
Effects of Virtual Reality in the Rehabilitation of Parkinson’s Disease: A Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
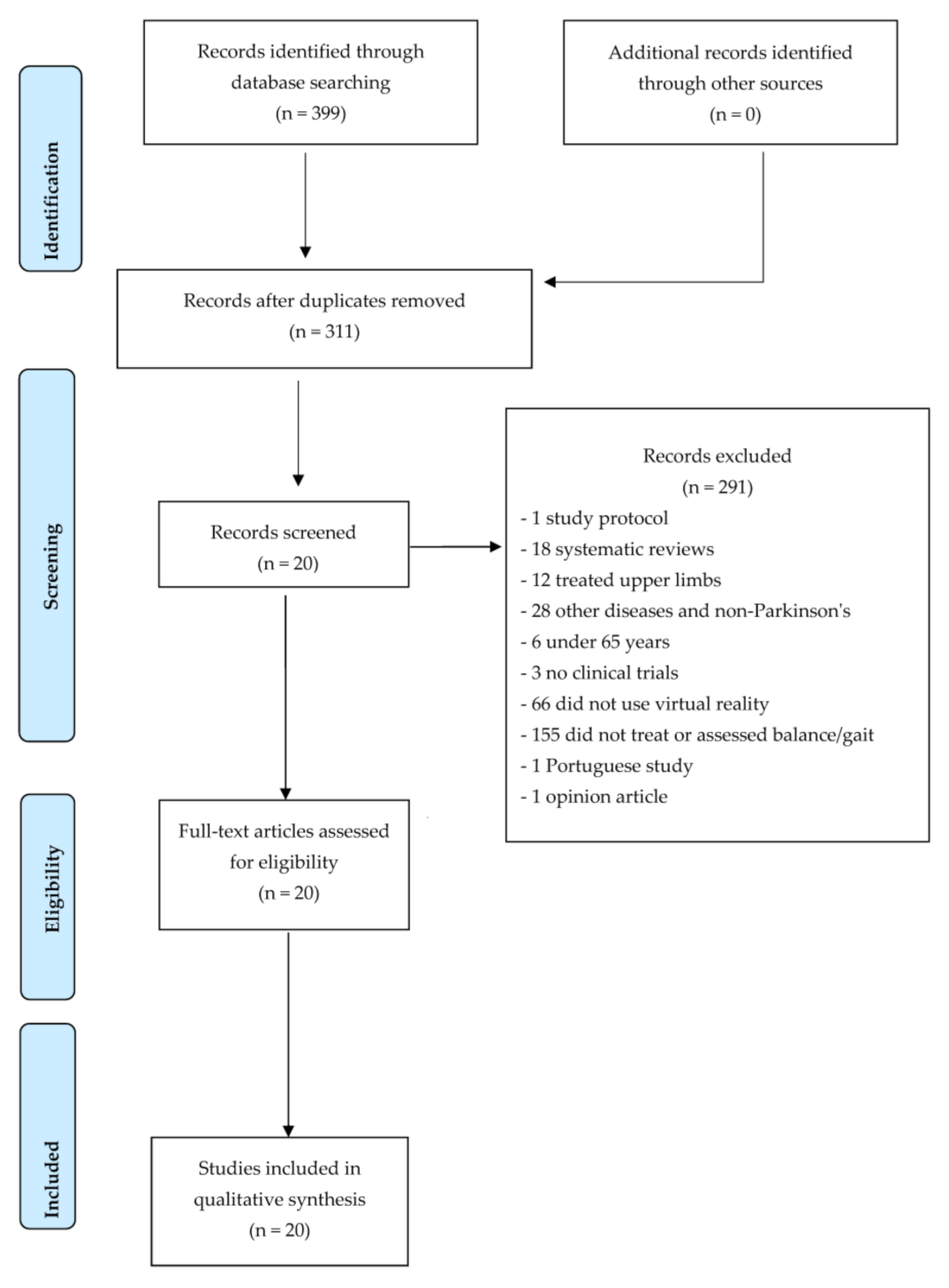
2.4. Study Selection
2.5. Assessment of Methodological Quality
2.6. Risk of Bias Analysis
3. Results
4. Discussion
5. Limitations of the Study and Further Research
6. Implications of the Use of Virtual Reality in Clinical Practice
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balestrino, R.; Schapira, A.H.V. Parkinson disease. Eur. J. Neurol. 2020, 27, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jin, M.; Wang, L.; Qin, B.; Wang, K. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Micheli, F.; Fernández Pardal, M. Neurología. In Neurología, 2nd ed.; Editorial Médica Panamericana: Buenos Aires, Argentina, 2011; p. 555. [Google Scholar]
- Chouza, M.; Raposo, I.; Fernández, R.; González, L.; Martínez, A.; Fernández, M.A. Protocolo de Fisioterapia en el paciente parkinsoniano. Fisioterapia 2001, 23, 191–199. [Google Scholar] [CrossRef]
- Moreno, C.L.; Cleves, C.C. Acta Neurológica colombiana Consenso de la asociación Colombiana de neurología sobre enfermedad de Parkinson. Acta Neurol. Colomb. 2019, 35, 19–27. [Google Scholar] [CrossRef]
- Kulisevsky, J. Enfermedad de Parkinson: Guía Terapéutica de la Sociedad Catalana de Neurología. Available online: https://docplayer.es/7259662-Guia-terapeutica-de-la-sociedad-catalana-de-neurologia.html (accessed on 15 May 2021).
- Tunur, T.; DeBlois, A.; Yates, E.; Rickford, K.; Columna, L.A. Augmented reality-based dance intervention for individuals with Parkinson’s disease: A pilot study. Disabil. Health J. 2020, 13, 100848. [Google Scholar] [CrossRef]
- Earhart, G.M.; Dibble, L.E.; Ellis, T.; Nieuwboer, A. Rehabilitation and Parkinson’s disease. Parkinsons Dis. 2012, 2012, 371406. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Herd, C.P.; Clarke, C.E.; Meek, C.; Patel, S.; Stowe, R.; Deane, K.H.; Shah, L.; Sackley, C.M.; Wheatley, K.; et al. Physiotherapy for parkinson’s disease: A comparison of techniques. Cochrane Database Syst. Rev. 2014, 2014, CD002815. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.; Deane, K.H.; Wheatley, K.; et al. Physiotherapy intervention in Parkinson’s disease: Systematic review and meta-analysis. BMJ 2012, 345, e5004. [Google Scholar] [CrossRef] [Green Version]
- Morales, S.; Elizagaray, I.; Yepes, Ó.; de la Puente, L.; Gil, A. Effectiveness of virtual immersion programmes in patients with parkinson’s disease. A Syst. Rev. Rev. Neurol. 2018, 66, 69–80. [Google Scholar]
- Viñas, S.; Sobrido, M. Realidad virtual con fines terapéuticos en pacientes con ictus: Revisión sistemática. Neurologia 2016, 31, 255–277. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.Y.; Lin, K.H.; Hu, M.H.; Wu, R.M.; Lu, T.W.; Lin, C.H. Effects of virtual reality-augmented balance training on sensory organization and attentional demand for postural control in people with Parkinson disease: A randomized controlled trial. Phys. Ther. 2011, 91, 862–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez, P.; Moral, J.A.; Casado, E.; Salazar, A.; Lucena, D. Effects of virtual reality on balance and gait in stroke: A systematic review and meta-analysis. Rev. Neurol. 2019, 69, 223–234. [Google Scholar] [CrossRef]
- Peñasco, B.; De Los Reyes, A.; Gil, Á.; Bernal, A.; Pérez, B.; De La Peña, A.I. Application of virtual reality in the motor aspects of neurorehabilitation. Rev. Neurol. 2010, 51, 481–488. [Google Scholar]
- Robles, V. Virtual reality as a tool in physiotherapy: Fiction or reality? Fisioterapia 2018, 40, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Ferreira dos Santos, L.; Christ, O.; Mate, K.; Schmidt, H.; Krüger, J.; Dohle, C. Movement visualisation in virtual reality rehabilitation of the lower limb: A systematic review. BioMed. Eng. OnLine 2016, 15, 144. [Google Scholar] [CrossRef] [Green Version]
- Vavoda, J.T. Virtual Humanoids and Presence in Virtual Environments. Ph.D. Thesis, Fakultät für Mathematik, Informatik und Naturwissenschaften, Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, Germany, 2007. [Google Scholar]
- Bayón, M.; Martínez, J. Rehabilitación Del Ictus Mediante Realidad Virtual. Rehabilitación 2010, 44, 256–260. Available online: https://www.sciencedirect.com/science/article/pii/S0048712010000514 (accessed on 15 May 2023). [CrossRef]
- Iacoboni, M.; Woods, R.P.; Brass, M.; Bekkering, H.; Mazziotta, J.C.; Rizzolatti, G. Cortical mechanism of human imitations. Science 1999, 286, 2526–2528. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Torres-Narváez, M.; Sánchez-Romero, J.; Pérez-Viatela, A.; Betancu, E.; Villamil-Ballesteros, J.; Valero-Sánchez, K. Entrenamiento motor en el continuo de la realidad a la virtualidad. Fac. Med. 2018, 66, 117–123. [Google Scholar] [CrossRef]
- Schultheis, M.T.; Rizzo, A.A. The application of virtual reality technology in rehabilitation. Rehabil. Psychol. 2001, 46, 296–311. [Google Scholar] [CrossRef]
- Bailenson, J.; Patel, K.; Nielsen, A.; Bajscy, R.; Jung, S.-H.; Kurillo, G. The Effect of Interactivity on Learning Physical Actions in Virtual Reality. Med. Psychol. 2008, 11, 354–376. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.C.; Wang, H.K.; Wu, R.M.; Lo, C.S.; Lin, K.H. Home-based virtual reality balance training and conventional balance training in Parkinson’s disease: A randomized controlled trial. J. Formos. Med. Assoc. 2016, 115, 734–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, B.; Catalá, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Dockx, K.; Bekkers, E.M.; Van den Bergh, V.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 12, CD010760. [Google Scholar] [CrossRef]
- Lei, C.; Sunzi, K.; Dai, F.; Liu, X.; Wang, Y.; Zhang, B.; He, L.; Ju, M. Effects of virtual reality rehabilitation training on gait and balance in patients with Parkinson’s disease: A systematic review. PloS ONE 2019, 14, e0224819. [Google Scholar] [CrossRef] [Green Version]
- PEDro Scale (Escala PEDro). Available online: http://www.pedro.org.au/spanish/downloads/pedro-scale/ (accessed on 15 February 2023).
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Assessing risk of bias in included studies. In Cochrane Handbook of Systematic Review of Interventions, Version 510; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Mirelman, A.; Maidan, I.; Herman, T.; Deutsch, J.E.; Giladi, N.; Hausdorff, J.M. Virtual reality for gait training: Can it induce motor learning to enhance complex walking and reduce fall risk in patients with Parkinson’s disease? J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Loureiro, A.P.C.; Ribas, C.G.; Zotz, T.G.G.; Chen, R.; Ribas, F. Feasibility of virtual therapy in rehabilitation of Parkinson’s disease patients: Pilot study. Fisioter. Mov. 2012, 25, 659–666. [Google Scholar] [CrossRef]
- Pompeu, J.E.; Arduini, L.A.; Botelho, A.R.; Fonseca, M.B.F.; Pompeu, S.M.A.A.; Torriani-Pasin, C.; Deutsch, J.E. Feasibility, safety and outcomes of playing Kinect Adventures!TM for people with Parkinson’s disease: A pilot study. Physiotherapy 2014, 100, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Palacios, G.; García, I.; Ramos, P. A Kinect-Based System for Lower Limb Rehabilitation in Parkinson’s Disease Patients: A Pilot Study. J. Med. Syst. 2015, 39, 103. [Google Scholar] [CrossRef]
- Lee, N.Y.; Lee, D.K.; Song, H.S. Effect of virtual reality dance exercise on the balance, activities of daily living, And depressive disorder status of Parkinson’s disease patients. J. Phys. Ther. Sci. 2015, 27, 145–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Y.Y.; Yang, Y.R.; Cheng, S.J.; Wu, Y.R.; Fuh, J.L.; Wang, R.Y. Virtual Reality-Based Training to Improve Obstacle-Crossing Performance and Dynamic Balance in Patients With Parkinson’s Disease. Neurorehabilit. Neural Repair. 2015, 29, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.Y.; Yang, Y.R.; Wu, Y.R.; Wang, R.Y. Virtual Reality-Based Wii Fit Training in Improving Muscle Strength, Sensory Integration Ability, and Walking Abilities in Patients with Parkinson’s Disease: A Randomized Control Trial. Int. J. Gerontol. 2015, 9, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.; Geroin, C.; Dimitrova, E.; Boldrini, P.; Waldner, A.; Bonadiman, S.; Picelli, A.; Regazzo, S.; Stirbu, E.; Primon, D.; et al. Virtual Reality Telerehabilitation for Postural Instability in Parkinson’s Disease: A Multicenter, Single-Blind, Randomized, Controlled Trial. Biomed. Res. Int. 2017, 2017, 7962826. [Google Scholar] [CrossRef] [Green Version]
- Ferraz, D.D.; Trippo, K.V.; Duarte, G.P.; Neto, M.G.; Bernardes, K.O.; Filho, J.O. The Effects of Functional Training, Bicycle Exercise, and Exergaming on Walking Capacity of Elderly Patients With Parkinson Disease: A Pilot Randomized Controlled Single-blinded Trial. Arch. Phys. Med. Rehabil. 2018, 99, 826–833. [Google Scholar] [CrossRef]
- Feng, H.; Li, C.; Liu, J.; Wang, L.; Ma, J.; Li, G.; Gan, L.; Shang, X.; Wu, Z. Virtual reality rehabilitation versus conventional physical therapy for improving balance and gait in parkinson’s disease patients: A randomized controlled trial. Med. Sci. Monit. 2019, 25, 4186–4192. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Cimino, V.; Buda, A.; Paladina, G.; Di Lorenzo, G.; Manuli, A.; Milardi, D.; Bramanti, P.; Bramanti, A. Improving motor performance in Parkinson’s disease: A preliminary study on the promising use of the computer assisted virtual reality environment (CAREN). Neurol. Sci. 2020, 41, 933–941. [Google Scholar] [CrossRef]
- Yuan, R.Y.; Chen, S.C.; Peng, C.W.; Lin, Y.N.; Chang, Y.T.; Lai, C.H. Effects of interactive video-game-based exercise on balance in older adults with mild-to-moderate Parkinson’s disease. J. Neuroeng. Rehabil. 2020, 17, 91. [Google Scholar] [CrossRef]
- Pazzaglia, C.; Imbimbo, I.; Tranchita, E.; Minganti, C.; Ricciardi, D.; Monaco, R.L.; Parisi, A.; Padua, L. Comparison of virtual reality rehabilitation and conventional rehabilitation in Parkinson’s disease: A randomised controlled trial. Physiotherapy 2020, 106, 36–42. [Google Scholar] [CrossRef]
- Brachman, A.; Marszałek, W.; Kamieniarz, A.; Michalska, J.; Pawłowski, M.; Juras, G. Biomechanical measures of balance after balance-based exergaming training dedicated for patients with Parkinson’s disease. Gait Posture 2021, 87, 170–176. [Google Scholar] [CrossRef]
- Maranesi, E.; Casoni, E.; Baldoni, R.; Barboni, I.; Rinaldi, N.; Tramontana, B.; Amabili, G.; Benadduci, M.; Barbarossa, F.; Luzi, R.; et al. The Effect of Non-Immersive Virtual Reality Exergames versus Traditional Physiotherapy in Parkinson’s Disease Older Patients: Preliminary Results from a Randomized-Controlled Trial. Int. J. Environ. Res. Public Health 2022, 10, 14818. [Google Scholar] [CrossRef]
- Kashif, M.; Ahmad, A.; Bandpei, M.A.M.; Gilani, S.A.; Hanif, A.; Iram, H. Combined effects of virtual reality techniques and motor imagery on balance, motor function and activities of daily living in patients with Parkinson’s disease: A randomized controlled trial. BMC Geriatr. 2022, 30, 381. [Google Scholar] [CrossRef]
- Hong, Z.M.; Qiu, J.F.; Zhang, S.Q.; Wang, Y.B.; He, K.L.; Ma, R.J. Jiao’s scalp acupuncture combined with virtual reality rehabilitation training for motor dysfunction in patients with Parkinson’s disease: A randomized controlled trial. Zhongguo Zhen Jiu 2022, 12, 726–730. [Google Scholar] [CrossRef]
- Canning, C.G.; Allen, N.E.; Nackaerts, E.; Paul, S.S.; Nieuwboer, A.; Gilat, M. Virtual reality in research and rehabilitation of gait and balance in Parkinson disease. Nat. Rev. Neurol. 2020, 16, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.C. A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Human. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Ikbali Afsar, S.; Mirzayev, I.; Umit Yemisci, O.; Cosar Saracgil, S.N. Virtual Reality in Upper Extremity Rehabilitation of Stroke Patients: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2018, 27, 3473–3478. [Google Scholar] [CrossRef]
- Lloréns, R.; Noé, E.; Colomer, C.; Alcañiz, M. Effectiveness, usability, and cost-benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 418–425.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sá, M.J. Exercise therapy and multiple sclerosis: A systematic review. J. Neurol. 2014, 261, 1651–1661. [Google Scholar] [CrossRef]
- Truijen, S.; Abdullahi, A.; Bijsterbosch, D.; van Zoest, E.; Conijn, M.; Wang, Y.; Struyf, N.; Saeys, W. Effect of home-based virtual reality training and telerehabilitation on balance in individuals with Parkinson disease, multiple sclerosis, and stroke: A systematic review and meta-analysis. Neurol. Sci. 2022, 43, 2995–3006. [Google Scholar] [CrossRef]
- Peñasco-Martín, B.; De los Reyes-Guzmán, A.; Gil-Agudo, A.; Bernal-Sahún, A.; Pérez-Aguilar, B.; De la Peña-González, A.I. Aplicación de la realidad virtual en los aspectos motores de la neurorrehabilitación. Rev. Neurol. 2010, 51, 481–488. [Google Scholar] [CrossRef]
- Abbas, R.L.; Cooreman, D.; Al Sultan, H.; El Nayal, M.; Saab, I.M.; El Khatib, A. The Effect of Adding Virtual Reality Training on Traditional Exercise Program on Balance and Gait in Unilateral, Traumatic Lower Limb Amputee. Games Health J. 2021, 10, 50–56, Erratum in: Games Health J. 2021, 10, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Tack, C. Virtual reality and chronic low back pain. Disabil. Rehabil. Assist. Technol. 2021, 16, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Bond, S.; Laddu, D.R.; Ozemek, C.; Lavie, C.J.; Arena, R. Exergaming and Virtual Reality for Health: Implications for Cardiac Rehabilitation. Curr. Probl. Cardiol. 2021, 46, 100472. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Syntax Adopted |
|---|---|
| PubMed | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| Cochrane | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| Dialnet | ‘Enfermedad de Parkinson Y realidad virtual Y marcha Y equilibrio’; ‘Enfermedad de Parkinson Y realidad virtual Y Fisioterapia’; ‘Enfermedad de Parkinson Y realidad virtual Y fisioterapia’. |
| Scopus | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| Web of Science | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| PsycINFO | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| Science Direct | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| PEDro (Physiotherapy Evidence Database) | ‘Parkinson’s Disease AND virtual reality AND gait AND balance’; ‘Parkinson’s disease AND virtual reality AND Physical therapy’; ‘Parkinson’s disease AND virtual reality AND physiotherapy’. |
| Authors | Sample, Gender, and Mean Age | Type of Study and Intervention | Treatment and Follow-up Period | Console Type | Assessment Tools | Results |
|---|---|---|---|---|---|---|
| Mirelman et al., 2011 [32] |
|
| Treatment setting not specified. Intervention.
|
| 6MWT: assessing resistance GaitRite mat: quantified gait characteristics (stride, stride length, and obstacle clearance), Accelerometer (stride time, quantifying time measurements), Motor part UPDRS (Part III) | Gait speed increased by 8.9%, improved gait length and stride time, and remained on track. Walking plus numerical subtraction, significant improvement in stride length and stride time p = 0.016, and improvement in gait variability. 6MWT: improved after training and maintained at follow-up and after training. Obstacle Negotiation: significantly improved speed, gait speed during the 6-m test, and habitual gait speed. |
| Yen et al., 2011 [14] |
|
| Treatment setting not specified. Intervention.
| Balanced Training System
| SOT: 3 sensory systems (visual, somatosensory, and vestibular) in six categories were assessed. Sensory relationships were measured by computerised dynamic posturography (SMART Balance Master). | Pre-training: balance tests with no significant differences. After training: no significant differences between VR and conventional treatment with respect to balance. Better balance in SOT-6 of the VR compared to the conventional treatment (after follow-up this improvement was not significant). Balance training with VR significantly improved the capacity for sensory integration VR group as well as the Conventional treatment group improved in 1 SOT condition. In summary, both VR training and conventional training are beneficial for balance improvement. |
| Loureiro et al., 2012 [33] |
|
| Treatment setting not specified Intervention.
| Wii fit plus balance board | Borg scale: to establish the relationship between perceived exertion and external load or stress data. BBS TUG | BBS: Significant change from baseline. TUG: not statistically significant changes when compared to the baseline data. |
| Pompeu et al., 2014 [34] |
|
| Treatment setting not specified. Intervention.
| Kinect Adventures four games (space pop, 20,000 escapes, reflexion ridge and river rush). | Body function: 6-MWT Balance Evaluation System Test (BESTest) (DGI) | All participants improved their performance in the four games.
|
| Palacios-Navarro et al., 2015 [35] |
|
| The treatment was carried out at the rehabilitation centre. Intervention:
|
| 10 metre walk test (10MWT) at the beginning and at the end (maximum speed). All subjects were taking medication and were in ON PHASE. | Throughout the sessions, there were overall improvements in completion time and in the 10MWT clinical scale p = 0.002. |
| Lee et al., 2015 [36] |
|
| Treatment setting not specified. Intervention.
| Wii video games The virtual reality dance exercise used the K-Pop Dance Festival (Nintendo Inc., Japan) game for the Wii (Nintendo Inc., Japan) video game system. Songs liked by patients were selected from the various categories of K-Pop music included in the software. A strap was used to fix the remote control to the hands, and the patients tried to mimic the characters on the TV monitor. When subjects properly mimicked the movement, they felt vibrations from the remote control and heard the word ‘perfect’ broadcast by the TV speaker. | BBS (Balance) Modified Barthel Index (ADL) | Balance: after 6 weeks of treatment balance significantly improved in the EG from 46 to 48.1. In the CG no significant improvement from 45 to 45.4 ADL: changes in ADL had significantly improved in the EG and not in the CG. |
| Liao et al., 2015 [37] |
|
| Treatment setting not specified. Intervention.
The day before the intervention; day after the intervention and 30 days after the intervention. |
| Primary outcome measures: obstacle crossing performance and dynamic balance (stride length, cross stride speed and vertical clearance and dynamic balance using the LoS-limits of stability test). Secondary outcome measures: SOT; FES-1, TUG | Initial assessment: there were no significant differences between the initial results. Hurdle crossing results: EG (RV): improvements in stride length and stride speed over CG and no differences between EG(VR) and EG (traditional exercise). Balance test and SOT: EG (traditional exercise) and EG (VR): significant improvements over CG. EG(VR): improvements in forward movement in post-training, tracking and lateral movement. TUG: EG (VR) and EG (traditional exercise): significant improvement over GG after training and follow-up. |
| Liao et al., 2015 [38] |
|
| Treatment setting not specified Intervention.
| Nintendo Wii and balance board.
| Level walking performance. The GAITRite system (E-T variables: Gait speed and stride length). Functional gait performance Assessment (FGA): ability to modify gait to the task. Muscle strength: hand dynamometer with maximum force for 5 s. SOT: Sensory integration ability | Pre-intervention: there were no significant differences between the groups. Post intervention: Walking skills: VR Wii and Traditional Exercise groups showed significant improvements in gait, length, speed, and FGA compared to the CG. At post intervention and follow-up measurements, there were no significant differences between VR and Traditional exercise groups. Muscle strength: significant differences compared to GC but not between VR Wii and TE. SOT: Significant differences with respect to CG and also significant improvements of EG VR vs. EG traditional exercise at post and follow up. |
| Yang et al., 2016 [27] |
|
| Treatment setting not specified. Intervention.
| Micro-Star International Co. a wireless balance board.
| BBS DGI TUG Unified Parkinson’s rating scale motor score | BBS and DGI were significantly higher than in the initial tests of both VR and CG. Significant improvement in the TUG test in both groups. In summary, both CG and EG with VR showed improvement in balance and gait after training and follow-up. No difference found between VR balance training at home and conventional balance training at home. |
| Gandolfi et al., 2017 [39] |
|
| Treatment setting not specified. Intervention.
Before the intervention, after the intervention and at one month of follow up. | Nintendo Wii with Wii Fit game system and balance board. | BBS ABC 10-MWT for gait speed DGI | Both groups showed a significant overall improvement as measured by ABC scale, 10-MWT, DGI. Improved static and dynamic postural control in EG VR at home. Improvements in mobility and dynamic balance in EG SI. EG SI was more effective than Tele Wii in DGI after training. |
| Domínguez-Ferraz et al., 2018 [40] |
|
| Treatment setting not specified. Intervention.
| Xbox 360 Kinect Adventures video game. | Primary outcome measures:
| All groups showed significant improvements in 6MWT, SST. Only G3 showed significant improvement in gait speed at 10MWT. |
| Feng et al., 2019 [41] |
|
| Treatment setting not specified Intervention.
pre and post intervention | It does not specify the device used to apply the VR treatment. | BBS TUG UPDRS FGA | BBS, TUG and FGA scores were significantly improved in both groups (p < 0.05). BBS, TUG and UPDRS were significantly (p < 0.05) better in EG. There was no significant difference in UPDRS3 between the pre- and post-rehabilitation data of the control group (p < 0.05). |
| Calabró et al., 2020 [42] |
|
| Treatment setting not specified. Consecutively screening of the outpatients with PD who attended the Behavioral and Robotic Neuro-rehabilitation Laboratory of the IRCCS Neurolesi between August 2017 and October 2018. Intervention.
| CAREN SYSTEM. Consists of a motion capture system and a base platform driven by hydraulic and mechanical actuators (i.e., a 6–DOF motion platform and built-in instrumented treadmill). The movement of the platform is either driven by the subject’s movements or pre-programmed in synchrony with function curves (that define a specific pathway in the virtual environment). The platform’s movement is synchronized with the visual stimulus (e.g., the platform elevates when the subject arrives at a bump on the screen; the platform tilts accordingly when the road tilts). | Primary outcome measures: BBS; TUG. Secondary outcome measures: MDS-UPDRS II; and III 2. 10 MWT. Instrumental gait analysis with an accelerometer at lumbar level quantifying: (gait cycle length, stride length, gait cycle duration). | Significant improvement in each clinical outcome measure; however, at T2 they returned to baseline results. EG VR: At T4 the improvement in clinical outcome was maintained after the 3-month follow-up. CAREN training slightly shortened the duration of the gait cycle (p = 0.04), most evidently the swing phase (p = 0.04), increased gait speed (p = 0.001) stride length (p = 0.02) and percentage of single limb support (p < 0.001) and reduced stride width (p < 0.001) and cadence (p = 0.01). |
| Yuan et al., 2020 [43] |
|
| Treatment setting not specified Intervention.
At 6 weeks and at 12 weeks. | IVGB SYSTEM The IVGB system was developed by modifying the XaviX entertainment system. The IVGB exercise program consisted of two tasks: a multi-directional step task and a target-directed stepping task. The IVGB system offers aural and visual feedback in both tasks to increase participants’ attention. | Primary outcome measures: BBS Secondary outcome measures: MSL test. Walking ability and indicator of mobility function and risk of falls. |
MSL test: Group B higher at week 12 than initially. BBS and two MSL scales were significantly different between the two groups at 6 weeks. A 6-week IVGB training significantly improved balance ability and MSL in left, right and backward directions in group B patients. IVGB: virtual reality tasks improved motor coordination and the ability to stand on one leg. |
| Pazzaglia et al., 2020 [44] |
|
| Treatment setting not specified. Duration of the programme: 6 consecutive weeks. Each session 40 min 3 times per week. |
| BBS: to measure balance. Secondary outcome measures: DGI: to evaluate the ability to adapt gait to complex walking tasks. DAHS questionnaire: to measure performance of the upper limb. SF-36 questionnaire: to evaluate quality of life. | Patients in the EG showed better balance and gait outcomes BBS p = 0.003:
|
| Tunur et al., 2020 [8] |
|
| Treatment setting not specified. Intervention.
| Google Glass All applications and features normally found in Google Glass were removed for this study to prevent personal information from being collected. The Google Glass were defaulted to an offline environment that only contained the MTG modules. The MTG was voice-activated using the prompt ‘OK Glass’, followed by choosing the preferred MTG module from the list of four MTG modules: Warm Me Up; Balance Me; Unfreeze Me; Walk with Me. The participants could use voice-activated commands, or swipe and tap the control bar to navigate through the menu. Each of the first three modules have three or four different movement variations, averaging approximately 45 s per video. |
|
|
| Brachman et al., 2021 [45] | N = 24 patients with PD EG: 12 Mean age 69.5 ± 7.2 Sex: 8 males and 4 females. EC: 12 Mean age 65.3 ± 9.2 Sex: 7 males and 5 females | RCT EG: was trained with a custom made exergaming balance-based training system. CG: a conventional balance training. | Treatment setting: A Virtual Reality scenario was projected on the 65-inch screen situated 2 m away in front of the participant. Intervention: 12 balance-based exergaming training sessions; 3 sessions per week using the exergaming balance training system. Each training lasted for 30 min. Participants in the control group received 12 training sessions (3 sessions per week) of the conventional balance rehabilitation. Evaluation
| The VR system included two integrated devices, a Kinect sensor system and a custom made force platform. Patients were introduced inside the video game as an avatar character which provided instantaneous visual feedback about participants’ performance. In each training session patients practiced maintaining static posture, leaning in different directions, dynamic weight shifting, gait initiation, step making and trunk rotation. | All measurements were performed on a force platform, which was part of a VR-based balance system. Postural stability: Quiet Standing Eyes Open. Quiet Standing Eyes Closed. Dynamic balance: FBT LOS | After training, participants in both groups showed significantly better results in static balance performance. However, only exergaming training significantly improved LOS performance (higher values of Range of forward lean (p = 0.039, dz = 0.67) and leaning rate (p = 0.007, dz = 0.96). Also FBT test improved significantly only in experimental group (decrease in time to target hit (p = 0.02, dz = 0.76) and significant increase in average COP velocity (p = 0.008, dz = 0.93). |
| Maranesi et al., 2022 [46] | N = 30 patients with PD EG: 16 Mean age: 72.7 ± 6.3 Sex: 6 males and 10 females CG: 14 Mean age: 75.1 ± 5.4 Sex: 9 males and 5 females | RCT preliminary result. EG: technological Rehabilitation. CG: traditional rehabilitation. | A 10-sessions training was conducted, divided into 2 sessions per week, for 5 weeks. CG performed traditional therapy sessions lasting 50 min each. EG: The technological intervention group carried out 30 min of traditional therapy and 20 min of treatment. Traditional rehabilitation treatments, consisting of breathing and relaxation, task-oriented exercise to improve strength and to reduce limitations in the activities of daily living, walking with cues to reduce gait deficit, stretching to relieve muscle and joint stiffness, static and dynamic balance training to reduce postural control impairments, flexibility exercises to improve the range of motion of different joint, unilateral and contralateral coordination exercises performed in bed and while standing, involving 4 limbs. Evaluation
| Tymo® system: a wireless platform that provides non-immersive virtual reality exergames, which can be adapted to each patient according to the functional capacity, in order to improve balance and postural control; the system offers a number of therapy games from Verena Schweizer’s neuro-training | CDR PIADS BI SF-12 FES-I Gait and balance performance on Tinetti’s POMA | There was an improvement in balance at the end of treatments in both groups (CG: 12.4 ± 0.7 vs. 13.5 ± 0.8, p = 0.017; TG: 13.8 ± 0.5 vs. 14.7 ± 0.4, p = 0.004). The overall risk of falls was significantly reduced only in the experimental technology rehabilitation group (POMA Total: 24.6 ± 0.9 vs. 25.9 ± 0.7, p = 0.010). All POMA scores differed statistically significantly in the EG, highlighting the improvement not only in balance but also in gait characteristics (9.7 ± 0.8 vs. 11.4 ± 0.2, p = 0.003). There was also an improvement in the psychological sphere in the EG, measured through the MSC-(17.1 ± 0.4 vs. 16.5 ± 0.4, p = 0.034). |
| Kashif et al., 2022 [47] | N = 44 patients with idiopathic PD EG; 22 Mean age: 63.86 ± 4.57 Sex: 13 male and 9 female CG: 22 Mean age: 62.32 ± 4.61 Sex: 12 male and 10 female | RCT EG: routine physical therapy along with VR and MI techniques CG: routine physical therapy (warm-up, stretching, strengthening, and relaxation exercises, limb coordination exercises, trunk, neck, and gait training), | For safety purposes, the patients stood inside parallel bars on the Wii Fit board with their shoes of EG received 60-min sessions: 40-minroutine physical therapy as in EC; 10–15 min of VR; and 5–10 min of MI techniques. Every other day (three days a week) for 12 weeks, CG received 40-min sessions and 20 min of walking and cycling, with a short rest period every other day (three days a week) for 12 weeks. Evaluation:
| The VR system consisted of a wall-mounted display, a Wii box, a Wii remote, and a Wii Fit board. The patients were instructed to stand on Wii Fit board while interacting with the VR system and playing the selected games. The games were of motor functionality, balance and ADL. The last 5–10 min of the session comprised the MI. Consisted of watching the recorded videos, analyzing the differences in both videos, and the differences in both videos. In the next step, they were instructed to relax and concentrate on their calm breathing patterns. To finish by performing the activities, they were given verbal commands whenever necessary. | Motor Function UPDRS-part III. Balance confidence ABCS. BBS ADL UPDRS-part II | The experimental group showed a more significant improvement in motor function than the control group on UPDRS part III, with 32.45 ± 3.98 vs. 31.86 ± 4.62 before and 15.05 ± 7.16 vs. 25.52 ± 7.36 at 12 weeks, and p-value < 0.001. At 12 weeks, the BBS scores of the experimental group improved from 38.95 ± 3.23 to 51.36 ± 2.83, with a p-value < 0.001. At 12 weeks, the experimental group’s balance confidence improved significantly, from 59.26 ± 5.87 to 81.01 ± 6.14, with a p-value < 0.001. The ADL scores of the experimental group also improved, going from 22.00 ± 4.64 to 13.07 ± 4.005 after 12 weeks, with a p-value < 0.001. |
| Hong et al., 2022 [48] | N = 52 patients with PD EG: 26 CG: 26 | CG: Routine basic treatment and VR rehabilitation training. EG: Same as control group but added Jiao scalp acupuncture. Scalp points included movement area, balance area, and dance tremor control area. | Both groups were treated once a day, 5 times a week, for a total of 8 weeks. | It does not specify the device used to apply the VR treatment. | The gait parameters (step distance, step width, step speed, and step frequency). Timed ‘up-and-go’ test. Unified Parkinson’s disease rating scale part Ⅲ (UPDRS-Ⅲ) | Four weeks into treatment:
|
| Study | Criteria | Score | Result | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Mirelman et al., 2011 [32] | N | N | N | N | N | N | N | Y | Y | N | Y | 3 | POOR |
| Yen et al., 2011 [14] | N | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Loureiro et al., 2012 [33] | Y | N | N | Y | N | N | N | Y | N | Y | N | 3 | POOR |
| Pompeu et al., 2014 [34] | Y | N | N | Y | N | N | Y | Y | Y | N | Y | 5 | FAIR |
| Palacios-Navarro et al., 2015 [35] | N | N | N | Y | N | N | N | Y | Y | N | Y | 4 | FAIR |
| Lee et al., 2015 [36] | N | Y | N | Y | N | N | N | N | N | Y | Y | 4 | FAIR |
| Liao et al., 2015 [37] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | GOOD |
| Liao et al., 2015 [38] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | GOOD |
| Yang et al., 2016 [26] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Gandolfi et al., 2017 [39] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 | GOOD |
| Domínguez-Ferraz et al., 2018 [40] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | GOOD |
| Feng et al., 2019 [41] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Calabró et al., 2019 [42] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 | FAIR |
| Yuan et al., 2020 [43] | Y | Y | N | N | N | N | N | N | N | V | Y | 3 | POOR |
| Pazzaglia et al., 2020 [44] | N | Y | N | Y | N | N | Y | N | N | Y | Y | 5 | FAIR |
| Tunur et al., 2020 [8] | Y | N | N | N | N | N | Y | Y | Y | N | N | 3 | POOR |
| Brachman et al., 2021, [45] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Maranesi et al., 2022 [46] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Kashif et al., 2022 [47] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
| Hong et al., 2022 [48] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 | GOOD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Mansilla, J.; Bedmar-Vargas, C.; Garrido-Ardila, E.M.; Torres-Piles, S.T.; González-Sánchez, B.; Rodríguez-Domínguez, M.T.; Ramírez-Durán, M.V.; Jiménez-Palomares, M. Effects of Virtual Reality in the Rehabilitation of Parkinson’s Disease: A Systematic Review. J. Clin. Med. 2023, 12, 4896. https://doi.org/10.3390/jcm12154896
Rodríguez-Mansilla J, Bedmar-Vargas C, Garrido-Ardila EM, Torres-Piles ST, González-Sánchez B, Rodríguez-Domínguez MT, Ramírez-Durán MV, Jiménez-Palomares M. Effects of Virtual Reality in the Rehabilitation of Parkinson’s Disease: A Systematic Review. Journal of Clinical Medicine. 2023; 12(15):4896. https://doi.org/10.3390/jcm12154896
Chicago/Turabian StyleRodríguez-Mansilla, Juan, Celia Bedmar-Vargas, Elisa María Garrido-Ardila, Silvia Teresa Torres-Piles, Blanca González-Sánchez, María Trinidad Rodríguez-Domínguez, María Valle Ramírez-Durán, and María Jiménez-Palomares. 2023. "Effects of Virtual Reality in the Rehabilitation of Parkinson’s Disease: A Systematic Review" Journal of Clinical Medicine 12, no. 15: 4896. https://doi.org/10.3390/jcm12154896