
Norwegian Version of the Chelsea Critical Care Physical Assessment Tool (CPAx-NOR): Translation, Face Validity, Cross-Cultural Adaptation and Inter-Rater Reliability
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chelsea Critical Care Physical Assessment—CPAx
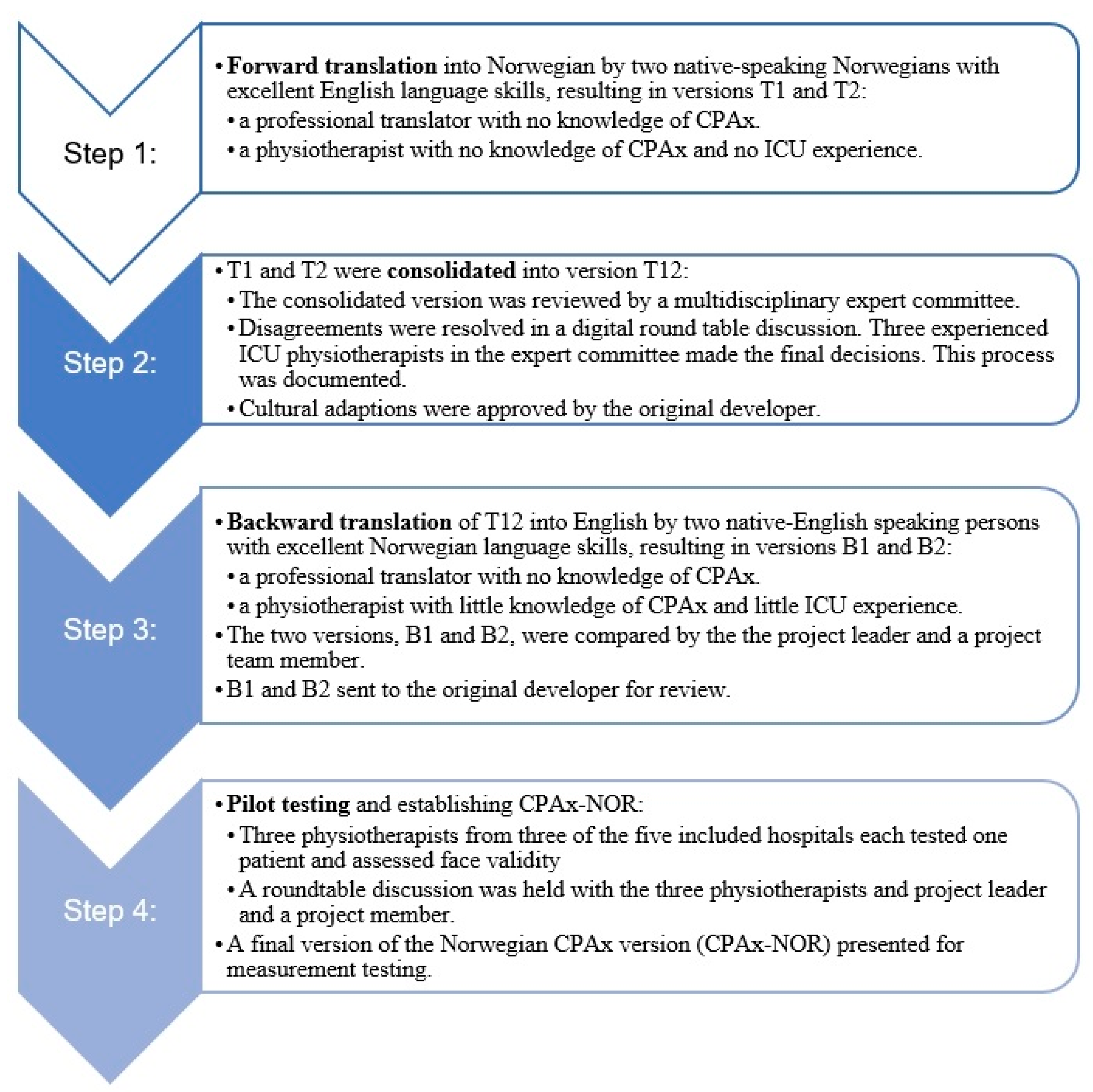
2.1.1. Stage I. Translation and Cross-Cultural Adaption
2.1.2. Face Validity
2.2. Stage II. Evaluation of CPAx-NOR Inter-Rater Reliability
Design and Setting
2.3. Participants and Patients
2.4. Data Collection, Procedures and Measurement
2.5. Inter-Rater Reliability
2.6. Change in Scores during Patient Trajectory
2.7. Statistical Analysis
3. Results
3.1. Translation, Cross-Cultural Adaption and Face Validity
3.2. Patient Population at Start of Physiotherapy (A) and at Discharge from the ICU (B)
3.3. Inter-Rater Reliability and Limits of Agreement
3.4. Change in Scores of CPAx-NOR
3.5. Floor and Ceiling Effects
4. Discussion
4.1. Reliability
4.2. Change in Scores
4.3. Floor and Ceiling Effects
4.4. Perspective, Further Research and Clinical Implications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fan, E.; Cheek, F.; Chlan, L.; Gosselink, R.; Hart, N.; Herridge, M.S.; Hopkins, R.O.; Hough, C.L.; Kress, J.P.; Latronico, N.; et al. An official American Thoracic Society Clinical Practice guideline: The diagnosis of intensive care unit–acquired weakness in adults. Am. J. Respir. Crit. Care Med. 2014, 190, 1437–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S.; Tansey, C.M.; Matte, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohtake, P.J.; Lee, A.C.; Scott, J.C.; Hinman, R.S.; Ali, N.A.; Hinkson, C.R.; Needham, D.M.; Shutter, L.; Smith-Gabai, H.; Spires, M.C.; et al. Physical Impairments Associated with Post-Intensive Care Syndrome: Systematic Review Based on the World Health Organization’s International Classification of Functioning, Disability and Health Framework. Phys. Ther. 2018, 98, 631–645. [Google Scholar] [CrossRef] [Green Version]
- Gandotra, S.; Lovato, J.; Case, D.; Bakhru, R.N.; Gibbs, K.; Berry, M.; Files, D.C.; Morris, P.E. Physical Function Trajectories in Survivors of Acute Respiratory Failure. Ann. Am. Thorac. Soc. 2019, 16, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, B.B.; Suri, R.; Suchyta, M.R.; Digrande, K.F.; Sherwood, K.D.; Colantuoni, E.; Dinglas, V.D.; Needham, D.M.; Hopkins, R.O. Return to work after critical illness: A systematic review and meta-analysis. Thorax 2020, 75, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Gosselink, R.; Bott, J.; Johnson, M.; Dean, E.; Nava, S.; Norrenberg, M.; Schönhofer, B.; Stiller, K.; van de Leur, H.; Vincent, J.L. Physiotherapy for adult patients with critical illness: Recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Med. 2008, 34, 1188–1199. [Google Scholar] [CrossRef]
- Arias-Fernandez, P.; Romero-Martin, M.; Gomez-Salgado, J.; Fernandez-Garcia, D. Rehabilitation and early mobilization in the critical patient: Systematic review. J. Phys. Ther. Sci. 2018, 30, 1193–1201. [Google Scholar] [CrossRef] [Green Version]
- Sommers, J.; Engelbert, R.H.; Dettling-Ihnenfeldt, D.; Gosselink, R.; Spronk, P.E.; Nollet, F.; van der Schaaf, M. Physiotherapy in the intensive care unit: An evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin. Rehabil. 2015, 29, 1051–1063. [Google Scholar] [CrossRef] [Green Version]
- Stiller, K. Physiotherapy in intensive care: An updated systematic review. Chest 2013, 144, 825–847. [Google Scholar] [CrossRef]
- Parry, S.M.; Huang, M.; Needham, D.M. Evaluating physical functioning in critical care: Considerations for clinical practice and research. Crit. Care 2017, 21, 249. [Google Scholar] [CrossRef] [Green Version]
- Parry, S.M.; Granger, C.L.; Berney, S.; Jones, J.; Beach, L.; El-Ansary, D.; Koopman, R.; Denehy, L. Assessment of impairment and activity limitations in the critically ill: A systematic review of measurement instruments and their clinimetric properties. Intensive Care Med. 2015, 41, 744–762. [Google Scholar] [CrossRef] [PubMed]
- Corner, E.; Wood, H.; Englebretsen, C.; Thomas, A.; Grant, R.; Nikoletou, D.; Soni, N. The Chelsea critical care physical assessment tool (CPAx): Validation of an innovative new tool to measure physical morbidity in the general adult critical care population; an observational proof-of-concept pilot study. Physiotherapy 2013, 99, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Astrup, K.; Corner, E.; Van Tulder, M.; Sorensen, L. Reliability and responsiveness of the Danish version of The Chelsea Critical Care Physical Assessment tool (CPAx). Physiother. Theory Pract. 2021, 39, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Holdar, U.; Eriksson, F.; Siesage, K.; Corner, E.J.; Ledström, V.; Svensson-Raskh, A.; Kierkegaard, M. Cross-cultural adaptation and inter-rater reliability of the Swedish version of the Chelsea critical care assessment tool (CPAX-Swe) in critically ill patients. Disabil. Rehabil. 2021, 43, 1600–1604. [Google Scholar] [CrossRef]
- Eggmann, S.; Verra, M.L.; Stefanicki, V.; Kindler, A.; Seyler, D.; Hilfiker, R.; Schefold, J.C.; Bastiaenen, C.H.G.; Zante, B. German version of the Chelsea Critical Care Physical Assessment Tool (CPAx-GE): Translation, cross-cultural adaptation, validity, and reliability. Disabil. Rehabil. 2022, 44, 4509–4518. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, G.; Wu, Y.; Guo, J.; Ding, N.; Jiang, B.; Wei, H.; Li, B.; Yue, W.; Tian, J. Chinesisation, adaptation and validation of the Chelsea Critical Care Physical Assessment Tool in critically ill patients: A cross-sectional observational study. BMJ Open 2021, 11, e045550. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W-163–W-194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Buanes, E.A.; Kristine, R.K.; Helland, F.; Barrat-Due, A. Norsk Intensiv-OG Pandemiregister. Årsrapport for 2021 Med Plan for Forbetringstiltak 2022. Available online: https://helse-bergen.no/seksjon/intensivregister/Documents/%C3%85rsrapporter%20i%20NIR/NIPaR%20%C3%85rsrapport%202021.pdf (accessed on 23 December 2022).
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Kazis, L.E.; Anderson, J.J.; Meenan, R.F. Effect sizes for interpreting changes in health status. Med. Care 1989, 27, S178–S189. [Google Scholar] [CrossRef]
- Rosenthal, R.; Cooper, H.; Hedges, L. Parametric measures of effect size. In The Handbook of Research Synthesis; Russell Sage Foundation: New York, NY, USA, 1994; pp. 231–244. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall/CRC: Boca Raton, FL, USA, 1991. [Google Scholar]
- Corner, E.J. The responsiveness of the Chelsea Critical Care Physical Assessment tool in measuring functional recovery in the burns critical care population: An observational study. Burns 2015, 41, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Measures of agreement. Perspect. Clin. Res. 2017, 8, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Olofsen, E.; Dahan, A.; Borsboom, G.; Drummond, G. Improvements in the application and reporting of advanced Bland-Altman methods of comparison. J. Clin. Monit. Comput. 2015, 29, 127–139. [Google Scholar] [CrossRef]
- Donoghue, D.; Stokes, E.K. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. J. Rehabil. Med. 2009, 41, 343–346. [Google Scholar] [CrossRef] [Green Version]
- Corner, E.J.; Soni, N.; Handy, J.M.; Brett, S.J. Construct validity of the Chelsea critical care physical assessment tool: An observational study of recovery from critical illness. Crit. Care 2014, 18, R55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggmann, S.; Verra, M.L.; Stefanicki, V.; Kindler, A.; Schefold, J.C.; Zante, B.; Bastiaenen, C.H.G. Predictive validity of the Chelsea Critical Care Physical Assessment tool (CPAx) in critically ill, mechanically ventilated adults: A prospective clinimetric study. Disabil. Rehabil. 2022, 45, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Gilbertson, L.; Barber-Lomax, S. Power and Pinch Grip Strength Recorded Using the Hand-Held Jamar Dynamometer and B+L Hydraulic Pinch Guage: British Normative Data for Adults. Br. J. Occup. Ther. 1994, 57, 483–488. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of the Patient Population Scored with CPAx-NOR | Start of Physiotherapy n = 57 A | Discharge from ICU n = 53 B |
|---|---|---|
| Sex, n (%) | Men 34 (n = 60%) Women 23 (n = 40%) | Men 33 (n = 62%) Women 20 (n = 38%) |
| Age, yrs Mean (range) | 64 (24–84) | 64 (24–84) |
| Type of diagnosis, % (n = men/women): | ||
| Cardiovascular | 21.1 (8/4) | 20.8 (8/3) |
| Respiratory | 28.1 (11/5) | 26.4 (10/4) |
| Infection | 21.1 (7/5) | 18.9 (5/5) |
| Postoperative complications | 15.8 (3/6) | 17.0 (4/5) |
| Other * | 14.0 (5/3) | 17.0 (6/3) |
| CPAx-NOR Score | Lead Rater Mean (SD) Min-Max | Observer Rater Mean (SD) Min-Max | ICC (95%CI) | SEM | MDC |
|---|---|---|---|---|---|
| Time point A n = 57 | 9.60 (10.84) 0–50 | 9.72 (11.00) 0–50 | 0.990 (0.983–0.994) | 0.77 | 2.12 |
| Time point B n = 53 | 28.45 (13.24) 1–50 | 28.06 (13.15) 2–50 | 0.994 (0.990–0.997) | 0.72 | 2.0 |
| Time point A + B n = 110 | 0.998 (0.996–0.998) | 0.68 | 1.89 |
| CPAx-NOR Items | Start of Physiotherapy (A) n = 57 | Discharge from the ICU (B) n = 53 | ||||||
|---|---|---|---|---|---|---|---|---|
| Lead Rater Median (IQR 25–75%) | Observer Rater Median (IQR 25–75%) | Weighted Kappa Values | Absolute Agreement (%) | Lead Rater Median (IQR 25–75%) | Observer Rater Median (IQR 25–75%) | Weighted Kappa Values | Absolute Agreement (%) | |
| Respiratory function | 2 (1–4) | 2 (1–4) | 0.987 | 93.0 | 5 (4–5) | 5 (4–5) | 0.980 | 98.1 |
| Cough | 2 (1–4) | 2 (1 4) | 0.940 | 77.2 | 5 (4–5) | 5 (4–5) | 0.931 | 79.2 |
| Moving within the bed | 0 (0 1) | 0 (0 1) | 0.905 | 86.0 | 3 (2–4) | 3 (1–4) | 0.925 | 73.6 |
| Supine to sitting on the edge of the bed | 0 (0–1) | 0 (0–1) | 0.972 | 93.0 | 2 (1–4) | 2 (1 4) | 0.965 | 83.0 |
| Dynamic sitting | 0 (0–2) | 0 (0–2) | 0.957 | 87.7 | 4 (3–5) | 4 (3–5) | 0.961 | 79.2 |
| Standing balance | 0 (0–0) | 0 (0–0) | 0.959 | 94.7 | 3 (0–4) | 3 (0 4) | 0.990 | 94.3 |
| Sit to stand | 0 (0–0) | 0 (0–0) | 0.967 | 93.0 | 2 (0–3) | 2 (0–3) | 0.980 | 88.7 |
| Transferring from bed to chair | 0 (0–0) | 0 (0–0) | 0.975 | 98.2 | 2 (0–4) | 2 (0–4) | 0.992 | 96.2 |
| Stepping | 0 (0–0) | 0 (0–0) | 0.969 | 96.5 | 2 (0–4) | 2 (0–4) | 0.970 | 88.7 |
| Grip strength | 0 (0–2) | 0 (0–2) | 0.996 | 98.2 | 2 (1–3) | 2 (1–3) | 0.992 | 96.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schanke, C.M.; Brekka, A.K.; Rimehaug, S.A.; Klokkerud, M.; Andersen, T.M. Norwegian Version of the Chelsea Critical Care Physical Assessment Tool (CPAx-NOR): Translation, Face Validity, Cross-Cultural Adaptation and Inter-Rater Reliability. J. Clin. Med. 2023, 12, 5033. https://doi.org/10.3390/jcm12155033
Schanke CM, Brekka AK, Rimehaug SA, Klokkerud M, Andersen TM. Norwegian Version of the Chelsea Critical Care Physical Assessment Tool (CPAx-NOR): Translation, Face Validity, Cross-Cultural Adaptation and Inter-Rater Reliability. Journal of Clinical Medicine. 2023; 12(15):5033. https://doi.org/10.3390/jcm12155033
Chicago/Turabian StyleSchanke, Charlotte Marie, Anne Kristine Brekka, Stein Arne Rimehaug, Mari Klokkerud, and Tiina Maarit Andersen. 2023. "Norwegian Version of the Chelsea Critical Care Physical Assessment Tool (CPAx-NOR): Translation, Face Validity, Cross-Cultural Adaptation and Inter-Rater Reliability" Journal of Clinical Medicine 12, no. 15: 5033. https://doi.org/10.3390/jcm12155033