepatitis | 14 (6.5) | 12 (7.3) | 2 (4.0) | 0.529 | 0/214 | |
| Metabolic disease | 10 (4.7) | 7 (4.3) | 3 (6.0) | 0.702 | 0/214 | |
| Budd-Chiari syndrome | 6 (2.8) | 5 (3.0) | 1 (2.0) | 1.000 | 0/214 | |
| Other | 2 (0.9) | 1 (0.6) | 1 (2.0) | 0.414 | 0/214 | |
| All | No Disease | CMV Disease | Missing | |||
|---|---|---|---|---|---|---|
| Characteristics | (n = 214) | (n = 201) | (n = 13) | p-Value | (n/Total) | |
| Primary non-function | 2 (1.1) | 2 (1.0) | 0 (0) | 1.000 | 0/214 | |
| Early allograft dysfunction | 56 (30.9) | 50 (24.9) | 6 (46.2) | 0.107 | 0/214 | |
| Reoperation | 81 (37.9) | 74 (36.8) | 7 (53.9) | 0.247 | 0/214 | |
| Bile leak | 20 (10.8) | 17 (8.5) | 3 (23.1) | 0.109 | 0/214 | |
| Acute kidney injury | 94 (43.9) | 87 (43.3) | 7 (53.9) | 0.567 | 0/214 | |
| Invasive fungal infection | 26 (12.1) | 21 (10.4) | 5 (38.5) | 0.012 | 0/214 | |
| Candidiasis | 19 (8.9) | 15 (7.5) | 4 (30.8) | 0.018 | ||
| Aspergillosis | 5 (2.3) | 4 (2.0) | 1 (7.7) | 0/214 | ||
| Other | 2 (0.9) | 2 (1.0) | 0 (0) | |||
| Overall mortality | 29 (13.6) | 23 (11.4) | 6 (46.2) | 0.003 | 0/214 | |
| Time to death | 48 (1–340) | 57 (1–340) | 44 (26–242) | 0.733 | 0/214 | |
| Graft failure | 17 (7.9) | 16 (8.0) | 1 (7.7) | 1.000 | 0/214 | |
| Time to onset | 52 (1–300) | 35 (1–300) | 52 (52–52) | 1.000 | 0/214 | |
| Re-transplantation | 9 (4.2) | 8 (4.0) | 1 (7.7) | 0.437 | 0/214 | |
| Immunological complications | 23 (10.7) | 20 (10.0) | 3 (23.1) | 0.167 | 9/214 | |
| Acute cellular rejection (early-onset) | 8 (34.8) | 6 (30.0) | 2 (66.7) | 0.084 | 9/214 | |
| Acute cellular rejection (late-onset) | 12 (52.2) | 12 (60.0) | 0 (0) | 1.000 | 9/214 | |
| Chronic rejection | 1 (4.3) | 1 (5.0) | 0 (0) | 1.000 | 9/214 | |
| Antibody-mediated rejection | 1 (4.3) | 1(5.0) | 0 (0) | 1.000 | 9/214 | |
| Graft-versus-host disease | 1 (4.3) | 0 (0) | 1 (33.3) | 0.065 | 9/214 | |
| Vascular complications | 30 (14.0) | 29 (14.7) | 1 (7.7) | 1.000 | 9/214 | |
| HAT (early-onset) | 8 (26.7) | 8 (27.6) | 0 (0) | 1.000 | 9/214 | |
| HAT (late-onset) | 3 (10.0) | 3 (10.3) | 0 (0) | 1.000 | 9/214 | |
| Portal vein thrombosis | 10 (33.3) | 10 (34.5) | 0 (0) | 1.000 | 9/214 | |
| Venous thromboembolism | 4 (13.3) | 4 (13.8) | 0 (0) | 1.000 | 9/214 | |
| Arterial thrombotic disease | 5 (16.7) | 4 (13.8) | 1 (100.0) | 0.282 | 9/214 | |
| Non-anastomic biliary strictures | 27 (12.6) | 24 (11.9) | 3 (23.1) | 0.386 | 9/214 | |
| Ischemic-type biliary lesion | 15 (7.0) | 12 (50.0) | 3 (100.0) | 0.058 | 9/214 | |
| Intrahepatic biliary lesions | 12 (5.6) | 12 (50.0) | 0 (0) | 1.000 | 9/214 | |
| Post-transplant lymphoproliferative disorder | 2 (0.9) | 1 (0.5) | 1 (7.7) | 0.123 | 9/214 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breitkopf, R.; Treml, B.; Bukumiric, Z.; Innerhofer, N.; Fodor, M.; Radovanovic Spurnic, A.; Rajsic, S. Cytomegalovirus Disease as a Risk Factor for Invasive Fungal Infections in Liver Transplant Recipients under Targeted Antiviral and Antimycotic Prophylaxis. J. Clin. Med. 2023, 12, 5198. https://doi.org/10.3390/jcm12165198
Breitkopf R, Treml B, Bukumiric Z, Innerhofer N, Fodor M, Radovanovic Spurnic A, Rajsic S. Cytomegalovirus Disease as a Risk Factor for Invasive Fungal Infections in Liver Transplant Recipients under Targeted Antiviral and Antimycotic Prophylaxis. Journal of Clinical Medicine. 2023; 12(16):5198. https://doi.org/10.3390/jcm12165198
Chicago/Turabian StyleBreitkopf, Robert, Benedikt Treml, Zoran Bukumiric, Nicole Innerhofer, Margot Fodor, Aleksandra Radovanovic Spurnic, and Sasa Rajsic. 2023. "Cytomegalovirus Disease as a Risk Factor for Invasive Fungal Infections in Liver Transplant Recipients under Targeted Antiviral and Antimycotic Prophylaxis" Journal of Clinical Medicine 12, no. 16: 5198. https://doi.org/10.3390/jcm12165198