
Current Therapies in Kidney Transplant Rejection
Abstract
:1. Introduction
2. T-Cell-Mediated Rejection (TCMR)
2.1. Diagnosis
2.2. Current Therapies
2.2.1. Corticosteroids
2.2.2. T-Cell-Depleting Agents
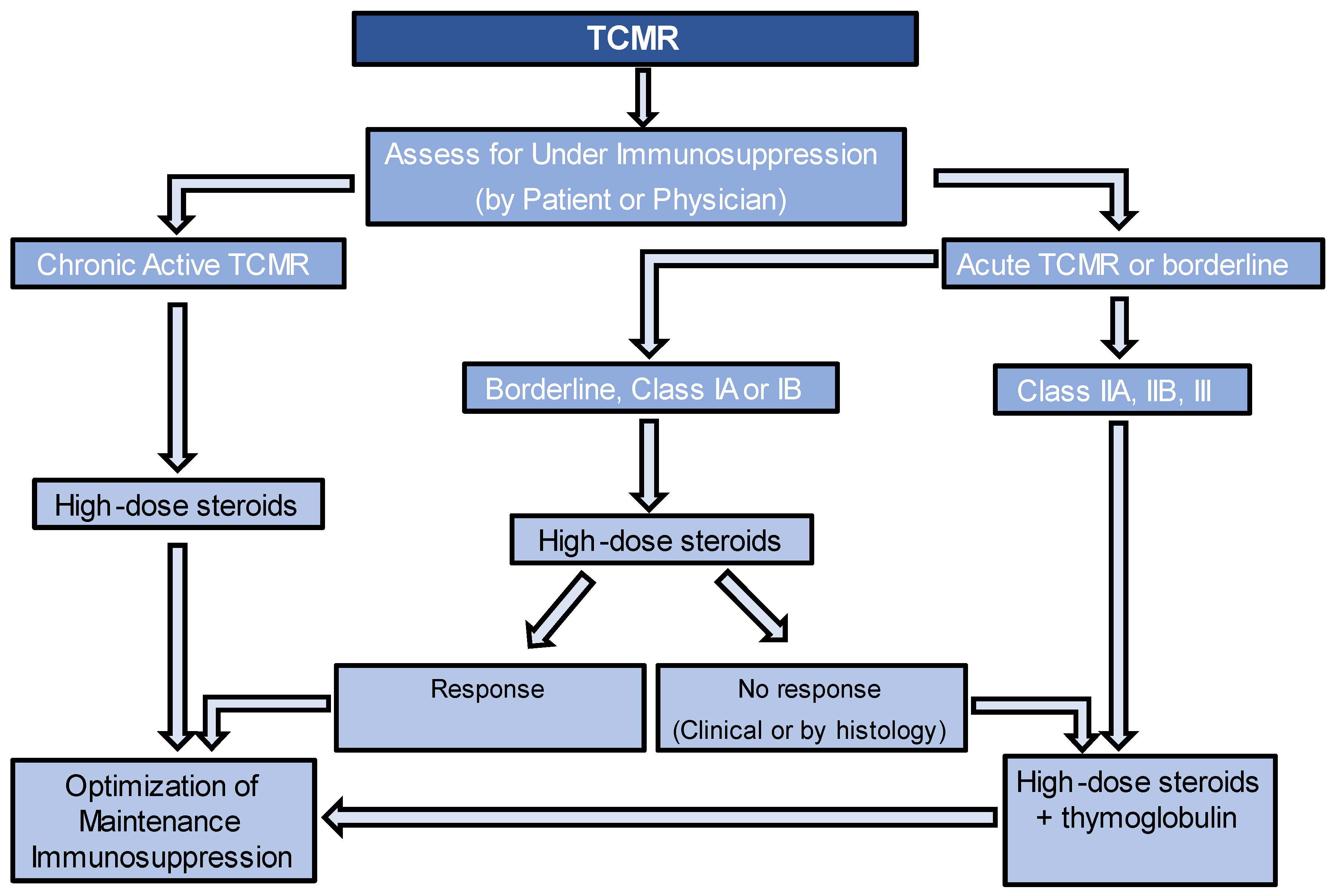
2.3. Approach to Treatment
3. Borderline Changes
4. Antibody-Mediated Rejection (ABMR)
4.1. Diagnosis
4.2. Current Therapies
4.2.1. Plasmapheresis
4.2.2. Immunoadsorption
4.2.3. Intravenous Immunoglobulin (IVIG)
4.2.4. Anti-CD20 Monoclonal Antibody
4.2.5. Complement Inhibitors
4.2.6. Proteasome Inhibitors
4.2.7. Splenectomy
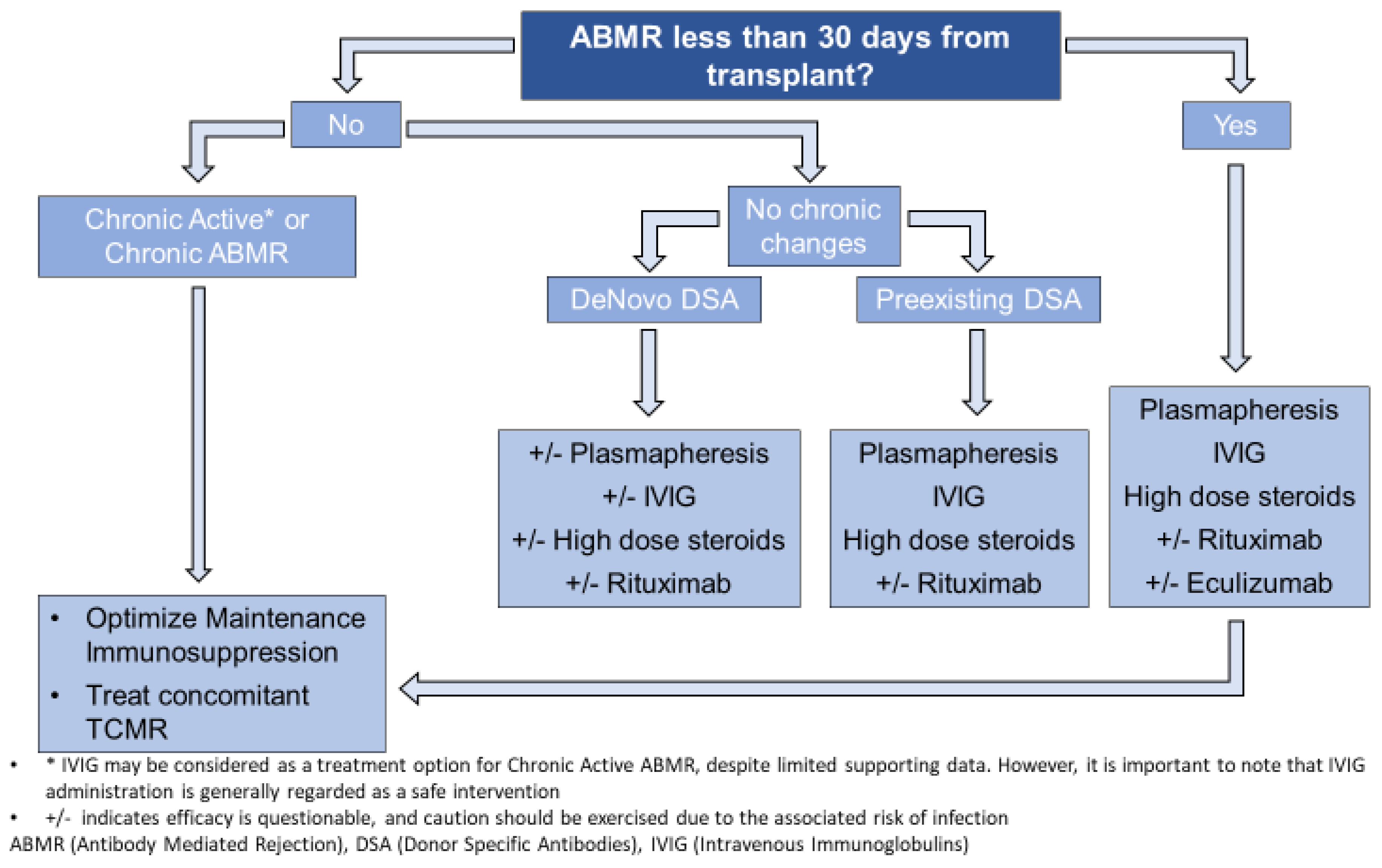
4.3. Approach to Treatment
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poggio, E.D.; Augustine, J.J.; Arrigain, S.; Brennan, D.C.; Schold, J.D. Long-term kidney transplant graft survival—Making progress when most needed. Am. J. Transpl. 2021, 21, 2824–2832. [Google Scholar] [CrossRef]
- United Network for Organ Sharing. Data Reports. Available online: https://www.unos.org/data/transplant-trends/ (accessed on 14 April 2023).
- El-Zoghby, Z.M.; Stegall, M.D.; Lager, D.J.; Kremers, W.K.; Amer, H.; Gloor, J.M.; Cosio, F.G. Identifying specific causes of kidney allograft loss. Am. J. Transpl. 2009, 9, 527–535. [Google Scholar] [CrossRef]
- Loupy, A.; Suberbielle-Boissel, C.; Hill, G.S.; Lefaucheur, C.; Anglicheau, D.; Zuber, J.; Martinez, F.; Thervet, E.; Méjean, A.; Charron, D.; et al. Outcome of subclinical antibody-mediated rejection in kidney transplant recipients with preformed donor-specific antibodies. Am. J. Transpl. 2009, 9, 2561–2570. [Google Scholar] [CrossRef] [PubMed]
- Solez, K.; Axelsen, R.A.; Benediktsson, H.; Burdick, J.F.; Cohen, A.H.; Colvin, R.B.; Croker, B.P.; Droz, D.; Dunnill, M.S.; Halloran, P.F.; et al. International standardization of criteria for the histologic diagnosis of renal allograft rejection: The Banff working classification of kidney transplant pathology. Kidney Int. 1993, 44, 411–422. [Google Scholar] [CrossRef] [Green Version]
- Loupy, A.; Haas, M.; Roufosse, C.; Naesens, M.; Adam, B.; Afrouzian, M.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Becker, J.U.; et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am. J. Transpl. 2020, 20, 2318–2331. [Google Scholar] [CrossRef]
- Wiebe, C.; Rush, D.N.; Gibson, I.W.; Pochinco, D.; Birk, P.E.; Goldberg, A.; Blydt-Hansen, T.; Karpinski, M.; Shaw, J.; Ho, J.; et al. Evidence for the alloimmune basis and prognostic significance of Borderline T cell-mediated rejection. Am. J. Transpl. 2020, 20, 2499–2508. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.C. Immunosuppressive Medications. Clin. J. Am. Soc. Nephrol. 2016, 11, 332–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, F.; Parajuli, S.; Garg, N.; Mohamed, M.; Zhong, W.; Djamali, A.; Mandelbrot, D. How Should Acute T-cell Mediated Rejection of Kidney Transplants Be Treated: Importance of Follow-up Biopsy. Transpl. Direct. 2022, 8, e1305. [Google Scholar] [CrossRef]
- Gaber, L.W.; Moore, L.W.; Alloway, R.R.; Flax, S.D.; Shokouh-Amiri, M.H.; Schroder, T.; Gaber, A.O. Correlation between Banff classification, acute renal rejection scores and reversal of rejection. Kidney Int. 1996, 49, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Lamarche, C.; Côté, J.M.; Sénécal, L.; Cardinal, H. Efficacy of Acute Cellular Rejection Treatment According to Banff Score in Kidney Transplant Recipients: A Systematic Review. Transpl. Direct. 2016, 2, e115. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes Transplant Work, G. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transpl. 2009, 9 (Suppl. S3), S1–S155. [Google Scholar] [CrossRef] [PubMed]
- Zand, M.S.; Vo, T.; Huggins, J.; Felgar, R.; Liesveld, J.; Pellegrin, T.; Bozorgzadeh, A.; Sanz, I.; Briggs, B.J. Polyclonal rabbit antithymocyte globulin triggers B-cell and plasma cell apoptosis by multiple pathways. Transplantation 2005, 79, 1507–1515. [Google Scholar] [CrossRef]
- de Castro, M.C.; Deboni, L.; Esmeraldo Rde, M.; Matuk, T.A.; Pacheco, A.; Saitovitch, D.; Salomão, A.; Silva Junior, H.T.; Villaça, S. Use of Thymoglobulin® (antithymocyte immunoglobulin) in renal transplantation: Practical guide. J. Bras. Nefrol. 2015, 37, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Chandran, S.; Mannon, R.B. T cell-mediated rejection in kidney transplant recipients: The end(point) is also the beginning. Am. J. Transpl. 2022, 22, 683–684. [Google Scholar] [CrossRef]
- Mehta, R.; Bhusal, S.; Randhawa, P.; Sood, P.; Cherukuri, A.; Wu, C.; Puttarajappa, C.; Hoffman, W.; Shah, N.; Mangiola, M.; et al. Short-term adverse effects of early subclinical allograft inflammation in kidney transplant recipients with a rapid steroid withdrawal protocol. Am. J. Transpl. 2018, 18, 1710–1717. [Google Scholar] [CrossRef] [Green Version]
- Schinstock, C.A.; Mannon, R.B.; Budde, K.; Chong, A.S.; Haas, M.; Knechtle, S.; Lefaucheur, C.; Montgomery, R.A.; Nickerson, P.; Tullius, S.G.; et al. Recommended Treatment for Antibody-mediated Rejection After Kidney Transplantation: The 2019 Expert Consensus From the Transplantion Society Working Group. Transplantation 2020, 104, 911–922. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Li, Z.; Wu, W.; Luo, G.; Xu, C.; Sun, Z.; Mei, H. Role of MICA antibodies in solid organ transplantation. Clin. Transpl. 2014, 28, 152–160. [Google Scholar] [CrossRef]
- Dragun, D.; Müller, D.N.; Bräsen, J.H.; Fritsche, L.; Nieminen-Kelhä, M.; Dechend, R.; Kintscher, U.; Rudolph, B.; Hoebeke, J.; Eckert, D.; et al. Angiotensin II type 1-receptor activating antibodies in renal-allograft rejection. N. Engl. J. Med. 2005, 352, 558–569. [Google Scholar] [CrossRef] [Green Version]
- Abuzeineh, M.; Kyeso, Y.; Philogene, M.C.; Alachkar, N.; Alasfar, S. Presentation and Outcomes of Antibody-Mediated Rejection Associated With Angiotensin II Receptor 1 Antibodies Among Kidney Transplant Recipients. Transpl. Proc. 2021, 53, 1501–1508. [Google Scholar] [CrossRef]
- Mauiyyedi, S.; Pelle, P.D.; Saidman, S.; Collins, A.B.; Pascual, M.; Tolkoff-Rubin, N.E.; Williams, W.W.; Cosimi, A.B.; Schneeberger, E.E.; Colvin, R.B. Chronic humoral rejection: Identification of antibody-mediated chronic renal allograft rejection by C4d deposits in peritubular capillaries. J. Am. Soc. Nephrol. 2001, 12, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Naesens, M.; Roufosse, C.; Colvin, R.B.; Haas, M.; Lefaucheur, C.; Mannon, R.B.; Adam, B.; Aubert, O.; Böhmig, G.A.; Callemeyn, J.; et al. The Banff 2022 Kidney Meeting Report: Re-Appraisal of Microvascular Inflammation and the Role of Biopsy-Based Transcript Diagnostics. Available online: https://ssrn.com/abstract=4447700 (accessed on 13 May 2023). [CrossRef]
- Allen, N.H.; Dyer, P.; Geoghegan, T.; Harris, K.; Lee, H.A.; Slapak, M. Plasma exchange in acute renal allograft rejection. A controlled trial. Transplantation 1983, 35, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, F.; Shinohara, Y. Lymphocyte subset proportions in Guillain-Barré syndrome patients treated with plasmapheresis. Eur. Neurol. 2000, 44, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Dau, P.C.; Callahan, J.P. Immune modulation during treatment of systemic sclerosis with plasmapheresis and immunosuppressive drugs. Clin. Immunol. Immunopathol. 1994, 70, 159–165. [Google Scholar] [CrossRef]
- De Luca, G.; Lugaresi, A.; Iarlori, C.; Marzoli, F.; Di Iorio, A.; Gambi, D.; Uncini, A. Prednisone and plasma exchange improve suppressor cell function in chronic inflammatory demyelinating polyneuropathy. J. Neuroimmunol. 1999, 95, 190–194. [Google Scholar] [CrossRef]
- Bonomini, V.; Vangelista, A.; Frascà, G.M.; Di Felice, A.; Liviano D’Arcangelo, G. Effects of plasmapheresis in renal transplant rejection. A controlled study. Trans. Am. Soc. Artif. Intern. Organs 1985, 31, 698–703. [Google Scholar]
- Rifle, G.; Chalopin, J.M.; Turc, J.M.; Guigner, F.; Vialtel, P.; Dechelette, E.; Chenais, F.; Cordonnier, D. Plasmapheresis in the treatment of renal allograft rejections. Transpl. Proc. 1979, 11, 20–26. [Google Scholar]
- Naik, R.B.; Ashlin, R.; Wilson, C.; Smith, D.S.; Lee, H.A.; Slapak, M. The role of plasmapheresis in renal transplantation. Clin. Nephrol. 1979, 11, 245–250. [Google Scholar]
- Cardella, C.J.; Sutton, D.; Uldall, P.R.; deVeber, G.A. Intensive plasma exchange and renal-transplant rejection. Lancet 1977, 1, 264. [Google Scholar] [CrossRef]
- Kirubakaran, M.G.; Disney, A.P.; Norman, J.; Pugsley, D.J.; Mathew, T.H. A controlled trial of plasmapheresis in the treatment of renal allograft rejection. Transplantation 1981, 32, 164–165. [Google Scholar] [CrossRef]
- Blake, P.; Sutton, D.; Cardella, C.J. Plasma exchange in acute renal transplant rejection. Prog. Clin. Biol. Res. 1990, 337, 249–252. [Google Scholar] [PubMed]
- Sanchez, A.P.; Cunard, R.; Ward, D.M. The selective therapeutic apheresis procedures. J. Clin. Apher. 2013, 28, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Bohmig, G.A.; Wahrmann, M.; Regele, H.; Exner, M.; Robl, B.; Derfler, K.; Soliman, T.; Bauer, P.; Mullner, M.; Druml, W. Immunoadsorption in severe C4d-positive acute kidney allograft rejection: A randomized controlled trial. Am. J. Transpl. 2007, 7, 117–121. [Google Scholar] [CrossRef]
- Caliskan, Y.; Mirioglu, S.; Dirim, A.B.; Ozluk, Y.; Yegit, O.; Aksoy, E.; Safak, S.; Guller, N.; Demir, E.; Artan, A.S.; et al. A comparison of methods of plasmapheresis for the treatment of late antibody mediated rejection in kidney transplant recipients. Ther. Apher. Dial. 2023, 27, 428–434. [Google Scholar] [CrossRef]
- Dietrich, G.; Kazatchkine, M.D. Normal immunoglobulin G (IgG) for therapeutic use (intravenous Ig) contain antiidiotypic specificities against an immunodominant, disease-associated, cross-reactive idiotype of human anti-thyroglobulin autoantibodies. J. Clin. Investig. 1990, 85, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Kazatchkine, M.D.; Dietrich, G.; Hurez, V.; Ronda, N.; Bellon, B.; Rossi, F.; Kaveri, S.V. V region-mediated selection of autoreactive repertoires by intravenous immunoglobulin (i.v.Ig). Immunol. Rev. 1994, 139, 79–107. [Google Scholar] [CrossRef]
- Lee, C.Y.; Lin, W.C.; Wu, M.S.; Yang, C.Y.; Yeh, C.C.; Tsai, M.K. Repeated cycles of high-dose intravenous immunoglobulin and plasmapheresis for treatment of late antibody-mediated rejection of renal transplants. J. Formos. Med. Assoc. 2016, 115, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Lefaucheur, C.; Nochy, D.; Andrade, J.; Verine, J.; Gautreau, C.; Charron, D.; Hill, G.S.; Glotz, D.; Suberbielle-Boissel, C. Comparison of combination Plasmapheresis/IVIg/anti-CD20 versus high-dose IVIg in the treatment of antibody-mediated rejection. Am. J. Transpl. 2009, 9, 1099–1107. [Google Scholar] [CrossRef]
- Montgomery, R.A.; Zachary, A.A.; Racusen, L.C.; Leffell, M.S.; King, K.E.; Burdick, J.; Maley, W.R.; Ratner, L.E. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refractory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients. Transplantation 2000, 70, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Thielke, J.; DeChristopher, P.J.; Sankary, H.; Oberholzer, J.; Testa, G.; Benedetti, E. Highly successful living donor kidney transplantation after conversion to negative of a previously positive flow-cytometry cross-match by pretransplant plasmapheresis. Transpl. Proc. 2005, 37, 643–644. [Google Scholar] [CrossRef] [PubMed]
- Warren, D.S.; Simpkins, C.E.; Cooper, M.; Montgomery, R.A. Modulating alloimmune responses with plasmapheresis and IVIG. Curr. Drug Targets Cardiovasc. Haematol. Disord. 2005, 5, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C.; Tyan, D.; Stablein, D.; McIntosh, M.; Rose, S.; Vo, A.; Toyoda, M.; Davis, C.; Shapiro, R.; Adey, D.; et al. Evaluation of intravenous immunoglobulin as an agent to lower allosensitization and improve transplantation in highly sensitized adult patients with end-stage renal disease: Report of the NIH IG02 trial. J. Am. Soc. Nephrol. 2004, 15, 3256–3262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buch, M.H.; Smolen, J.S.; Betteridge, N.; Breedveld, F.C.; Burmester, G.; Dörner, T.; Ferraccioli, G.; Gottenberg, J.E.; Isaacs, J.; Kvien, T.K.; et al. Updated consensus statement on the use of rituximab in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2011, 70, 909–920. [Google Scholar] [CrossRef]
- Sautenet, B.; Blancho, G.; Büchler, M.; Morelon, E.; Toupance, O.; Barrou, B.; Ducloux, D.; Chatelet, V.; Moulin, B.; Freguin, C.; et al. One-year Results of the Effects of Rituximab on Acute Antibody-Mediated Rejection in Renal Transplantation: RITUX ERAH, a Multicenter Double-blind Randomized Placebo-controlled Trial. Transplantation 2016, 100, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Moreso, F.; Crespo, M.; Ruiz, J.C.; Torres, A.; Gutierrez-Dalmau, A.; Osuna, A.; Perelló, M.; Pascual, J.; Torres, I.B.; Redondo-Pachón, D.; et al. Treatment of chronic antibody mediated rejection with intravenous immunoglobulins and rituximab: A multicenter, prospective, randomized, double-blind clinical trial. Am. J. Transpl. 2018, 18, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Becker, Y.T.; Becker, B.N.; Pirsch, J.D.; Sollinger, H.W. Rituximab as treatment for refractory kidney transplant rejection. Am. J. Transpl. 2004, 4, 996–1001. [Google Scholar] [CrossRef]
- Kaposztas, Z.; Podder, H.; Mauiyyedi, S.; Illoh, O.; Kerman, R.; Reyes, M.; Pollard, V.; Kahan, B.D. Impact of rituximab therapy for treatment of acute humoral rejection. Clin. Transpl. 2009, 23, 63–73. [Google Scholar] [CrossRef]
- Wan, S.S.; Ying, T.D.; Wyburn, K.; Roberts, D.M.; Wyld, M.; Chadban, S.J. The Treatment of Antibody-Mediated Rejection in Kidney Transplantation: An Updated Systematic Review and Meta-Analysis. Transplantation 2018, 102, 557–568. [Google Scholar] [CrossRef]
- Bhalla, A.; Alachkar, N.; Alasfar, S. Complement-Based Therapy in the Management of Antibody-Mediated Rejection. Adv. Chronic Kidney Dis. 2020, 27, 138–148. [Google Scholar] [CrossRef]
- Benamu, E.; Montoya, J.G. Infections associated with the use of eculizumab: Recommendations for prevention and prophylaxis. Curr. Opin. Infect. Dis. 2016, 29, 319–329. [Google Scholar] [CrossRef]
- Locke, J.E.; Magro, C.M.; Singer, A.L.; Segev, D.L.; Haas, M.; Hillel, A.T.; King, K.E.; Kraus, E.; Lees, L.M.; Melancon, J.K.; et al. The use of antibody to complement protein C5 for salvage treatment of severe antibody-mediated rejection. Am. J. Transpl. 2009, 9, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Biglarnia, A.R.; Nilsson, B.; Nilsson, T.; von Zur-Mühlen, B.; Wagner, M.; Berne, C.; Wanders, A.; Magnusson, A.; Tufveson, G. Prompt reversal of a severe complement activation by eculizumab in a patient undergoing intentional ABO-incompatible pancreas and kidney transplantation. Transpl. Int. 2011, 24, e61–e66. [Google Scholar] [CrossRef] [PubMed]
- Stewart, Z.A.; Collins, T.E.; Schlueter, A.J.; Raife, T.I.; Holanda, D.G.; Nair, R.; Reed, A.I.; Thomas, C.P. Case report: Eculizumab rescue of severe accelerated antibody-mediated rejection after ABO-incompatible kidney transplant. Transpl. Proc. 2012, 44, 3033–3036. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Kumar, V.; Mompoint-Williams, D.; Reed, R.D.; MacLennan, P.A.; Stegner, K.; Locke, J.E. Dosing Eculizumab for Antibody-Mediated Rejection in Kidney Transplantation: A Case Report. Transpl. Proc. 2016, 48, 3099–3105. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.K.; Bentall, A.; Dean, P.G.; Shaheen, M.F.; Stegall, M.D.; Schinstock, C.A. Use of Eculizumab for Active Antibody-mediated Rejection That Occurs Early Post-kidney Transplantation: A Consecutive Series of 15 Cases. Transplantation 2019, 103, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- Orandi, B.J.; Zachary, A.A.; Dagher, N.N.; Bagnasco, S.M.; Garonzik-Wang, J.M.; Van Arendonk, K.J.; Gupta, N.; Lonze, B.E.; Alachkar, N.; Kraus, E.S.; et al. Eculizumab and splenectomy as salvage therapy for severe antibody-mediated rejection after HLA-incompatible kidney transplantation. Transplantation 2014, 98, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.; Kirkiles-Smith, N.C.; Deng, Y.H.; Formica, R.N.; Moeckel, G.; Broecker, V.; Bow, L.; Tomlin, R.; Pober, J.S. Eculizumab Therapy for Chronic Antibody-Mediated Injury in Kidney Transplant Recipients: A Pilot Randomized Controlled Trial. Am. J. Transpl. 2017, 17, 682–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viglietti, D.; Gosset, C.; Loupy, A.; Deville, L.; Verine, J.; Zeevi, A.; Glotz, D.; Lefaucheur, C. C1 Inhibitor in Acute Antibody-Mediated Rejection Nonresponsive to Conventional Therapy in Kidney Transplant Recipients: A Pilot Study. Am. J. Transpl. 2016, 16, 1596–1603. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, R.A.; Orandi, B.J.; Racusen, L.; Jackson, A.M.; Garonzik-Wang, J.M.; Shah, T.; Woodle, E.S.; Sommerer, C.; Fitts, D.; Rockich, K.; et al. Plasma-Derived C1 Esterase Inhibitor for Acute Antibody-Mediated Rejection Following Kidney Transplantation: Results of a Randomized Double-Blind Placebo-Controlled Pilot Study. Am. J. Transpl. 2016, 16, 3468–3478. [Google Scholar] [CrossRef] [Green Version]
- Perry, D.K.; Burns, J.M.; Pollinger, H.S.; Amiot, B.P.; Gloor, J.M.; Gores, G.J.; Stegall, M.D. Proteasome inhibition causes apoptosis of normal human plasma cells preventing alloantibody production. Am. J. Transpl. 2009, 9, 201–209. [Google Scholar] [CrossRef]
- Walsh, R.C.; Everly, J.J.; Brailey, P.; Rike, A.H.; Arend, L.J.; Mogilishetty, G.; Govil, A.; Roy-Chaudhury, P.; Alloway, R.R.; Woodle, E.S. Proteasome inhibitor-based primary therapy for antibody-mediated renal allograft rejection. Transplantation 2010, 89, 277–284. [Google Scholar] [CrossRef]
- Cengiz Seval, G.; Beksac, M. The safety of bortezomib for the treatment of multiple myeloma. Expert. Opin. Drug Saf. 2018, 17, 953–962. [Google Scholar] [CrossRef]
- Nigos, J.G.; Arora, S.; Nath, P.; Hussain, S.M.; Marcus, R.J.; Ko, T.Y.; Sureshkumar, K.K. Treatment of antibody-mediated rejection in kidney transplant recipients: A single-center experience with a bortezomib-based regimen. Exp. Clin. Transpl. 2012, 10, 609–613. [Google Scholar] [CrossRef] [Green Version]
- Everly, M.J.; Everly, J.J.; Susskind, B.; Brailey, P.; Arend, L.J.; Alloway, R.R.; Roy-Chaudhury, P.; Govil, A.; Mogilishetty, G.; Rike, A.H.; et al. Bortezomib provides effective therapy for antibody- and cell-mediated acute rejection. Transplantation 2008, 86, 1754–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, R.C.; Brailey, P.; Girnita, A.; Alloway, R.R.; Shields, A.R.; Wall, G.E.; Sadaka, B.H.; Cardi, M.; Tevar, A.; Govil, A.; et al. Early and late acute antibody-mediated rejection differ immunologically and in response to proteasome inhibition. Transplantation 2011, 91, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Flechner, S.M.; Fatica, R.; Askar, M.; Stephany, B.R.; Poggio, E.; Koo, A.; Banning, S.; Chiesa-Vottero, A.; Srinivas, T. The role of proteasome inhibition with bortezomib in the treatment of antibody-mediated rejection after kidney-only or kidney-combined organ transplantation. Transplantation 2010, 90, 1486–1492. [Google Scholar] [CrossRef] [PubMed]
- Eskandary, F.; Regele, H.; Baumann, L.; Bond, G.; Kozakowski, N.; Wahrmann, M.; Hidalgo, L.G.; Haslacher, H.; Kaltenecker, C.C.; Aretin, M.B.; et al. A Randomized Trial of Bortezomib in Late Antibody-Mediated Kidney Transplant Rejection. J. Am. Soc. Nephrol. 2018, 29, 591–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, B.; Gangemi, A.; Thielke, J.; Oberholzer, J.; Sankary, H.; Benedetti, E. Successful rescue of refractory, severe antibody mediated rejection with splenectomy. Transplantation 2007, 83, 99–100. [Google Scholar] [CrossRef]
- Locke, J.E.; Zachary, A.A.; Haas, M.; Melancon, J.K.; Warren, D.S.; Simpkins, C.E.; Segev, D.L.; Montgomery, R.A. The utility of splenectomy as rescue treatment for severe acute antibody mediated rejection. Am. J. Transpl. 2007, 7, 842–846. [Google Scholar] [CrossRef]
- Sellarés, J.; de Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am. J. Transpl. 2012, 12, 388–399. [Google Scholar] [CrossRef]
- Djamali, A.; Kaufman, D.B.; Ellis, T.M.; Zhong, W.; Matas, A.; Samaniego, M. Diagnosis and management of antibody-mediated rejection: Current status and novel approaches. Am. J. Transpl. 2014, 14, 255–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Class/Grade of Rejection | Minimal Pathological Findings Required for Diagnosis | |
|---|---|---|
| aTCMR α | Grade IA | t2 + (i2 or i3) |
| Grade IB | t3 + (i2 or i3) | |
| Grade IIA | v1 with or without interstitial inflammation and/or tubulitis | |
| Grade IIB | v2 with or without interstitial inflammation and/or tubulitis | |
| Grade III | v3 with or without interstitial inflammation and/or tubulitis | |
| caTCMR β | Grade IA | interstitial inflammation that affects more than 25% of sclerotic cortical parenchyma and more than 25% of the total cortical parenchyma (ti2 or ti3) with t2 |
| Grade IB | interstitial inflammation that affects more than 25% of sclerotic cortical parenchyma AND more than 25% of the total cortical parenchyma (ti2 or ti3) AND t3 | |
| Grade II | Chronic allograft arteriopathy (arterial intimal fibrosis with mononuclear cell inflammation in fibrosis and formation of neointima) | |
| Borderline Changes | i1, with t1, t2, or t3 or t1 with i2 or i3 | |
| Criteria 1 | Histologic evidence of acute tissue injury, including 1 or more of the following:
|
| Criteria 2 | Evidence of current/recent antibody interaction with vascular endothelium, including 1 or more of the following:
|
| Criteria 3 | Serologic evidence of circulating donor-specific antibodies (DSA to HLA or other antigens); C4d staining or expression of validated transcripts/classifiers as noted above in criterion 2 may substitute for DSA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alasfar, S.; Kodali, L.; Schinstock, C.A. Current Therapies in Kidney Transplant Rejection. J. Clin. Med. 2023, 12, 4927. https://doi.org/10.3390/jcm12154927
Alasfar S, Kodali L, Schinstock CA. Current Therapies in Kidney Transplant Rejection. Journal of Clinical Medicine. 2023; 12(15):4927. https://doi.org/10.3390/jcm12154927
Chicago/Turabian StyleAlasfar, Sami, Lavanya Kodali, and Carrie A. Schinstock. 2023. "Current Therapies in Kidney Transplant Rejection" Journal of Clinical Medicine 12, no. 15: 4927. https://doi.org/10.3390/jcm12154927