
Neurodevelopmental Outcome at Corrected Age of 2 Years among Children Born Preterm with Operative Vaginal Delivery: A Population-Based Study (LIFT Cohort)
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
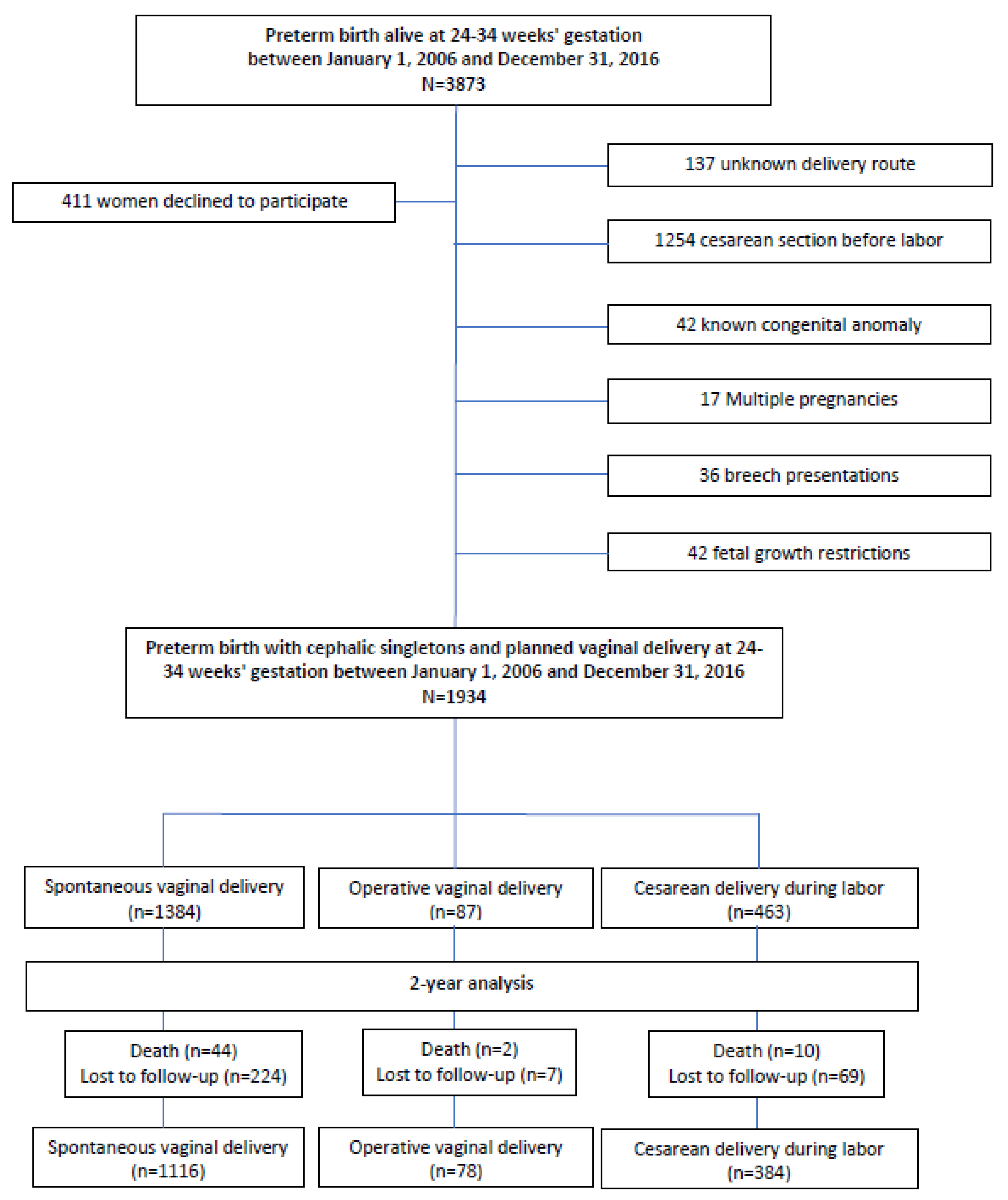
2.1. Study Design and Patients
2.2. Data Collection
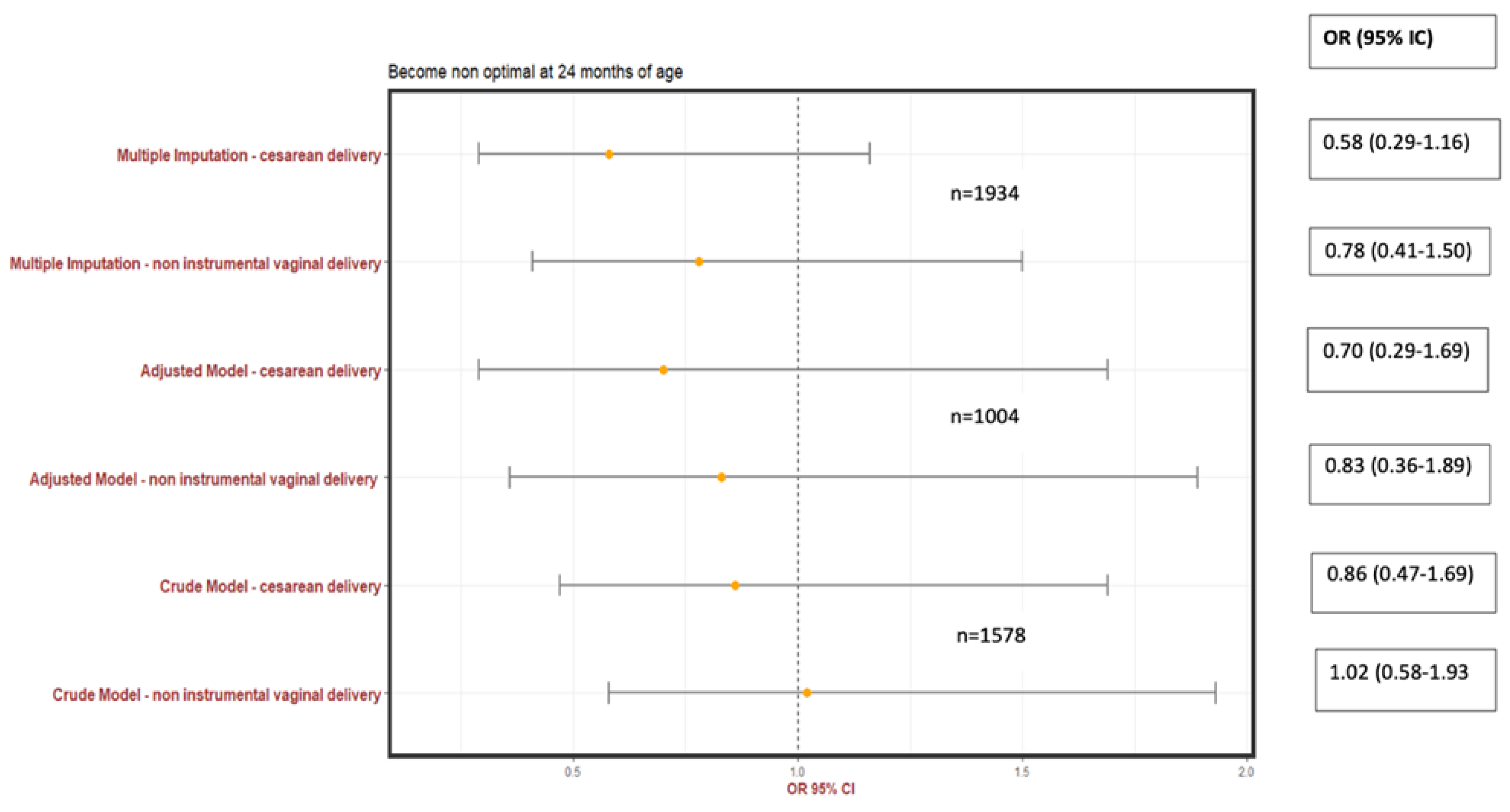
2.3. Endpoints
2.4. Exposure Variable
2.5. Adjustment Variables
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar]
- Lumley, J.; Lester, A.; Renou, P.; Wood, C. A failed RCT to determine the best method of delivery for very low birth weight infants. Control. Clin. Trials 1985, 6, 120–127. [Google Scholar] [CrossRef]
- Durie, D.; Sciscione, A.C.; Hoffman, M.K.; Mackley, A.B.; Paul, D. Mode of Delivery and Outcomes in Very Low-Birth-Weight Infants in the Vertex Presentation. Am. J. Perinatol. 2010, 28, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Åberg, K.; Norman, M.; Ekéus, C. Preterm birth by vacuum extraction and neonatal outcome: A population-based cohort study. BMC Pregnancy Childbirth 2014, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Schwarzman, P.; Sheiner, E.; Wainstock, T.; Mastrolia, S.A.; Segal, I.; Landau, D.; Walfisch, A. Vacuum Extraction in Preterm Deliveries and Long-Term Neurological Outcome of the Offspring. Pediatr. Neurol. 2019, 94, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Gaudineau, A.; Lorthe, E.; Quere, M.; Goffinet, F.; Langer, B.; Le Ray, I.; Subtil, D. Planned delivery route and outcomes of cephalic singletons born spontaneously at 24–31 weeks’ gestation: The EPIPAGE-2 cohort study. Acta Obstet. Gynecol. Scand. 2020, 99, 1682–1690. [Google Scholar]
- Spong, C.Y.; Berghella, V.; Wenstrom, K.D.; Mercer, B.M.; Saade, G.R. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Obstet. Gynecol. 2012, 120, 1181–1193. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Sénat, M.-V.; Ancel, P.-Y.; Azria, E.; Benoist, G.; Blanc, J.; Brabant, G.; Bretelle, F.; Brun, S.; Doret, M.; et al. Prevention of spontaneous preterm birth: Guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF). Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 210, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Hanf, M.; Nusinovici, S.; Rouger, V.; Olivier, M.; Berlie, I.; Flamant, C.; Gascoin, G.; Van Bogaert, P.; Rozé, J.-C. Cohort Profile: Longitudinal study of preterm infants in the Pays de la Loire region of France (LIFT cohort). Int. J. Epidemiol. 2017, 46, 1396–1397. [Google Scholar] [CrossRef]
- Squires, J.; Bricker, D.; Potter, L. Revision of a parent-completed development screening tool: Ages and Stages Questionnaires. J. Pediatr. Psychol. 1997, 22, 313–328. [Google Scholar] [CrossRef]
- Flamant, C.; Branger, B.; Tich, S.N.T.; de La Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-Completed Developmental Screening in Premature Children: A Valid Tool for Follow-Up Programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef]
- Bruel, A.; Rozé, J.-C.; Flamant, C.; Simeoni, U.; Roussey-Kesler, G.; Allain-Launay, E. Critical Serum Creatinine Values in Very Preterm Newborns. PLoS ONE 2013, 8, e84892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouin, M.; Nguyen, S.; Savagner, C.; Troussier, F.; Gascouin, G.; Rozé, J.-C.; Flamant, C. Severe bronchiolitis in infants born very preterm and neurodevelopmental outcome at 2 years. Eur. J. Pediatr. 2013, 172, 639–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younge, N.; Goldstein, R.F.; Bann, C.M.; Hintz, S.R.; Patel, R.M.; Smith, P.B.; Bell, E.F.; Rysavy, M.A.; Duncan, A.F.; Vohr, B.R.; et al. Survival and Neurodevelopmental Outcomes among Periviable Infants. N. Engl. J. Med. 2017, 376, 617–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahedi-Spung, L.D.; Raghuraman, N.; Macones, G.A.; Cahill, A.G.; Rosenbloom, J.I. Neonatal morbidity and mortality by mode of delivery in very preterm neonates. Am. J. Obstet. Gynecol. 2022, 226, 114.e1–114.e7. [Google Scholar] [CrossRef]
- Pierrat, V.; Marchand-Martin, L.; Arnaud, C.; Kaminski, M.; Resche-Rigon, M.; Lebeaux, C.; Bodeau-Livinec, F.; Morgan, A.S.; Goffinet, F.; Marret, S.; et al. Neurodevelopmental outcome at 2 years for preterm children born at 22 to 34 weeks’ gestation in France in 2011: EPIPAGE-2 cohort study. BMJ 2017, 358, j3448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leroux, B.G.; Tich, S.N.T.; Branger, B.; Gascoin, G.; Rouger, V.; Berlie, I.; Montcho, Y.; Ancel, P.-Y.; Rozé, J.-C.; Flamant, C. Neurological assessment of preterm infants for predicting neuromotor status at 2 years: Results from the LIFT cohort. BMJ Open 2013, 3, e002431. [Google Scholar] [CrossRef] [Green Version]
- Grant, A.; Glazener, C.M. Elective caesarean section versus expectant management for delivery of the small baby. Cochrane Database Syst. Rev. 2001, 2, CD000078. [Google Scholar]
- Schonhaut, L.; Armijo, I.; Schönstedt, M.; Alvarez, J.; Cordero, M. Validity of the Ages and Stages Questionnaires in Term and Preterm Infants. Pediatrics 2013, 131, e1468–e1474. [Google Scholar] [CrossRef] [Green Version]
- Steenis, L.J.P.; Verhoeven, M.; Hessen, D.J.; van Baar, A.L. Parental and professional assessment of early child development: The ASQ-3 and the Bayley-III-NL. Early Hum. Dev. 2015, 91, 217–225. [Google Scholar] [CrossRef]
- Kerstjens, J.M.; Nijhuis, A.; Hulzebos, C.V.; Van Imhoff, D.E.; van Wassenaer-Leemhuis, A.G.; Van Haastert, I.C.; Lopriore, E.; Katgert, T.; Swarte, R.M.; van Lingen, R.A.; et al. The Ages and Stages Questionnaire and Neurodevelopmental Impairment in Two-Year-Old Preterm-Born Children. PLoS ONE 2015, 10, e0133087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolke, D.; Söhne, B.; Ohrt, B.; Riegel, K. Follow-up of preterm children: Important to document dropouts. Lancet 1995, 345, 447. [Google Scholar] [CrossRef] [PubMed]
- Sices, L.; Stancin, T.; Kirchner, H.L.; Bauchner, H. PEDS and ASQ Developmental Screening Tests May Not Identify the Same Children. Pediatrics 2009, 124, e640–e647. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Spontaneous Vaginal Delivery n = 1384 | Operative Vaginal Delivery n = 87 | Cesarean Section during Labor n = 463 | p Value a | |
|---|---|---|---|---|
| Age, y | 29.5 ± 5.5 | 30.6 ± 4.8 | 30.7 ± 5.2 | 0.50 |
| Missing data | 56.7% | 43.7% | 74.5% | |
| BMI before pregnancy, kg/m2 | 23.3 ± 1.1 | 23.7 ± 0.6 | 23.7 ± 0.9 | 0.37 |
| Missing data | 87.4% | 76% | 93% | |
| Tobacco use | 47 (23.3) | 2 (14.3) | 18 (24.0) | 0.72 |
| Missing data | 85.4% | 83.9% | 83.8% | |
| ART | 44 (8.8) | 5 (14.7) | 19 (12.6) | 0.24 |
| Missing data | 73.7% | 60.9% | 67.4% | |
| Chronic hypertension | 35 (13.5) | 3 (13.6) | 50 (61.7) | <0.001 |
| Missing data | 81.3% | 74.7% | 82.5% | |
| Preexisting type 1 or 2 diabetes | 1 (0.4) | 3 (14.3) | 0 | <0.001 |
| Missing data | 83% | 76% | 93% | |
| Maternal socioeconomic status | 0.20 | |||
| Low | 102 (12.9) | 2 (3.4) | 32 (12.3) | |
| Intermediate | 574 (72.5) | 47 (79.7) | 197 (75.8) | |
| High | 116 (14.6) | 10 (16.9) | 31 (11.9) | |
| Missing data | 42.8% | 32.2% | 32.3% | |
| Paternal socioeconomic status | 0.32 | |||
| Low | 102 (12.7) | 2 (3.4) | 32 (11.8) | |
| Intermediate | 560 (69.7) | 45 (76.3) | 193 (71.2) | |
| High | 141 (17.6) | 12 (20.3) | 46 (17.0) | |
| Missing data | 42.0% | 32.2% | 29.4% | |
| Threatened preterm birth | 980 (70.8) | 57 (65.5) | 248 (53.6) | 0.11 |
| Gestational diabetes mellitus | 16 (1.2) | 4 (4.6) | 3 (0.6) | 0.99 |
| Corticosteroid treatment | 796 (57.5) | 53 (60.9) | 256 (55.3) | 0.54 |
| Magnesium sulfate | 49 (3.5) | 4 (4.6) | 11 (2.4) | 0.38 |
| IOL | 44 (3.2) | 1 (1.1) | 19 (4.1) | 0.32 |
| Spontaneous Vaginal Delivery n = 1384 | Operative Vaginal Delivery n = 87 | Cesarean Section During Labor n = 463 | p Value a | |
|---|---|---|---|---|
| Gestational age at birth, weeks | 30.6 ± 2.5 | 31.7 ± 1.9 | 30.6 ± 2.3 | 0.001 |
| 25–27 WG | 189 (13.7) | 3 (3.4) | 49 (10.6) | |
| 28–31 WG | 448 (32.4) | 22 (25.3) | 187 (40.4) | |
| 32–34 WG | 747 (54.0) | 62 (71.3) | 227 (49.0) | |
| Level of neonatal care | 0.03 | |||
| Maternity with NICU | 1292 (93.5) | 83 (95.4) | 449 (97.0) | |
| Maternity without NICU | 59 (4.3) | 4 (4.6) | 13 (2.8) | |
| Delivery at home | 28 (2.0) | 0 | 0 | |
| Missing data | 0.4% | 0 | 0.2% | |
| PPROM > 24 h | 348 (25.1) | 20 (23.0) | 100 (21.6) | 0.29 |
| Chorioamnionitis | 76 (5.5) | 3 (3.4) | 30 (6.5) | 0.48 |
| Birth weight, g | 1653 ± 481 | 1807 ± 395 | 1564 ± 445 | <0.001 |
| Z-score of birth weight | 0.29 ± 0.80 | 0.14 ± 0.73 | 0.02 ± 0.86 | <0.001 |
| <−1 SD | 47 (3.4) | 5 (5.7) | 47 (10.2) | |
| Between −1 SD and 0 SD | 451 (32.7) | 28 (32.2) | 184 (39.7) | |
| Between 0 and +1 SD | 658 (47.7) | 44 (50.6) | 183 (39.5) | |
| >+1 SD | 223 (16.2) | 10 (11.5) | 49 (10.6) | |
| Male | 793 (57.3) | 61 (70.1) | 272 (58.7) | 0.06 |
| Height at birth, cm | 40.0 ± 1.1 | 42.0 ± 0.8 | 39.6 ± 1.8 | 0.15 |
| Head circumference at birth, cm | 28.3 ± 2.1 | 29.4 ± 1.8 | 28.3 ± 2.2 | 0.22 |
| Apgar score < 7 at 5 min | 104 (7.5) | 4 (4.6) | 61 (13.2) | <0.001 |
| Neonatal procedures in delivery room | 960 (69.4) | 20 (23.0) | 85 (18.4) | <0.001 |
| Mask ventilation | 512 (39.4) | 50 (61.0) | 190 (45.1) | |
| Intubation | 38 (22.9) | 11 (13.4) | 127 (30.2) | |
| External cardiac massage | 324 (5.0) | 1 (1.2) | 19 (4.5) | |
| Intraventricular hemorrhage ≥ grade 3 | 31 (2.2) | 2 (2.3) | 14 (3.0) | 0.64 |
| Periventricular leukomalacia | 36 (2.6) | 3 (3.4) | 13 (2.8) | 0.88 |
| Bronchopulmonary dysplasia | 56 (4.1) | 2 (2.3) | 15 (3.2) | 0.56 |
| Need closure of ductus arteriosus | 174 (12.6) | 9 (10.3) | 52 (11.2) | 0.65 |
| Necrotizing enterocolitis | 16 (1.2) | 1 (1.1) | 6 (1.3) | 0.97 |
| Neonatal morbidity b | 237 (17.2) | 12 (13.8) | 80 (17.3) | 0.71 |
| Neonatal death | 44 (3.2) | 2 (2.3) | 10 (2.2) | 0.79 |
| Spontaneous Vaginal Delivery n = 1384 | Operative Vaginal Delivery n = 87 | Cesarean Section During Labor n = 463 | p Value a | |
|---|---|---|---|---|
| Pediatric death (<2 years) | 3 (0.2) | 0 | 0 | - |
| Loss of follow-up | 224 (16.2) | 7 (8.0) | 69 (14.9) | 0.05 |
| At 2 years of corrected age | n = 1116 (80.6) | n = 78 (89.7) | n = 384 (82.9) | |
| Height, cm | 87.5 ± 3.8 | 87.5 ± 4.0 | 87.3 ± 5.3 | |
| Weight, kg | 12.1 ± 1.6 | 12.2 ± 1.3 | 12.1 ± 2.5 | |
| Head circumference, cm | 48.8 ± 1.8 | 49.4 ± 1.8 | 48.7 ± 1.7 | |
| Non-optimal clinical examination | 188 (16.8) | 13 (16.7) | 56 (14.6) | 0.51 |
| Missing data | 2.8% | 2.6% | 2.3% | |
| ASQ score | 244.7 ± 38.4 | 246.1 ± 31.9 | 242.4 ± 36.3 | 0.58 |
| Non-optimal ASQ score (<185) | 54 (5.7) | 7 (2.9) | 19 (5.8) | 0.61 |
| Missing data | 14.9% | 15.1% | 15.1% | |
| Primary outcome b | 204 (18.3) | 14 (18.0) | 61 (15.9) | 0.57 |
| Non-Optimal Neurocognitive Development a n = 279 | Optimal Neurocognitive Development n = 1299 | p Value b | |
|---|---|---|---|
| Chronic hypertension | 14 (5.0) | 63 (4.8) | 1.0 |
| Maternal socioeconomic status | 0.004 | ||
| Low | 32 (19.3) | 94 (10.3) | |
| Intermediate | 114 (68.7) | 690 (75.2) | |
| High | 20 (12.0) | 133 (14.5) | |
| Missing data | 40.5% | 29.4% | |
| PPROM > 24 h | 51 (18.3) | 326 (25.1) | 0.02 |
| Missing data | 1.1% | 4.0% | |
| Chorioamnionitis | 16 (5.8) | 65 (5.0) | 0.72 |
| Missing data | 1.1% | 0.2% | |
| Magnesium sulfate treatment | 11 (3.9) | 38 (2.9) | 0.48 |
| Missing data | 4.7% | 3.5% | |
| Corticosteroid treatment | 155 (55.6) | 739 (56.9) | 0.73 |
| Missing data | 0.7% | 0.4% | |
| IOL | 9 (3.2) | 45 (3.5) | 0.99 |
| Missing data | 0.4% | 2.0% | |
| Gestational age at birth, weeks | 29.7 (2.7) | 30.9 (2.3) | <0.001 |
| 25–27 WG | 62 (22.2) | 113 (8.7) | <0.001 |
| 28–31 WG | 117 (41.9) | 438 (33.7) | |
| 32–34 WG | 100 (35.9) | 748 (57.6) | |
| Mode of delivery | 0.57 | ||
| Spontaneous vaginal delivery | 204 (73.1) | 912 (70.2) | |
| Operative vaginal delivery | 14 (5.0) | 64 (4.9) | |
| Cesarean section during labor | 61 (21.9) | 323 (24.9) | |
| Birth weight, g | 1475 ± 489 | 1685 ± 447 | <0.001 |
| Z-score of birth weight | 0.20 ± 0.8 | 0.23 ± 0.8 | 0.61 |
| <−1 SD | 15 (5.4) | 66 (5.1) | |
| Between −1 SD and 0 SD | 97 (34.9) | 436 (33.6) | |
| Between 0 and +1 SD | 127 (45.7) | 605 (46.6) | |
| >+1 SD | 39 (14.0) | 190 (14.6) | |
| Level of neonatal care | |||
| Maternity with NICU | 259 (92.8) | 1237 (95.2) | 0.29 |
| Maternity without NICU | 14 (5.0) | 49 (3.8) | |
| Delivery at home | 6 (2.2) | 13 (1.0) | |
| Apgar score < 7 at 5 min | 38 (13.6) | 87 (6.7) | <0.001 |
| Neonatal procedures in delivery room | <0.001 | ||
| Mask ventilation | 90 (35.4) | 542 (45.1) | |
| Intubation | 93 (36.6) | 262 (21.8) | |
| External cardiac massage | 14 (5.5) | 27 (2.2) | |
| Need closure of ductus arteriosus | 65 (23.3) | 112 (8.6) | <0.001 |
| Missing data | 0 | 0 | |
| Bronchopulmonary dysplasia | 19 (6.8) | 37 (2.9) | 0.002 |
| Missing data | 0.4% | 0.2% | |
| Intraventricular hemorrhage ≥ grade 3 | 6 (2.2) | 13 (1.0) | 0.19 |
| Missing data | 0 | 0 | |
| Periventricular leukomalacia | 27 (9.7) | 13 (1.0) | <0.001 |
| Missing data | 0 | 0 | |
| Necrotizing enterocolitis | 6 (2.2) | 12 (0.9) | 0.15 |
| Missing data | 0 | 0 | |
| Neonatal morbidity c | 91 (32.7) | 157 (12.1) | <0.001 |
| Missing data | 0.4% | 0.1% |
| Variable | Crude OR (95% CI) | p-Value | Adj. OR (95% CI) | p-Value | Imp. OR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Male | 1.18 (0.90–1.54) | 0.23 | ||||
| Gestational age at birth | 0.82 (0.78–0.87) | <0.001 | - | - | ||
| ≤27 WG | 4.10 (2.82–5.96) | <0.001 | 1.28 (0.50–3.25) | 0.60 | ||
| 28–31 WG | 2.00 (1.49–2.68) | <0.001 | 1.33 (0.75–2.37) | 0.33 | ||
| 32–34 WG | 1.00 | - | 1.00 | - | ||
| Birth weight | 1.00 (1.00–1.00) | <0.001 | 1.00 (0.99–1.00) | 0.45 | ||
| Z-score of birth weight (SD) | ||||||
| <−1 | 1.00 | - | ||||
| Between −1 and 0 | 0.98 (0.54–1.82) | 0.94 | ||||
| Between 0 and +1 | 0.92 (0.58–1.91) | 0.79 | ||||
| >+1 | 0.90 (0.56–2.10) | 0.76 | ||||
| Maternal socioeconomic status | ||||||
| Low | 1.00 | - | 1.00 | - | 1.00 | - |
| Intermediate | 0.49 (0.31–0.77) | 0.002 | 0.54 (0.34–0.88) | 0.01 | −0.68 (−3.22–0.61) | <0.01 |
| High | 0.44 (0.24–0.81) | 0.01 | 0.47 (0.24–0.92) | 0.03 | −0.79 (−2.51–0.31) | <0.01 |
| Chronic hypertension | 1.04 (0.55–1.82) | 0.91 | ||||
| PPROM > 24 h | ||||||
| No | 1.00 | - | 1.00 | - | 1.00 | - |
| Yes | 0.67 (1.07–2.08) | 0.02 | 0.64 (0.41–0.99) | 0.05 | −0.41 (0.18–2.27) | 0.02 |
| Chorioamnionitis | ||||||
| No | 1.00 | - | ||||
| Yes | 1.15 (0.64–1.98) | 0.61 | ||||
| Magnesium sulfate | ||||||
| No | 1.00 | - | ||||
| Yes | 1.36 (0.66–2.61) | 0.38 | ||||
| Corticosteroid treatment | ||||||
| No | 1.00 | - | ||||
| Yes | 0.95 (0.73–1.23) | 0.68 | ||||
| Induction of labor | ||||||
| No | 1.00 | - | ||||
| Yes | 0.93 (0.42–1.83) | 0.84 | ||||
| Level of maternity | ||||||
| Without NICU | 1.00 | - | ||||
| With NICU | 0.74 (0.41–1.42) | 0.34 | ||||
| At home | 1.62 (0.49–4.93) | 0.41 | ||||
| Apgar score < 7 at 5 min | 2.20 (1.45–3.27) | <0.001 | 1.29 (0.70–2.37) | 0.41 | ||
| Immediate neonatal procedures | ||||||
| No procedure | 1.00 | - | 1.00 | - | 1.00 | - |
| Mask ventilation | 1.08 (0.76–1.56) | 0.66 | 1.18 (0.72–1.93) | 0.50 | −0.07 (0.18–0.36) | 0.72 |
| Intubation | 2.32 (1.61–3.35) | <0.001 | 1.99 (1.12–3.54) | 0.02 | 0.79 (0.18–4.37) | <0.001 |
| External cardiac massage | 3.98 (1.64–6.75) | <0.001 | 2.43 (0.90–6.54) | 0.08 | 1.24 (0.35–3.50) | <0.001 |
| Need to close the ductus arteriosus | ||||||
| No | 1.00 | - | 1.00 | - | ||
| Yes | 3.22 (2.29–4.50) | <0.001 | 1.03 (0.34–3.06) | 0.96 | ||
| BPD | ||||||
| No | 1.00 | - | 1.00 | - | ||
| Yes | 2.50 (1.39–4.36) | 0.002 | 1.37 (0.57–3.26) | 0.48 | ||
| IVH grade III or IV | ||||||
| No | 1.00 | - | ||||
| Yes | 2.17 (0.76–5.55) | 0.12 | ||||
| PVL | ||||||
| No | 1.00 | - | 1.00 | - | 1.00 | - |
| Yes | 10.6 (5.50–21.48) | <0.001 | 5.47 (1.43–20.81) | 0.01 | 2.20 (0.35–6.35) | <0.001 |
| NEC | ||||||
| No | 1.00 | - | ||||
| Yes | 2.36 (0.81–6.13) | 0.09 | ||||
| Neonatal morbidity a | ||||||
| No | 1.00 | - | 1.00 | - | ||
| Yes | 3.54 (2.61–4.77) | <0.001 | 1.34 (0.45–3.96) | 0.59 | ||
| SVD (versus OVD) | 1.02 (0.58–1.93) | 0.94 | 0.85 (0.37–1.95) | 0.70 | −0.24 (−0.74–0.33) | 0.46 |
| CS (versus OVD) | 0.86 (0.47–1.69) | 0.65 | 0.76 (0.31–1.80) | 0.53 | −0.54 (−1.53–0.35) | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ducarme, G.; Fosse, V.; Rouger, V.; Winer, N.; Flamant, C.; Olivier, M. Neurodevelopmental Outcome at Corrected Age of 2 Years among Children Born Preterm with Operative Vaginal Delivery: A Population-Based Study (LIFT Cohort). J. Clin. Med. 2023, 12, 4970. https://doi.org/10.3390/jcm12154970
Ducarme G, Fosse V, Rouger V, Winer N, Flamant C, Olivier M. Neurodevelopmental Outcome at Corrected Age of 2 Years among Children Born Preterm with Operative Vaginal Delivery: A Population-Based Study (LIFT Cohort). Journal of Clinical Medicine. 2023; 12(15):4970. https://doi.org/10.3390/jcm12154970
Chicago/Turabian StyleDucarme, Guillaume, Victoria Fosse, Valérie Rouger, Norbert Winer, Cyril Flamant, and Marion Olivier. 2023. "Neurodevelopmental Outcome at Corrected Age of 2 Years among Children Born Preterm with Operative Vaginal Delivery: A Population-Based Study (LIFT Cohort)" Journal of Clinical Medicine 12, no. 15: 4970. https://doi.org/10.3390/jcm12154970